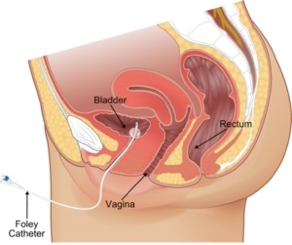
Urinary catheterization is the placement of any tube in the Bladder via urethra to drain or collect urine from the bladder, or to inject liquids used for treatment or diagnosis of bladder conditions.
Introduction
The ability to insert a urinary catheter is an essential skill in medicine.
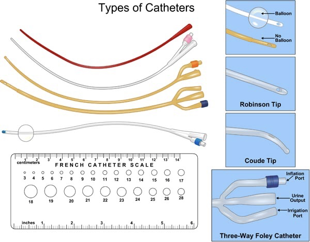
Catheters are sized in units called French, where one French equals 1/3 of 1 mm. Catheters vary from 12 (small) FR to 48 (large) FR, 3-16mm in size.
They also come in different varieties including ones with and without a bladder balloon, and ones with different sized balloons. – you should check how
much the balloon is made to hold when inflating the balloon with water!
Universal precautions
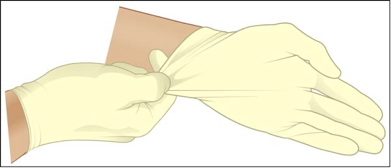
Gloves must be worn while starting the Foley, not only to protect the user but also to prevent infection in the patient. Trauma protocol calls for all team members to wear gloves, face and eye protection and gowns.

The potential for contact with a patient’s blood and/or body fluids while starting a catheter is present and increases with the inexperience of the operator.
Indications
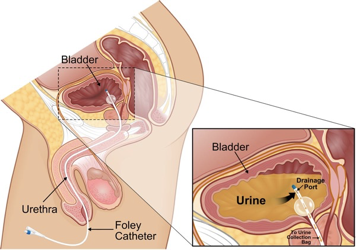
By inserting a Foley catheter you are gaining access to the bladder and its contents. Thus, enabling you to drain bladder contents, decompress the bladder, obtain a specimen and introduce a passage into the GU tract. Urinary output is also a sensitive indicator of volume status and renal perfusion (and thus tissue perfusion also).

In the emergency department catheters can be used to aid in the diagnosis of GU bleeding.
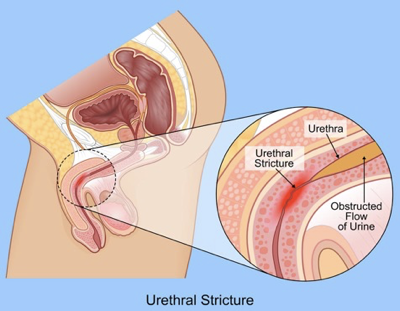
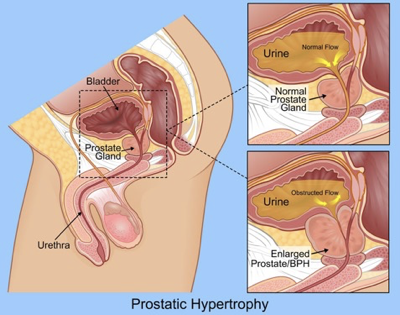
Common indications to catheterize a patient include: acute or chronic urinary retention (which can damage the kidneys), bladder outlet obstruction, orthopedic procedures that may limit a patient’s movement, the need for accurate monitoring of input and output (such as in an ICU), benign prostatic hyperplasia, incontinence, and the effects of various surgical interventions involving the bladder and prostate. In some cases, as in urethral stricture or prostatic hypertrophy, insertion will be difficult and early consultation with urology is essential.
Contraindications
Foley catheters are contraindicated in the presence of urethral trauma. Urethral injuries may occur in patients with multisystem injuries and pelvic factures, as well as straddle impacts.
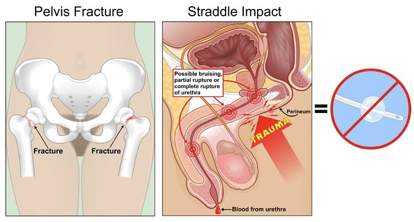
If this is suspected, one must perform a genital and rectal exam first. If one finds blood at the meatus [“mee-ey-tuh s”] of the urethra, a scrotal hematoma, a pelvic fracture or a high riding prostate, then a high suspicion of urethral tear is present. One must then perform retrograde urethrography (injecting 20 cc of contrast into the urethra).
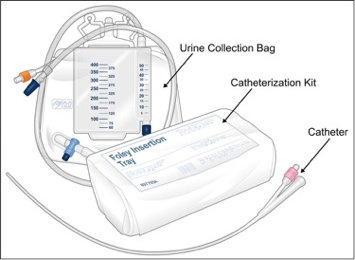
Catheterization Equipment
The following is a list of equipment commonly used during a urinary catheterization procedure:
Sterile gloves
Sterile drapes
Cleansing solution
Cotton swabs
Forceps
Sterile water (usually 10 cc)
Foley catheter (usually 16-18 French)
Syringe (usually 10 cc)
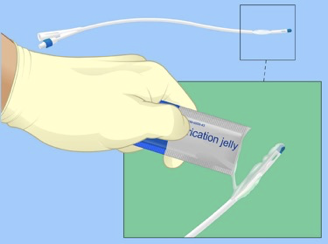
Lubricant (water based jelly or xylocaine jelly)
Collection bag and tubing

Procedure
Gather equipment.
Explain procedure to the patient

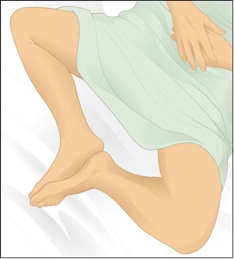
Assist patient into supine position with legs spread and feet together
Open catheterization kit and catheter
Prepare sterile field, apply sterile gloves
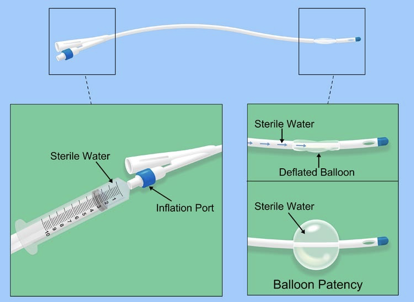
Check balloon for patency.
Generously coat the distal portion (2-5 cm) of the catheter with lubricant
Apply sterile drape
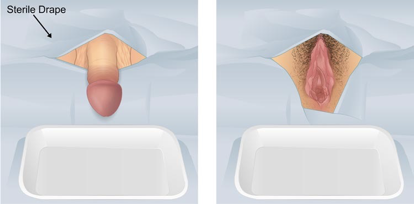
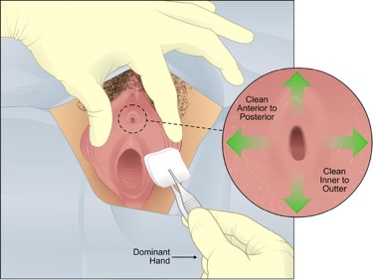
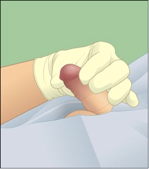
If female, separate labia using non-dominant hand. If male, hold the penis with the non-dominant hand. Maintain hand position until preparing to inflate balloon.
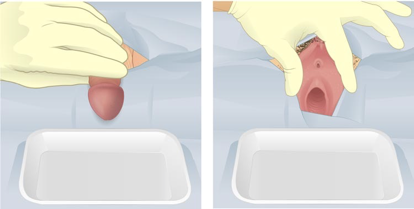
Using dominant hand to handle forceps, cleanse peri-urethral mucosa with cleansing solution. Cleanse anterior to posterior, inner to outer, one swipe per swab, discard swab away from sterile field.
Pick up catheter with gloved (and still sterile) dominant hand. Hold end of catheter loosely coiled in palm of dominant hand.

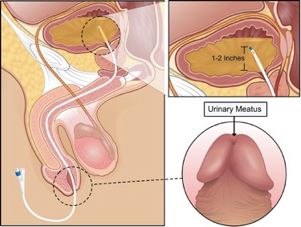
In the male, lift the penis to a position perpendicular to patient’s body and apply light upward traction (with non-dominant hand)
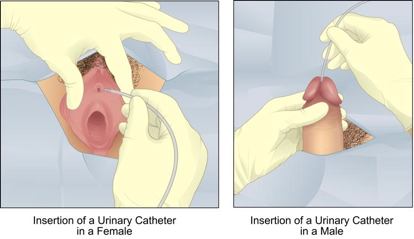
Identify the urinary meatus and gently insert until 1 to 2 inches beyond where urine is noted
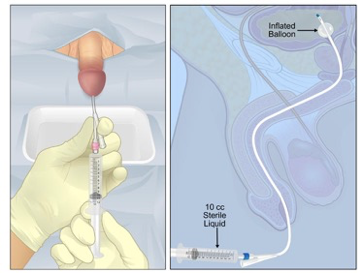
Inflate balloon, using correct amount of sterile liquid (usually 10 cc but check actual balloon size)
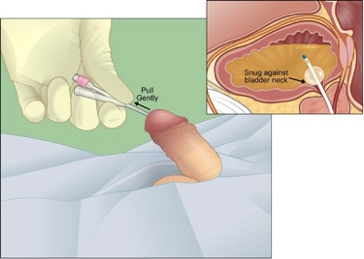
Gently pull catheter until inflation balloon is snug against bladder neck
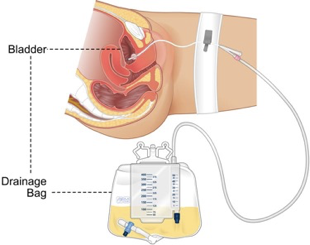
Connect catheter to drainage system
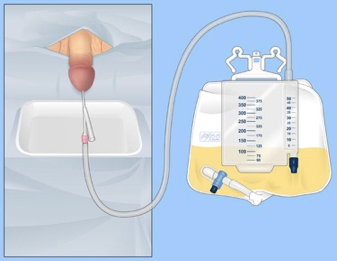
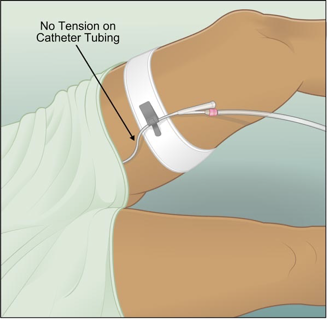
Secure catheter to abdomen or thigh, without tension on tubing
Place drainage bag below level of bladder
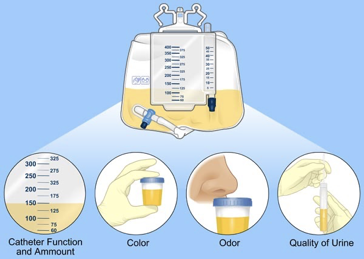
Evaluate catheter function and amount, color, odor, and quality of urine
Remove gloves, dispose of equipment appropriately, wash hands

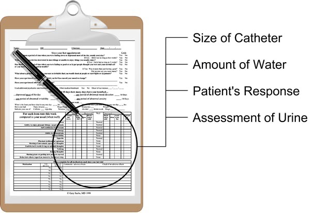
Document size of catheter inserted, amount of water in balloon, patient’s response to procedure, and assessment of urine
Complications
For some patients the insertion and removal of a catheter causes excruciating pain, so a topical anesthetic is used. Catheterization should be performed as a sterile medical procedure and should only be done by trained, qualified personnel, using equipment designed for this purpose, except in the case of intermittent self catheterization where the patient has been trained to perform the procedure themselves.
The main complications are tissue trauma and infection. After 48 hours of catheterization, most catheters are colonized with bacteria, thus leading to possible bacteruria [“bak-teer-ee-yoo r-ee-uh”] and its complications. Catheters can also cause renal inflammation, nephro-cysto-lithiasis, and pyelonephritis [“pahy-uh-loh-nuh-frahy-tis”] if left in for prolonged periods.
The most common short term complications are inability to insert catheter, and causation of tissue trauma during the insertion.
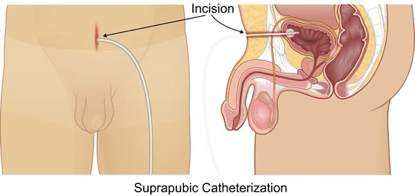
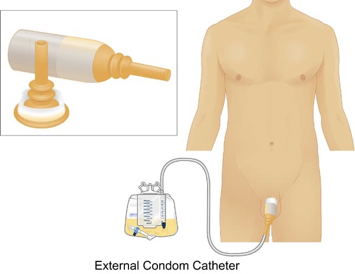
The alternatives to urethral catheterization include suprapubic catheterization and external condom catheters for longer durations.
Catheter Removal
With any insertion of a urinary catheter into a patient’s bladder, it is important to plan its removal as soon as possible. Whether this is a permanent removal, a scheduled catheter change, or an unplanned change due to complications; delayed removal may lead to damage to the bladder neck, encrustations and/or urinary infections.
Before beginning make sure the patient understands the procedure, explain any potential symptoms they may experience during and following removal of the catheter.
Check the patient’s records. Note amount of water inflated into the balloon.
Gather equipment: gloves, cleaning solution and the appropriate syringe (normally 10ml syringe for routine catheters).
Wash hands and put on gloves.
Place a container between patient’s legs to catch any urine spillage during removal.
Release any leg attachment system.
Attach syringe to the catheter valve and deflate the balloon. Do not pull on the syringe but allow the balloon contents to flow back on its own.
Ask the patient to relax and to take a deep breath. As the patient exhales, slowly and smoothly remove the catheter.
Inspect the catheter tip for pus, encrustation or damage.
Remove gloves and dispose of equipment.
Wash hands.
Record the date and time of removal. Encourage the patient to drink plenty of fluids and document urine output until frequency and volumes are satisfactory. Observe for any signs of voiding difficulties or if patient develops abdominal pain.