Description #
A discussion effective team management, briefings, debriefings and conflict resolution
Learning Objectives #
In this unit students will learn why teamwork breaks down and learn some techniques that will enable them to resolve conflict and manage there teams more effectively
Team management #
Team Management
Teamwork is an inherent part of healthcare; many tasks impose cognitive and physical demands that are too strenuous for one individual, and tasks in highly technical and specialized environments demand that different groups of professionals cooperate in order for a problem to be dealt with successfully. Aviation safety research indicates that poor crew coordination is major contributing factor in accidents. Since both aircrew and healthcare professionals share many work-related issues (time constraints, stress, fatigue, etc), strategies that have proven effective in aviation can also be applied to the healthcare field.
Poor teamwork is often caused by a lack of shared understanding about the necessity and function of teamwork. Conflicts can emerge between team members, causing a breakdown in communication and subsequent underutilization or misallocation of available resources. Team members can also be hesitant or fail to question the actions of other team members, even when serious concerns exist.
Barriers to effective teamwork
A team brings increases expertise, experience and cognitive resources to a given situation. Workload can also be handled more effectively. Still, teams are vulnerable to a number of threats, which can impact patient safety:
Unclear chain of authority: When there is no clear team leader, there will be less clear direction when it comes to acting. Tasks may go unfinished or not accomplished at all because everyone might think someone else will do it. Also, the possibility of risky decisions may increase because nobody will have to account for the outcome. Team leaders should also resist the temptation to become too ‘hands on’ with the patient, it is generally preferable that they monitor the overall situation, delegating tasks as necessary.
Different mental models: Members of a team made up form different disciplines may view a situation differently, based on their area of expertise. When this occurs, the sharing of information is vital if decisions based on incomplete information are to be avoided.
Poor communication skills: As we have seen, communicating effectively is very important when building and maintaining situational awareness. Poor communication can lead to a failure to announce intended tasks and/or reluctance to question assumptions or actions of others.
Peer pressure: When a majority of team members have formed an opinion, it can be very difficult to change their minds. Dissenting opinions may be seen as a threat to team cohesion and therefore dismissed. The danger is that options, which do not confirm the majority’s point of view will not be used in the decision-making process; once a treatment path has been chosen, the team becomes less flexible in their approach because nobody expresses doubts, asks questions, or looks for contradictory evidence.
Excessive deference to senior team members: It can be uncomfortable, difficult or even frowned upon to question the decisions or actions people higher up the hierarchy ladder. Nevertheless, patient safety should always be the top priority and every member of a team should be encouraged to speak up if they are concerned with a course of action. This is recognized as a contributing factor in many aviation accidents and is a major part of our human factors training. Techniques for doing this will be covered in the section on conflict management.
Strategies for improving teamwork
In 2000, the University of Texas conducted a study on the attitudes towards stress, fatigue and teamwork as they relate to job performance, using pilots and surgical staff as their subjects.
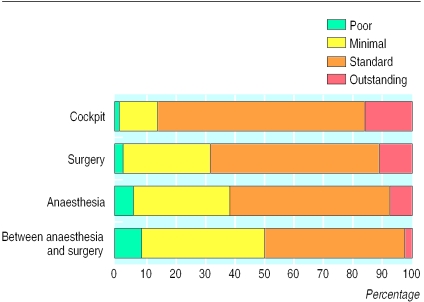
Quality of observed teamwork
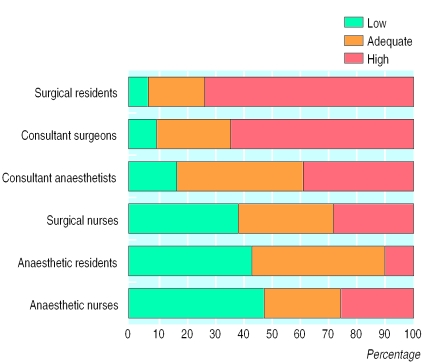
Assessment of quality of teamwork
The findings indicated that the quality of teamwork was higher in the cockpit than in the operating room, and that physicians tend to overrate the quality of their teamwork skills. This is not meant as an indictment of physicians’ competence; it is understandable for a number of reasons. First, human factors training and research in medicine is still relatively new; there is less data to work from and it takes time for attitudes to change. We must also consider that individual achievement is strongly encouraged in many cultures and educational systems, which can make effective teamwork challenging.
Team performance can be improved by applying as many of the following concepts as possible:
– Fostering a positive team climate
– Establishing clear team leadership
– Sharing the mental model
– Applying problem solving strategies when appropriate
– Sharing workload
– Monitoring other team members
– Improving team skills through training, briefing and debriefing
– Solving conflicts constructively
Resolving conflict
Conflicts are an integral part of working with others. Conflict is often though of as a personal disagreement with another person and while this is sometimes the case, form an operational standpoint, conflict is a difference of expectations.
It can be difficult question the decisions or actions of others, especially when dealing with superiors. Some may see it as questioning their competence or an erosion of their authority, especially in the presence of others. Subordinates may also fear repercussions on their job security, prospects for promotion and professional and/or personal reputation if they question the actions of superiors. In the end, it’s all about the patient; their safety should always be the top priority.
Passiveness or aggressiveness are not effective behaviors when it comes to resolving conflict. Being open, forthright, and respectful are the most important techniques when dealing with differences in expectations. Being appropriately assertive is an effective method for resolving conflict. You are being assertive when you state your opinion or position in a positive and direct manner.
The goal of assertiveness is to prompt other team members to diligently reconsider their point of view before a decision is made. People generally prefer to be convinced by facts, and not by the authority of the other, that a planned action is appropriate. Assertiveness is not aggressiveness; it involves communicating ones concerns, ideas and needs to others in a clear and direct manner, without being demeaning. Assertive statements suggest a sense of personal responsibility, as well as a sense of honesty and fairness.
Whenever you feel uncomfortable or concerned about a patient’s safety, challenge authority in a respectful, nonthreatening, and supportive way and make sure that critical information is addressed. Since it is nearly always awkward to question someone in authority, the following approach, developed by Transport Canada, may help to broach the issue in a constructive manner:
1) Opening: Get the person’s attention
2) Express concern
3) State the problem
4) Propose a solution
5) Get a decision and/or response
The following guidelines can also prove useful when managing conflict within a team:
– Focus on ‘what’s right’, not ‘who’s right’; the patient’s safety comes first!
– Gather the facts
– Use ‘I’ and ‘we’ statements
– If you state a problem, propose a solution
– Abandon your idea if the other is better
– Be assertive, as required
– If you are in doubt: Ask! Your only risk is pride
The importance of briefings
In both aviation and healthcare, good situational awareness and effective teamwork require a shared mental model of the situation or task, at hand. Ideally, this should be achieved before the start of the common task. In the aviation setting, briefings are an excellent way to ensure everyone is ‘on the same page’. Ideally, a briefing should cover the following:
– Team members, (names, roles)
– A review of the current situation
– Planned actions
– Contingencies
– Available resources
– Expectations for speaking up and sharing information
– Subtask allocation
– Any other information pertinent to the task at hand
The importance of debriefings
During a stressful, time-critical event, there may not enough time to resolve conflicts ‘on-the-fly’. Debriefings can be used to systematically address any conflicts that may have arisen during the event, review actions and procedures, clarify misunderstandings and answer questions from the team. The goal of the debriefing should be to learn as much as possible form an event in order to improve future performance. While it is important to conduct a debriefing following a negative event, conducting a debriefing following an event where everything went ‘right’ can be equally as useful; giving credit where credit is due helps build confidence in an individual and cohesion in a team. Feedback should be constructive, respectful, objective and precise. If possible, give genuinely positive feedback first; any critical issues will be accepted more readily. Embarrassing a team member should be avoided, feedback should address observable behavior, not characteristics of a person; problematic behavior should be dealt with in private.
Set a good example: Take feedback willingly and show gratitude for it; everybody can learn from feedback.
Conclusion
Teamwork management in a complex, dynamic setting such as front line health care poses special challenges because a team of experts does not always make an expert team. To be effective, team members must combine their ‘hard’ technical expertise with ‘soft’ skills such as communication, workload management and conflict resolution, all the while being conscious of how human factors such as fatigue and stress affect individual performance.
There is no single ‘best method’, when it comes to team management. Some teams function effectively using a flatter hierarchy, for others, a traditional authority structure is more appropriate. In either case, it is essential that there be open communication between all team members. Numerous studies in the aviation field have shown that crews who display good communication skills commit fewer errors, and are able to mitigate them more quickly when they do occur. Team leaders should solicit input from subordinates and they in turn should be ready to provide timely and relevant information anytime they feel patient safety is in question.
It should also be remembered that providing safe, effective health care is not a democratic process, negotiation, or popularity contest; team leaders will eventually have to make unpopular decisions if they judge it to be in the patient’s best interest. That said, the quality of any decision depends on the quality of information considered, therefore a climate of open, timely and respectful communication should be encouraged in any team setting.
Simulators are an excellent tool for developing good communication and teamwork management practices.