Description #
Overview of the standards of practice that should be implemented in facilities providing Procedural Sedation and Analgesia(PSA)to improve upon the quality of care and patient safety.
Learning Objectives #
At the end of the session the student will be able to:
a) Identify the recommended standards of practice and management of care for patients receiving Procedural Sedation and Analgesia(PSA)
b) Identify the core competencies, equipment, and supplies required for the safe and effective provision of PSA
Standards of Practice #
Professional nursing organizations (e.g. CRNBC) are instrumental in shaping nursing practice by developing standards of practice, education, ethical conduct and continuing competence. Unions, although primarily concerned with development of legally binding agreements that regulate salaries, working conditions and other contract negotiations also advocate for health and nursing policy related to e.g. scope of nursing practice. Professional organizations and unions have some common goals such as the welfare of members, improvement of working conditions and concern for professional ethics.
- From your clinical or educational experience, identify and an issue that concerns you and that you think requires a new or revised policy. Post it on the discussion board.
- As you read the concerns of your colleagues – propose a change/solution to the issue and post it on the discussion board.
INTRODUCTION
- The safe and effective provision of Procedural Sedation highlights the requirements for a broad base of knowledge and skills on the part of the practitioner
- In keeping with JCAHO’s recommendation that practice protocols be developed through a multidisciplinary approach, the following Standards of Practice are based on the guidelines established by the ASA (American Society of Anesthesiologists), JCAHO (Joint Commission on Accreditation of Healthcare Organizations) Canadian Society of gastroenterology Nurses and Associates, and the AORN (American Society of Operating Room Nurses)
- These guidelines will help identify the core competencies, equipment, and supplies required for the safe and effective provision of Procedural Sedation, thereby informing the Standards of Practice
- The Standards of Practice are used in conjunction with the institution’s Patient Care Guidelines
PATIENT EVALUATION
Practitioners should be familiar with sedation-oriented aspects of the patient’s medical history and how they might affect the response to sedation / analgesia.
These include:
- Major organ system abnormalities
- Previous adverse experience with sedation / analgesia / regional or general anesthesia
- Medications, allergies, and potential drug interactions
- Time and nature of last oral/gastric intake
- History of tobacco, alcohol, or drug abuse
- Relevant lab testing [e.g. bloodwork]
- Physical assessment and medical history
PRE-PROCEDURAL PREPARATION
• Informed consent is obtained from the patient or designate and includes the
benefits, risks, limitations, and alternatives to sedation / analgesia.
• Accompaniment home by a responsible adult post-procedure is confirmed for outpatient procedures.
• Gastric emptying [to reduce risk of vomiting and aspiration] is confirmed.
ASA Guidelines for healthy adults undergoing elective procedures:
NPO 6 hours since light meal; 2 hours since clear fluids
***The risk for aspiration [e.g. in emergencies or impaired gastric emptying]
must be considered in determining: the target level of sedation; whether the
procedure can be delayed; whether the trachea should be protected by
intubation.
Monitoring during PSA #
LEVEL OF CONSCIOUSNESS
The patient’s response to commands during the administration
of conscious / procedural sedation serves as a guide to their level of consciousness.
Monitoring level of consciousness reduces risks for sedation by allowing early detection
and treatment of adverse drug responses before sedation-related decompensation occurs.
PULMONARY VENTILATION
The primary causes of morbidity associated with sedation/ analgesia are drug-induced respiratory depression and airway obstruction (ASA Task Force). The risk of adverse outcomes associated with sedation / analgesia is reduced by monitoring ventilation through observation or auscultation; capnography may decrease
risk through apnea monitoring.
Ventilation and oxygenation are separate processes: monitoring oxygenation through
pulse oximetry is not a substitute for monitoring ventilation.
OXYGENATION
Oximetry effectively detects oxygen desaturation and hypoxemia,
decreasing the likelihood of progression to sedation-related decompensation.
HEMODYNAMICS
Sedation / analgesia may affect autonomic compensation by decreasing the natural response to hypovolemia and procedural stressors or, if inadequate, through harmful autonomic stress responses [e.g. hypertension, tachycardia]
Monitoring heart rate and blood pressure allows early detection of changes and appropriate intervention
LOC Monitor sedation / pain scale continuously and patient response to verbal commands [if appropriate] regularly (e.g. q 5-10 min)
SPO2
Continuous monitoring with appropriate alarms and, if available, the variable pitch ‘beep’ which gives audible indication of oxygen saturation
VITAL SIGNS
Monitor continuously:
- ECG
- Vital signs: BP, heart rate, respiratory rate and quality, SpO2
- LOC/ sedation / pain
- ETCO2 readings as required
ETCO2
- Where deep sedation is a probable or planned outcome
- Where moderate or dissociative sedation is a probable or planned outcome in any patient with an ASA classification status of 3 or above
- Where the respiratory rate assessment may be difficult due to procedural draping or positioning
- On occasion, procedural or patient factors may necessitate a modification of these monitoring guidelines [e.g. uncooperative / combative patients, procedural / positioning restrictions]
- Please refer to the following Guidelines for reference:
- VCH PSA ER Guideline CPD- 300
- VCH PSA General Guideline – CPD 400
ASSESSMENT/RECORDING OF VITAL SIGNS
At a minimum, assessment and recording should be:
- Before procedure begins
- Following administration of sedation / analgesia
- At regular intervals during the procedure -Q15 min until the discharge from Unit/Facility/Transfer Criteria are met Refer to Appendix A
- Q 5 min for patients in deep sedation
- Upon completion of procedure
- During initial recovery
The following vital signs should be recorded Q 5 minutes x 3 after initial and subsequent PSA doses and then Q15 minutes:
- BP
- Heart rate
- Respiratory rate
- Pulse oximetry
- LOC / sedation / pain
- ETCO2 readings as required
Availability of an individual responsible for patient monitoring #
STAFFING REQUIRED FOR PSA ADMINISTRATION
- A designated qualified individual (Dr., RN, or RT) other than the one performing the procedure must be present to monitor the patient receiving PSA
- During Procedural Sedation, this individual should have no other responsibilities that would leave the patient unattended or unmonitored; however, once the patient’s level of sedation is light or moderate and VS have stabilized, this individual may assist with minor, interruptible tasks
- If sedation level progresses to deep sedation, this monitoring Dr./ RN / RT should have no other responsibilities
- A third person must be readily accessible if assistance is required
- If an unintentional state of general anesthesia (unrousable even with painful stimulus) is produced as a result of sedation, all parties must recognize this as an emergency situation. All physicians and staff involved in the procedure must attend solely to the patient’s well being which requires the suspension of the procedure and attention to resuscitation interventions
Training of staff #
Individuals responsible for providing Procedural Sedation should:
- Understand the pharmacology and role of all PSA medications and reversal agents
- Have the knowledge and ability to use resuscitative equipment
- Be able to recognize the associated complications
- Have airway management skills
- Have the means and the ability to recognize when to summon assistance
Nursing responsibilities #
The responsibilities of the clinician are:
- Knowledge of the objectives of PSA
- Patient assessment
- Administration of medications as per physician’s orders
- Uninterrupted observation and monitoring of the patient from time of Procedural Sedation until time of discharge from One-to-One Monitoring
- Documentation (as described below)
- Provision of appropriate emergency intervention as necessary
Physician responsibilities #
The physician responsibilities are as follows:
- Completion of history and physical
- Completion of informed consent
- Ordering of the medication, dosage and route of administration
- Directing and providing emergency interventions as necessary
- Discharge orders
- Dictation of operative note after completion of procedure (as per hospital policy)
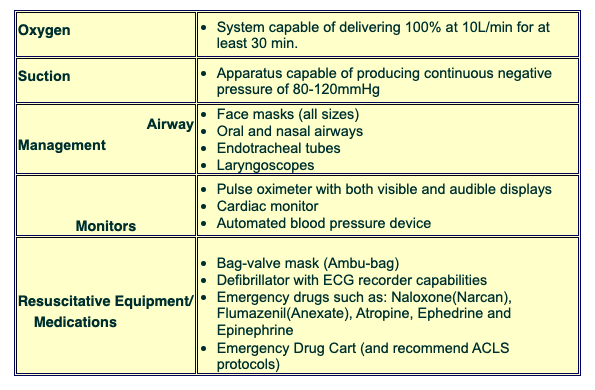
Emergency Resuscitative equipment #
Medications and Administration #
COMBINATIONS OR SEDATIVE / ANALGESIC AGENTS
While combinations of sedatives and opioids provide satisfactory Procedural Sedation, they may also increase the likelihood of adverse outcomes such as ventilatory depression, airway obstruction, and hypoxemia
While combinations of sedatives and opioids provide satisfactory Procedural Sedation, they may also increase the likelihood of adverse outcomes such as ventilatory depression, airway obstruction, and hypoxemia
- Therefore:
- Each medication and dose should be administered individually to achieve the desired effect [e.g. analgesic for pain relief, sedative to decrease awareness or anxiety]
- Doses should be titrated appropriately
- Respiratory function should be continuously monitored
TITRATION OF INTRAVENOUS SEDATIVE / ANALGESIC MEDICATIONS
Intravenous sedative / analgesic drugs should be administered in small, incremental doses which are titrated to the desired endpoints of Procedural Sedation
Titration is based on patient response as well as contributing factors such as: drug pharmacokinetics (e.g. absorption, distribution, metabolism and elimination), age, weight, medical history, hepatic and renal function, etc.
Sufficient time must lapse between doses to allow the effect of each dose to be assessed before subsequent drug administration
When drugs are administered by non-IV routes [oral, rectal, IM, SC], there should be an allowance time required for drug absorption before supplementation is considered.
Because absorption of oral medications is unpredictable, supplementation of sedation / analgesia by this route is not recommended
Refer to institutional pharmacy reference for drug dosages, onset, peak, and duration
Refer to Appendix E for Discharge Criteria
ANESTHETIC INDUCTION AGENTS
(Anesthetic Induction Agents Used for Sedation/ Analgesia )
Propofol, Ketamine
These agents can produce decreases in level of consciousness culminating in general anesthesia
**There are no specific pharmacological antagonists (reversal agents) for these agents
As such, use of these agents should be restricted to practitioners qualified to rescue patients from any level of sedation, including general anesthesia
****See institutional criteria for who can administer these agents and where this can be done [with qualified practitioners, continuous patient monitoring capability, and complete resuscitation resources available]
INTRAVENOUS ACCESS
- Intravenous administration of sedative / analgesic drugs increases the likelihood of satisfactory sedation and decreases the likelihood of adverse outcomes
- Where sedation is started by non-IV routes, IV access allows for administration of additional sedation / analgesia as well as a route for resuscitation drugs if needed
- IV access should be maintained throughout the procedure and until the patient is no longer at risk for cardio-respiratory depression and / or nausea and vomiting
- In patients without an IV, practitioners should determine the need for establishing / reestablishing IV access on a case-by-case basis
- In all instances, someone with IV skills should be immediately available
REVERSAL AGENTS
Specific antagonists include Naloxone (Narcan) for opioids and Anexate (Flumazenil) for benzodiazepines
***FLUMAZENIL MUST BE ADMINISTERED BY A PHYSICIAN
Immediate availability of these reversal agents is associated with decreased risk of adverse outcomes
However, acute reversal of opioid analgesia may result in pain, hypertension, tachycardia, or pulmonary edema
Respiratory depression should be initially treated with supplemental oxygen and, if necessary, positive-pressure ventilation by bag-valve mask
Prior to, or concomitantly with, pharmacological reversal, patients who become hypoxic or apneic during sedation / analgesia should:
1. Be encouraged or stimulated to breathe
deeply
2. Receive supplemental O2
3. Receive positive-pressure ventilation if
spontaneous ventilation inadequate
Following pharmacological reversal, patients should be monitored long enough (Minimum of 2 hours) to ensure that sedation and cardiorespiratory depression do not recur with the dissipation of antagonist effects
****Sedation regimes which include routine reversal of sedation / analgesia are discouraged
Refer to hospital pharmacy reference and / or Pharmacology Unit for drug dosages, onset, peak, and duration
Recovery Care #
CARE OF THE PATIENT POST PROCEDURE / TREATMENT
Patients may continue to be at risk for complications following their procedure
Decreased procedural stimulation, delayed drug absorption following non-IV administration, and slow drug elimination may contribute to residual sedation and cardiorespiratory depression
Following sedation / analgesia, patients should be observed in an appropriately staffed and equipped area until they return to their baseline level of consciousness and they are no longer at risk for cardiorespiratory depression
Discharge criteria should be designed to minimize risk of CNS or cardiorespiratory depression following discharge from observation by trained staff
Please refer to the VCH Guidelines for PSA Appendix F
Duration and frequency of monitoring is individualized, depending on:
- the level of sedation achieved
- patient condition
- nature of the procedure performed
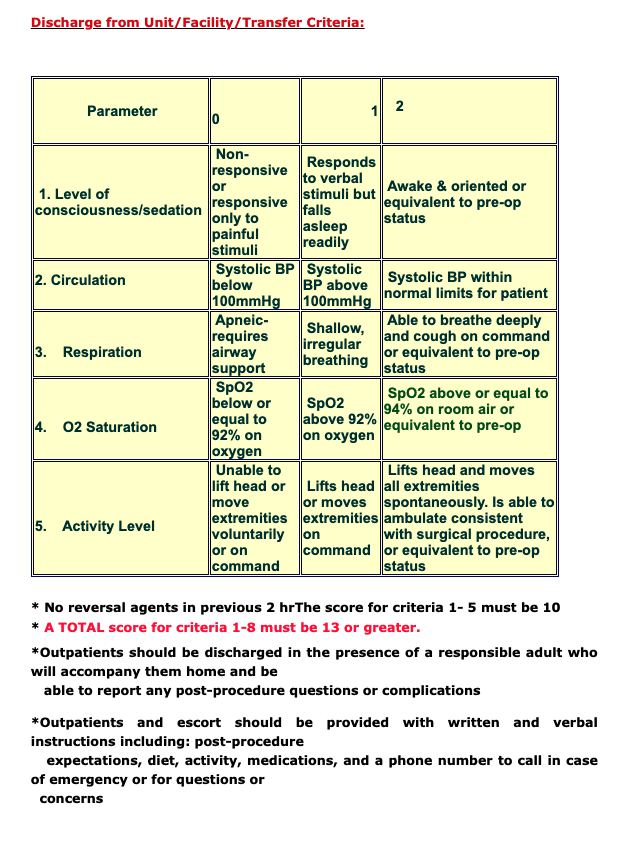
Discharge Guidelines #
DISCHARGE GUIDELINES
- Alert, oriented, has returned to pre-procedure level of consciousness
- VS stable and within acceptable limits
- Scoring system may assist in documenting fitness for discharge
- Sufficient time (Minimum of 2 hours) elapsed after receiving reversal agents to ensure that re-sedation does not occur
*****VCH Discharge Criteria uses a Modified Aldrete Scale*****
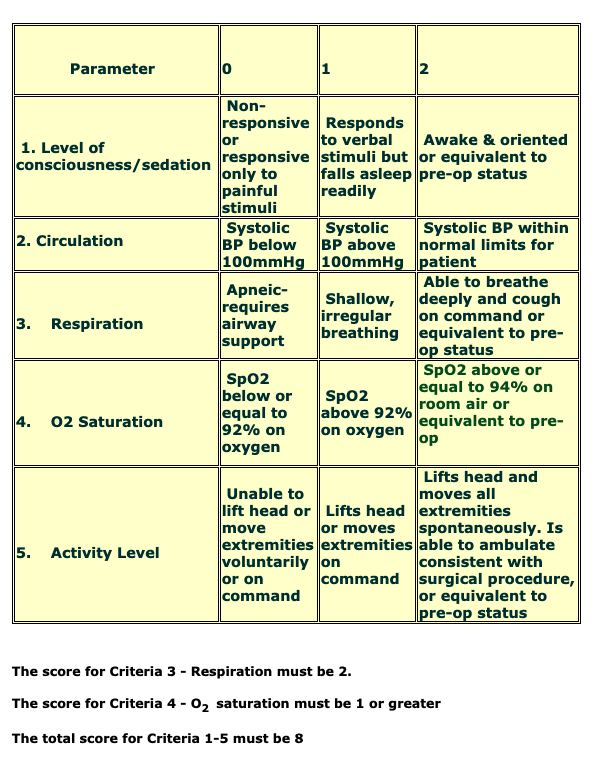
Discharge Criteria from One- to- One Monitoring:
Special situations #
SPECIAL SITUATIONS
Certain patients are at increased risk for developing complications related to sedation / analgesia and may warrant pre-procedure consultation with the appropriate specialists
- Underlying conditions which place patients at a higher risk for complications include:
- Extremes of age
- Severe cardiac / pulmonary / hepatic / renal disease
- Pregnancy
- Drug / alcohol abuse
- Obesity
- Potentially difficult airway
- Sleep apnea
- Uncooperative patient
- Anesthesiology should be consulted for compromised patients (e.g. any condition that may predispose to difficult airway management)
- A specialist may need to be consulted depending on: nature of underlying condition and urgency of situation
Monitoring equipment information #
MONITORING EQUIPMENT INFORMATION
(Capnography and Pulse Oximetry information used by permission from Nellcor Puritan Bennett LLC, Boulder, Colorado, part of Covidien)
Nellcor (Covidien)Pulse Oximetry Booklet
Nellcor (Covidien)Capnography Booklet
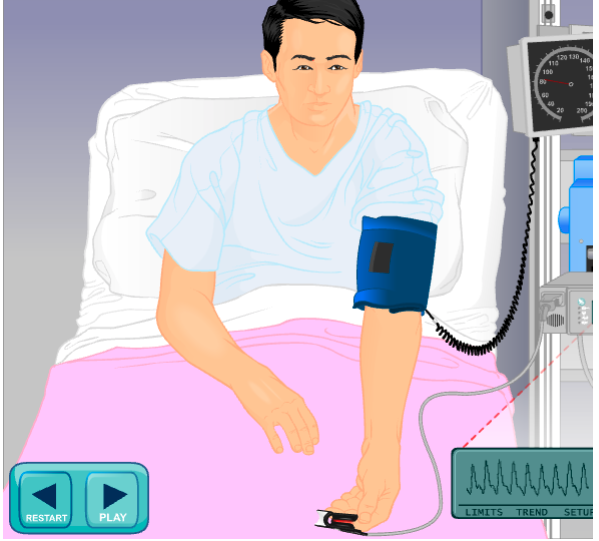
Pulse oximetry #
PULSE OXIMETRY
Pulse oximetry is an easy, painless, non-invasive method to continuously monitor SpO2. The pulse oximeter is attached to a patient with a finger or ear probe. Beams of red and infrared light pass through the tissue from a transmitter to a receiver. The receiving sensor measures the amount of light absorbed by the oxygenated and deoxygenated Hgb in pulsatile (arterial) blood. They will also monitor a patient’s heart rate by counting the pulsations, and give an indication of signal strength.
- Continuous pulse oximetry (SpO2) is mandatory for all procedural sedation/analgesia patients
- Normal Values:
- A normal SpO2 value is equal to or greater than 95%
- Values change with age, altitude, and in certain disease states (e.g. COPD)
- Normal values need to be individually determined and applied
- A major limitation of pulse oximetry is that it cannot quantify the degree of hypoxemia
Sources of SpO2 measurement errors:
- Motion artifact is the most common cause of inaccuracy with pulse oximeters. Patient movement can cause pulsatile venous flow which will be incorrectly measured as arterial pulsations, causing inaccurate heart rates and oximetry readings.
- Poor peripheral perfusion is another common cause of inaccuracy. When using the finger probe, check the proximal pulse and capillary refill closest to the site you plan to use. You may choose to use one hand rather than the other based on your assessment. Look for tight clothes, wrist restraints, tightly taped IV’s, BP cuffs, arterial lines as potential causes of restricted circulation. If the extremities are cold, you may try to warm the person’s hands or increase perfusion by applying heated towels or blankets.
- Exposure of the measuring probe to ambient light
- Abnormal hemoglobin can cause false highs (e.g. carboxyhemoglobin with smokers)
- Edematous sites will cause inaccurate values, as light from the LED will scatter throughout edematous tissue before reaching the photodetector (e.g.. vascular disease)
- Some intravascular dyes (e.g. cardiac output studies) cause false highs
- Methylene blue can cause a 65% false reduction
- Hemodilution, severe anemia
- Skin pigmentation- in cases with increased melanin or bilirubin
- Nail polish or acrylic nails- fingernail polish with black or blue hues can cause a false low of 3-5%
- Venous pulsations will cause false lows (Right sided heart failure, tricuspid regurgitation, tightly applied tensor, tourniquet application, BP cuff in/deflation
Tips for accurate measurement:
- Use trended rather than isolated values
- Apply a well-fitting sensor probe
- Check perfusion at the probe site-ensure the pulse display is over 3 bars
- Avoid edematous sites
- Avoid tension on the cable
- Avoid application of the sensor on the same limb as a noninvasive BP monitor
- Warm up the extremity (e.g. warm blanket)
- Try an ear probe (if peripherally shut down)
NON-INVASIVE BP MONITORING
- BP is a central measure of arterial flow, volume and tone
- Measurements are performed Q 5-15 mins, for the course of the patient’s procedural and recovery period
- Normal values for systolic pressure fall within 90-140mmHg
- Normal values for diastolic pressure fall within 60-90mmHg
- Sources of measurement error:
- Bladder length should be 80% of arm circumference and cuff width should be equal to 40% of arm circumference
- If the cuff is too small; pressure measurements will be falsely elevated
- If the cuff is too large, pressure measurements will be falsely low
- Rapid deflation of the cuff will produce a false high in systolic pressure, and a false high or low in diastolic pressure
- Placement of the limb above the heart causes a false low blood pressure
- Displacement of the pulse sensor away from the artery
- Applying the cuff upside down
- Principles and practices:
- Measure BP in both arms (a difference in systolic pressure of more than 10-15 mmHg indicates a decreased arterial flow on the lower reading side (e.g. obstruction, dissection)
- Check BP in supine, sitting and standing positions. A drop in systolic pressure of more than 20mmHg signifies orthostatic hypotension (e.g. vasodilating drugs, volume depletion)
TEMPERATURE
There are situations in which temperatures should be taken/monitored:
- Long procedure (>2hrs)
- History of hypo/hyperthermia (pt/family)
- Children or elderly
- Multiple crystalloid or colloid infusions
- Procedure specific
- Based on patient assessment
ETCO2 (Capnography) #
ETCO2
- End-tidal CO2 is the maximal concentration of CO2 at the end of an exhaled breath, and is a reflection of both ventilation and cardiovascular function
Normal values: 35-45mmHg
- Measured (sidestream or mainstream) by:
- Capnometry: numerical measurement of CO2 level in airway
- Capnography: graphical measurement of CO2 level in airway
- TYPES OF CAPNOGRAPHY
Mainstream Capnographs:
- Respiratory gases are continuously measured through an adaptor at the patients airway
- There is no lag-time, but this method is unable to monitor non-intubated patients
Sidestream Capnographs:
- Respiratory gases are continuously measured through an adaptor at the patients airway and transported through a sampling tube to the sensor
- Lag-time of 1-2 seconds, no added weight on the airway
- Is effective in the early detection of adverse respiratory events such as hypoventilation, airway obstruction and apnea which precede the actual development of hypoxia
- Capnography provides a breath by breath measurement of a patient’s ventilation that can quickly reveal a worsening trend in a patient’s condition
RECOMMENDED USES
Recommended for use where:
- 1. Deep sedation is a probable or planned outcome
- 2. Moderate or dissociative sedation is a probable or planned outcome
- 3. In any patient with ASA classification status of 3 or above
- 4.The respiratory rate assessment may be difficult due to procedural draping or positioning
CO2 PHYSIOLOGY
Normal CO2 Physiology:
- Combustion of food by cellular metabolism to produce energy is the source of physiologic CO2.
- CO2 is transported in the venous blood in 3 principal forms:
- 1) 5-10% is carried in physical solution and reflected by the PCO2
- 2) 20-30% is bound to blood proteins
- 3) 60-70% is carried as bicarbonate ion
WAVEFORMS
- Normal Capnography waveform:CO2 waveforms must include all of the following components for the ETCO2 to be a good estimator of PaCO2:A= zero baseline
- B= a rapid, sharp uprise
- C= an alveolar plateauSlide 4
- D= a well-defined end-tidal point
- E= a rapid, sharp downstroke
Abnormal Capnography waveforms:
1. Slow decrease in ETCO2.
The possible causes are:
- Hypovolemia
- Decreasing cardiac output
- Hypothermia
2.Exponential decrease in ETCO2 .
The possible causes are:
- Circulatory arrest
- Embolism
- Sudden hypotension, massive blood loss
- Sudden severe hyperventilation
3. Sudden loss of ETCO2 to or near 0
The possible causes are:
- Esophageal intubation
- Totally obstructed or kinked ET tube
- Kinked sampling tube
- Complete airway disconnection from ventilator
- Ventilator failure
4. Sustained low ETCO2
The possible causes are:
- Emphysema, asthma or chronic bronchitis
- Pulmonary emboli
- Pneumonia
- Hyperventilation
- Hyperthermia
5. Gradual increase in ETCO2The possible causes are:
- Hypoventilation
- Absorption of CO2 from peritoneal cavity
- Rapidly rising body temperature
6.Sudden increase in ETCO2
- The possible causes are:Injection of sodium bicarbonate
- Release of tourniquet
- Sudden increase in blood pressure
ECG Monitoring #
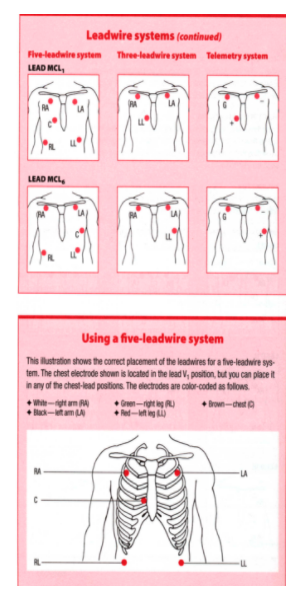
ECG MONITORING
All patients, regardless of location, should be placed on ECG monitoring during the procedure and continued until they meet the One to One Discharge Criteria
***All clinically significant ECG strips should be analyzed and mounted in the patient’s chart
For accurate monitoring, the electrode placement for a 3 or 5 lead system is pictured on the next slide. This placement may not be possible with certain procedure sites and dressings
REFERENCES
- American Society of Anesthesiologists. (2001). (Practice guidelines for sedation and analgesia by non-anesthesiologists. An updated report by the American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non-Anesthesiologists., 2001) and analgesia, 1-74
- AORN (2000). Recommended Practices for Managing the Patient Receiving Conscious Sedation/Analgesia.Available http://www.asahq.org/publicationsAndServices/practiceparam.htm#sedation
- Canadian Society of gastroenterology Nurses and Associates (2001). Guidelines for the Care of patients receiving conscious sedation.
- Cleveland Clinic Foundation. Guidelines for Procedural Sedation / Analgesia, http:www.asahq.orgclinicaltoolkitglproceduralsedation.pdf
- Cochran Foundation of Medical Research. Cardiovascular Disease Classification Chart. http://www.cochranfoundation.org/main/Cardio%20NYHA%20Classifications.htm
- Kobs, Ann. (1997). “Conscious sedation”. Questions about the anesthesia continuum. [In questions and answers from the JCAHO]. Nursing Management, 28(4), p. 14 & 17.
- Kost, M., (2004). Moderate Sedation: Core Competencies for Practice, 2nd edition, W.B. Saunders CO Saunders Elsevier, St. Louis, MO
- Policies from the following hospitals were also reviewed: Surrey Memorial, St. Paul’s Hospital, Richmond Hospital, Peace Arch Hospital, Vancouver Hospital, BC Children’s Hospital
- Robins, E., Bozadjian, E., (1997). Developing a Competency Based Program for Conscious Sedation.