Description #
This unit is designed to help health care professionals develop a better understanding of the risk factors and pathophysiology of Chronic Obstructive Pulmonary Disease (COPD).
Learning Objectives #
By the end of this unit, you should be able to:
1. Identify the risk factors for development of COPD
2. Explain the pathophysiology of COPD
3. List common comorbid conditions associated with COPD
Risk Factors #

Cigarette smoke is the most common cause of COPD. It can also be caused by long-term exposure to other airway irritants such as air pollution and occupational agents. In a small number of cases, COPD is caused by a hereditary disorder called alpha 1 – antitrypsin (AAT) deficiency.
Below is a break-down of the most common known risk factors for developing COPD.

Environmental Risk Factors #
In the majority of cases, COPD is caused by an abnormal inflammatory response of the lung to exposure to noxious particles or gases.
The most common environmental risk factors for COPD are described below. These are also known as “modifiable” risk factors, since the risk of developing COPD can be reduced by modifying exposure to these agents.
Smoking:
Smoking tobacco is the principal cause of 80 to 90% of COPD cases. The absolute risk for a continuing smoker to develop COPD is about 20% .
Tobacco smoke contains thousands of toxic chemicals, including arsenic, methane, hydrogen cyanide, and carbon monoxide. Exposure of the lungs to these harmful substances, particularly repeated and heavy exposure, causes the irreversible damage to the lungs seen in chronic bronchitis and emphysema. In most COPD patients, this exposure spans several decades. The greater the exposure, the higher the risk for developing COPD.
When assessing a smoker’s risk for developing COPD, quantification of tobacco consumption should be made. This is done through a calculation of Total Pack Years.
Total Pack Years = (number of cigarettes smoked per day ÷ 20) X number of years smoking
For example, a person who smokes 40 cigarettes a day and has smoked for 10 years would have a 20 pack-year smoking history
(40 cigarettes per day ÷ 20 cigarettes per pack) X = 10 years of smoking = 20 pack-year history.
Smokers who develop COPD typically have at least a 20 pack-year smoking history. Smoking cessation in patients with COPD will result only in minimal improvements in lung function. The damage that has been caused is not reversible. However, the subsequent loss of lung function as a result of the normal aging process will slow down to the rate seen in non-smokers.
It is recommended that health care providers offer a combination of pharmacotherapy and counseling to all patients who smoke in order to help them quit. Indivduals who have already developed COPD can reduce the rate of loss of lung function by quitting.
Environmental Tobacco Smoke (ETS):
Exposure to ETS in childhood can adversely affect lung growth and it may be associated with an increased risk of severe respiratory infections and developing COPD later in life. As well smoking during pregnancy is associated with low birth weight and abnormal growth and development of the lungs in utero. Exposure to tobacco smoke in the house, car and workplace has been associated with deterioration in lung function and safe levels of exposure have not been determined. Environmental smoking by-laws, which prohibit smoking in places such as cars and various public spaces, are therefore important in disease prevention, particularly in children.
Occupational Agents:
Another major risk factor is occupational exposure to certain dusts (e.g., cadmium, gold, coal, grain) and solvent fumes. Mixed exposures (dust and fume combination) appear to also play a role in development of COPD. Other relevant occupational agents include fibreglass, asbestos, and wood smoke.
Air Pollution:
Outdoor air pollution caused by automobile emissions (“smog”) is associated with increased symptoms among those with COPD, and it may play a minor role in the development of COPD in non-smokers. In cities heavily polluted by the burning of coal, the risks may be higher. In developing countries, where indoor air is polluted owing to poor ventilation of cooking smoke, the risk is also increased.
Host Factors #
About 10-20% of all COPD cases are cause by host factors, or factors associated with indivduals who acquire the disease. Host susceptibility may explain why only some smokers develop COPD.
Host factors are also known as non-modifiable risk factors, because they cannot be changed. Awareness of these risk factors is important in preventing disease in patients who smoke or have other modifiable risk factors. Consideration of these risk factors also plays a role in making an early diagnosis in patients who present with respiratory symptoms of COPD.
Age:
Age is the most important risk factor for COPD after smoking. COPD develops slowly over many years. Most people are at least 40 years old when symptoms appear. This is, in part, owing to the number of years spent smoking.
Although our lung function naturally decreases as we age, a much faster decline in lung function occurs in patients with COPD.
Susceptibility genes:
Although the vast majority of COPD cases are caused by COPD, only about 25% of smokers develop COPD. This variability in susceptibility to lung function decline among smokers is thought to have a genetic component.
Evidence of this genetic influence is demonstrated by studies showing that family members of patients with COPD are 1.2 to 3 times more likely to develop the disease. Genes may influence mechanisms such as the metabolism of toxic substances and the efficacy of mucociliary clearance.
Alpha1-antitrypsin (AAT) deficiency:
Alpha1-antitrypsin (AAT) deficiency is an autosomal, hereditary disorder which accounts for about 1-2% of all cases of emphysema. It is the most well-studied genetic cause of COPD.
Individuals with AAT deficiency have a 50-80% chance of developing emphysema. In non-smokers, respiratory sysmptoms usually do not appear until after age 50. In smokers, the disease can appear much sooner, often in their 30’s or 40’s.
AAT deficiency tends to be an underrecognized cause of COPD. It is estimated that fewer than 20% cases are diagnosed and treated.
The pathophysiology, diagnosis, and treatment of AAT deficiency is covered later in this course.
Childhood viral infections:
Severe respiratory infections in childhood may affect pulmonary defense mechanisms and alter lung development. Infections can cause scarring and reduced lung elasticity which can lead to reduced lung function and may predispose individuals to develop COPD later in life. When developing lungs are exposed to more than one damaging factor, such as second-hand smoke as well as pulmonary viral infections, the effects on respiratory function are compounded.
Asthma and bronchial hyper-responsiveness:
Bronchial hyper-responsive (BHR) is a condition in which the airways constrict too easily or too much in response to an airborne irritant, allergen, or other provoking stimulus. It is now thought to be an important risk factor for COPD, rather than a consequence of the disease.
As well as having symptoms which overlap with COPD, a history of physician-diagnosed asthma is itself a risk factor for developing COPD.
Individuals who smoke, as well as having nonspecific BHR, are at a greater risk for accelerated lung function decline. Female smokers seem to have more BHR than male smokers.
Other Potential Risk Factors #
There are a number of other factors, both modifiable and non-modifiable, that increase the risk of COPD. These risk factors are less well understood, and while they are not considered to be the most important risk factors for developing COPD, when combined with other risk factors, such as genetics and smoking, they can considerably increase the likelihood of developing the disease.
Female gender:
There is evidence of a female predisposition to the harmful effects of smoking and to some environmental and occupational risk factors. Female gender is the 3rd most important predictor of COPD after smoking and age. When this independent risk factor is combined with the rising prevalence of smoking in women, it is projected that COPD–related hospitalizations and deaths will be higher in women than in men in the future.
Low socioeconomic status:
There is a strong correlation between socioeconomic status, measured by education and income level, and the risk of developing COPD. A higher incidence of COPD is seen in lower socioeconomic groups. This is partly explained by the higher smoking rates among people in these groups, as well as a higher exposure to environmental and occupational risk factors. However exposure to these other risk factors may not explain all of the association and socioeconomic status is thought to be an important independent risk factor for COPD.
Poor nutrition:
Low body mass index is a risk factor for mortality in COPD. Weight loss and malnutrition are serious problems for patients with end-stage COPD, especially emphysema. Poor nutrition, caused by mechanical inefficiency of breathing and reduced dietary intake, can impair respiratory muscle strength, endurance, and immune system responses. This can, in turn, lead to hyperpneic respiratory failure and an increased susceptibility to lung infections. Patients with acute exacerbation of COPD are often malnourished on hospital admission and are subject to further decline during hospitalization.
Poor lung growth and development:
Newborns with poor airway function are more likely to have breathing disorders as adults. It is abnormal lung growth and development in the womb that appears to increase the risk for COPD later in life. Examples of potential causes of impaired fetal lung development include maternal smoking during pregnancy, genetic disorders, prematurity, and low birthweight.
Pathophysiology #
As mentioned in the previous unit, chronic bronchitis and emphysema are the two main pathologies that contribute to COPD. Patients with COPD have elements of one or both diseases. The signs and symptoms of chronic bronchitis and emphysema are covered in unit COPD-101.
The pathogenesis of COPD can be summarized as the result of an individual’s genetic susceptibility combined with exposure to one or more risk factors, leading to abnormal inflammatory processes. Regardless of the main pathology, either chronic bronchitis or emphysema, these processes ultimately result in severe airflow limitation and respiratory failure.
The primary pathophysiological features of COPD are summarized below. It is a combination of these mechanisms that cause the symptoms seen in all patients with COPD.
1. Inflammation
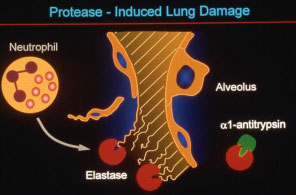
The normal inflammatory response is amplified in individuals who develop COPD. A wide range of inflammatory cells and mediators are involved. The most common cell types involved in the pathogenesis of COPD are neutrophils, macrophages, and CD8+ T lymphocytes.
In COPD, the protease elastase is released excessively in the lung in response to an irritant. Elastase is a proteolytic enzyme released by the white blood cells which digests bacteria and other foreign irritants in the lungs. The high elastase levels cannot be counterbalanced effectively by antiproteases, leading to elastin-mediated breakdown of the alveolar walls and destruction of lung tissue and the pulmonary vasculature. This damage to the tissues of the lung causes the airways to collapse and obstruct. Persistent and repeated inflammation of the small and large airways also leads to enlargement of the mucus glands and a hypersecretion of mucus, further contributing to narrowing of the airways and obstruction. The inflammatory process seen in patients with COPD persists long after the irritant (eg. cigarette smoke) is withdrawn.
Asthma is sometimes present with COPD, but not always. Like COPD, asthma is also a chronic inflammatory lung disorder, however the cells that contribute to the inflammatory process are different. The management of inflammation in these two separate diseases is also different. It is therefore important to determine whether or not asthma is present in a patient with COPD. Misdiagnosis is also common owing to similarities in clinical presentation between COPD and asthma. Some of these differences are summarized later in this unit.
2. Impaired defense mechanisms
The inflammation seen in COPD also impairs the defense mechanisms of the lungs. When the systems which normally repair damaged lung tissue is disrupted, airway tissue remodeling and scar tissue formation can occur, contributing to a decline in lung function.
As well, the mechanisms for eliminating mucus and foreign substances from the airways are also impaired. The lining of the airways is covered with tiny hair-like structures called cilia. Cilia beat continuously in a wave-like fashion to sweep and clean foreign material out of the lungs. Toxins and noxious gases that are inhaled into the lungs can damage or paralyze the cilia, slowing down their movement. This means that bacteria, viruses, environmental pollutants, tar, and toxins remain in the lungs. Mucus, which is hypersecreted in response to irritants and toxins, also accumulates in the airways, trapping inhaled particles.
This impaired mucociliary response seen in patients with COPD leaves patients at significantly higher risk for respiratory infections, exacerbations, and further damage to the airways.
It should be noted that quitting smoking will reverse this effect. The cilia begin to recover within days of quitting, and mucus and foreign materials will start to be swept out of the lungs more efficiently. The temporary increase in productive cough seen in smokers who have recently quit can be attributed to the reversal of ciliary paralysis. Unfortunately, in smokers who have already developed COPD, some of the damage caused to the lung will not be reversed by quitting. However smoking cessation remains a vitally important component of COPD management, since it will slow the progression of the disease.
3. Expiratory flow limitation
Expiratory flow limitation is the pathophysiological hallmark of COPD. It arises from a combination of a variety of factors affecting the airways. The mechanisms affecting airflow will vary from patient to patient, and in most patients the disease will be the result of multiple mechanisms.
In patients who have emphysema as the predominant component of COPD, alveolar wall damage is the main cause of expiratory flow limitation. The elastic recoil of the lung is reduced causing a reduction in the driving pressure for expiratory flow. As well, small airways can become compressed by adjacent overinflated lung units. The resulting abnormal expansion and contraction of the lungs causes breathing to become more laboured.
In patients with chronic bronchitis as the primary pathology, expiratory flow limitation results from increased resistance of the airways from mucosal thickening. Mucosal inflammation and edema lead to an increase in size and number of the goblet cells, which secrete mucus into the airways. Excessive mucus secretion may occlude the airways by mucus plugging. The airways are further narrowed as a result of repeated attempts at tissue repair. This leads to bronchial wall thickening, airway remodeling and fibrosis. The airways can become hyperresponsive or “twitchy”, as in asthma, however the resulting bronchoconstriction is only partially reversible with bronchodilator therapy.
4. Lung hyperinflation
As a result of the various mechanisms of expiratory flow limitation in COPD, a higher than normal volume of air remains in the lungs at the end of expiration. During times of increased ventilatory demand, or in advanced disease, air can become trapped in the lungs causing them to become overinflated with air. With lung hyperinflation, breathing becomes less efficient, contributing to an increased work of breathing, feelings of shortness of breath and anxiety.
In emphysema, hyperinflation of damaged areas of the lung can cause the development of bullae. Bullae are severely dilated air sacs which can aggravate gas exchange abnormalities and compress healthier areas of the lung. They can eventually rupture, causing sudden and severe respiratory symptoms and possibly a pneumothorax.
Patients with chronically hyperinflated lungs may develop a barrel-shaped chest. On chest x-ray, lung hyperinflation is often revealed as lung field hyperlucency and flattened diaphragms.
4. Respiratory failure
In healthy lungs, the tissue is perfused with blood via the pulmonary and bronchial arteries, and ultimately by the pulmonary capillaries in the alveolar walls. Blood leaves the lungs via the pulmonary veins.
In COPD, airway obstruction, together with destruction of the alveoli and the pulmonary vasculature lead to severely abnormal gas exchange. Both ventilation and perfusion of the lung tissues are impaired, with the result that oxygen uptake by the bloodstream and carbon dioxide elimination by the lungs are compromised. COPD patients may initially be able to compensate for these gas exchange abnormalities, by changing their ventilatory pattern. But during exacerbations, or in advanced disease, hypoxemia, hypercapnia and respiratory acidosis may develop.
Some patients with COPD can also be hypoxemic as a result of an increased work of breathing. These patients simply hypoventilate, become hypercapnic which will lower arterial oxygen content.
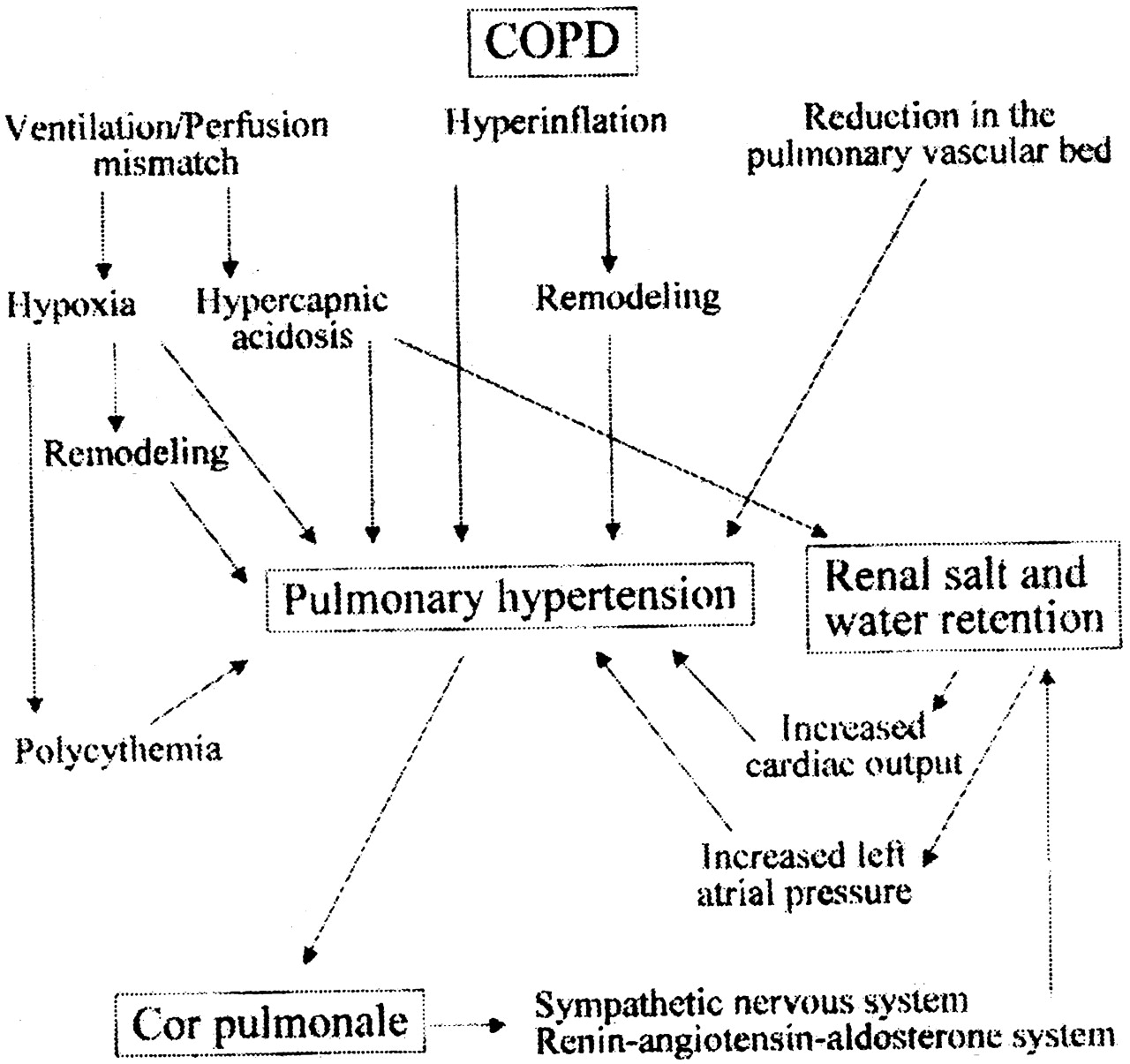
5. Pulmonary hypertension
Some patients with advanced COPD will develop pulmonary hypertension. This is owing to a combination of the vasoconstrictor effect of hypoxemia in the lungs, and the destruction of the pulmonary capillary bed.
Pulmonary hypertension is also caused by the direct toxic effects of tobacco smoke on the pulmonary vasculature.
This permanently increased pulmonary vascular resistance causes strain on the heart, and is associated with the development of cor pulmonale, or hypertrophy and dilation of the right ventricle.
Symptoms of cor pulmonale are peripheral edema, seen as swelling of the ankles, and shortness of breath.
The presence of pulmonary hypertension in COPD indicates a poor prognosis.
Alpha-1 Antitrypsin Deficiency #
As mentioned under the “Risk Factors” section of this unit, alpha1-antitrypsin (A1AT) deficiency is a hereditary disorder accounting for 1-2% of all cases of emphysema. Individuals with this disease have a 50-80% chance of developing emphysema.
The pathogenesis of emphysema caused by A1AT deficiency is slightly different than the “usual” COPD caused by smoking and exposure to other noxious particles and gases.
A1AT deficiency is a systemic disease, primarily affecting the lungs, in which there are low serum and lung levels of A1AT. A1AT is a natural protein, produced by the liver, that protects the lung tissue by controlling elastase levels.
When a person with A1AT deficiency is exposed to respiratory irritants or infection, elastase is released in the lung unchecked, eventually destroying healthy lung tissue as well. This lung structure degradation leads to emphysema.
The damage to the lung is faster and more pronounced in patients who smoke . A1AT deficiency may cause liver disease (cirrhosis) as well as COPD.
Depending on the type of A1AT deficiency, some individuals will not develop liver or lung disease. However, when emphysema and cirrhosis do appear, the disease can be life threatening. Symptoms are the same as those seen in severe or end-stage COPD.
Adults with emphysema caused by A1AT deficiency will develop symptoms at a much earlier age than patients with emphysema of other causes. This is especially true in smokers with A1AT deficiency, with symptoms often occurring in their 30’s and 40’s.
Alpha-1 antitrypsin level testing should take place in patients who are diagnosed with COPD:
- Before age 65
- Who have a smoking history of <20 pack years.
The treatment of A1AT deficiency is discussed in unit COPD-104:Management of Stable COPD
For more information on A1AT deficiency, click here for a downloadable PDF: A1ATDeficiency.pdf
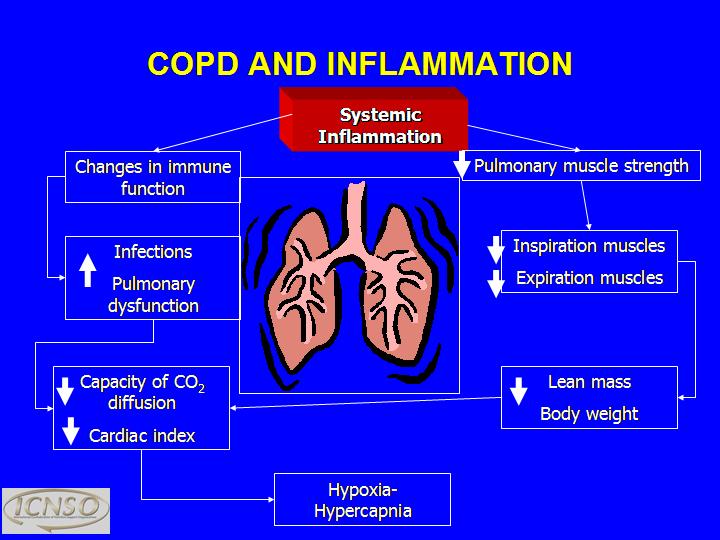
Systemic Effects #
COPD is a systemic disease, affecting more than just the lungs. We know this because inflammatory markers and pro-inflammatory mediators can be found in the bloodstream of COPD patients. The levels of these markers rise with increasing disease severity and are associated with poor lung function and the development of comorbid diseases.
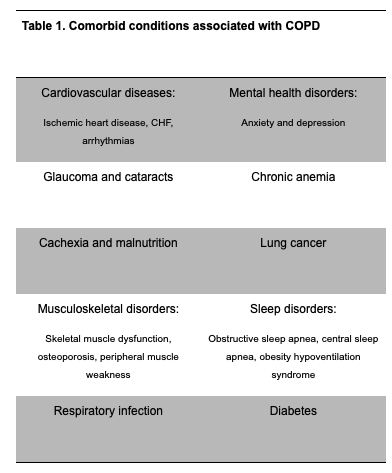
Comorbidities #
A comorbidity is a disease or other pathological process that occurs simultaneously with the primary disease of interest. Quite often, patients with COPD have multiple comorbid diseases. Table 1 below displays a list of common comorbidities associated with COPD.
The gas exchange abnormalities and hypoxemia resulting from airflow obstruction have a profound effect on all organ systems of the body. Some comorbidities, such as lung cancer and heart disease, share cigarette smoking as a common risk factor with COPD.
Also, as previously noted, abnormal inflammatory processes may not only be responsible for lung disease in COPD, but they may also play a role in the development of some of the comorbidities associated with COPD. Systemic inflammation may cause or worsen comorbid conditions such as cardiovascular disease, anemia, diabetes, and osteoporosis.
The presence of comorbidities often complicates the management of COPD. Comorbidities should be actively identified and treated as they contribute significantly to the risk of hospitalization and mortality.
References #
Ministry of Health guidelines
- O’Donnell DE, Aaron S, Bourbeau J, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease – 2007 update. Can Respir J. 2007;14(Suppl B):5B-32B.
- O’Donnell DE, Hernandez P, Caplan A, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease – 2008 update – highlights for primary care. Can Respir J. 2008;15(Suppl A):1A-8A.
- Marciniuk D, Hernandez P, Balter M, et al; Canadian Thoracic Society COPD Clinical Assembly Alpha-1 Antitrypsin Deficiency Expert Working Group. Alpha-1 antitrypsin deficiency target testing and augmentation therapy: A Canadian Thoracic Society clinical practice guideline. Can Respir J 2012;19(2):109-116.