Description #
A description will be added here.
Learning Objectives #
At the conclusion of this unit the student should be able to:
1) Identify the clinical symptoms manifested by a pulmonary embolus:
- acute, sudden onset of shortness of breath
- pain on inspiration
- high respiratory rate
- decreased oxygen saturations (not responsive to increase in oxygen)
- elevated JVD-etc (have to add more!)
2) Be able to appropriately respond to the clinical signs and symptoms as it relates to a pulmonary embolus
- increase oxygen to meet demands (use appropriate supportive oxygen therapy)
- arterial blood gasses
- full respiratory assessment
- ECG (differential diagnosis)
- continuous oxygen saturation readings
3) Identify common risk factors associated with pulmonary emoblus (identify the specifics of the risk factors associated with a surgical patient)
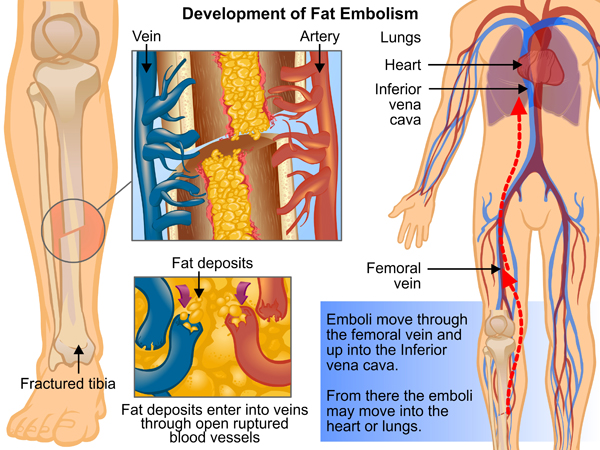
- a) recent long bone fractures
- oral contraceptives
- smoking
- prolonged best rest
- coagulation disorders
Etiology and Pathophysiology of Acute Pulmonary Embolism #
Etiology:
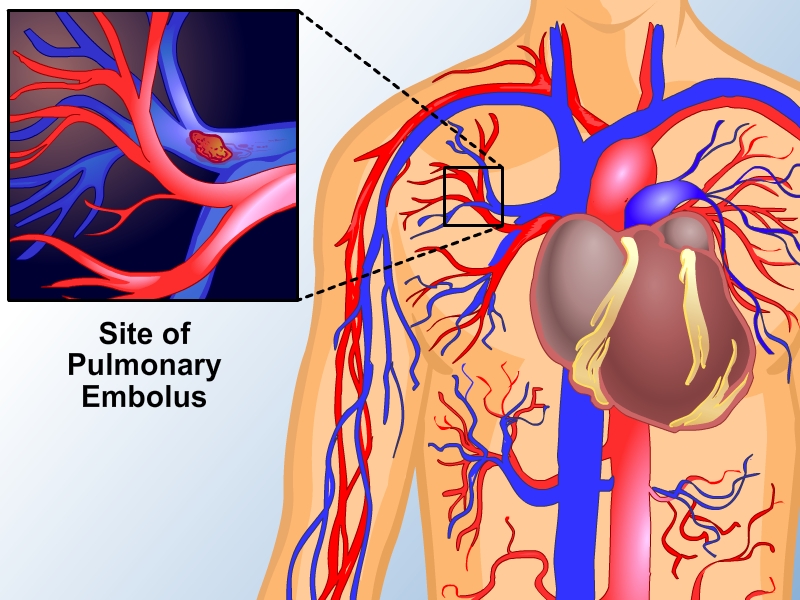
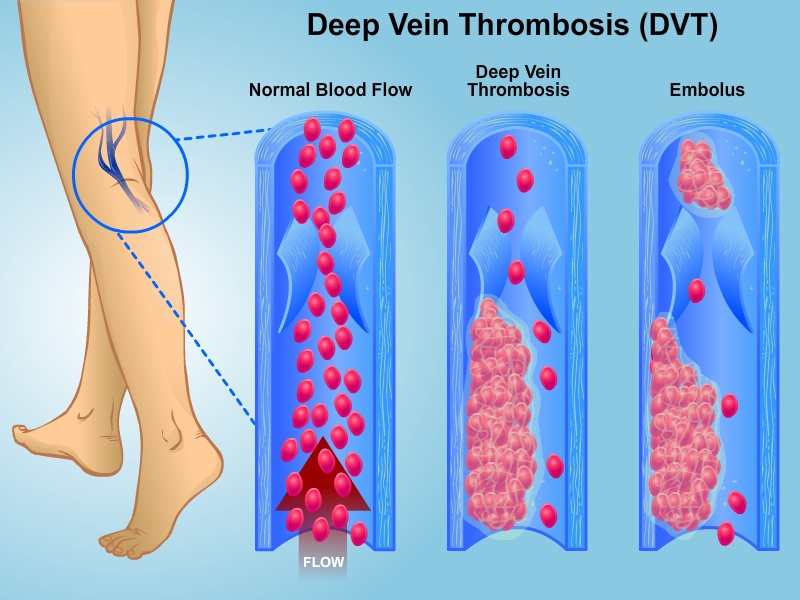
Pulmonary embolism (PE) is a relatively common disorder, and refers to the vascular obstruction (embolization) of the pulmonary arteries by blood clots (emboli). The emboli are usually originated from deep vein thrombi (DVT) of the calves, the thighs and pelvis. The thrombi break off from these sites and travel through the venous system to the lungs, with subsequent obstruction of blood flow to lung tissue. There are other possible causes of PE, such as fat globules from bone fractures, amniotic fluid from vaginal or C-section delivery, air from improper priming of IV line, and tumor fragments from tumor.
Predisposing risk factors for DVT involve one or more components of Virchow’s Triad: 1) hyper-coagulability of the blood, 2) blood vessel wall damage, and 3) venostasis. Hypercoagulability is a factor caused by genetic deficiencies in antithrombin III, protein S, protein C, and lupus anticoagulant. Fractures and surgical procedures, along with trauma are common causes of venous blood vessel damage. Venostasis is common in any circumstance that promotes physical immobilization, such as surgery, fractures, obesity, and prolonged illness. Although thromboemboli may form at almost any site, approximately 95% originate in the deep veins of the lower extremities. The remainders usually form in the pelvic veins. Thrombi may also form in the upper extremities, or as a result of indwelling catheters. Thrombi generally form at the site of turbulent blood flow around the venous valves or directly on the sites of endothelial wall damage.
Risk factors for DVT include obesity, congestive heart failure, malignancy, burns, use of estrogen-containing medications, and postoperative and postpartum states. These factors are additive in effect. Risk of embolism appears highest within the first 72 hours of development of a DVT. Age is not an independent risk factor but the higher likelihood of having more than one predisposing factors increases the frequency of PE in people over age 70. Genetics may play a role and genetic testing may be more common in coming years.
Pathophysiology:
Acute pulmonary embolism is a dynamic process, and affects both the respiratory and cardiac systems. The effects of PE range from being incidental and clinically irrelevant to severe obstruction of the pulmonary vasculature and sudden death. The pathologic changes in the lung are related both to the magnitude of the occlusion, and the subsequent degree of compromised pulmonary blood supply. The resulting physiologic changes may include dyspnea (shortness of breath) with tachypnea (high respiratory rate) and hyperventilation, arterial hypoxemia, pulmonary infarction, pulmonary hypertension with right ventricular failure and shock.
Tachypnea and dyspnea, almost always occurs after a PE. This process appears to be due to stimulation of juxtacapillary receptors (J receptors) in the alveolar capillary membrane by swelling of the alveolar interstitial space. The rapid and shallow breathing is usually associated with alveolar hyperventilation, which results in a lowered PaCO2 (hypocapnia) and respiratory alkalemia.
After occlusion of the pulmonary arteries, areas of the lung are ventilated but not perfused, resulting in wasted ventilation (alveolar deadspace) – the physiologic hallmark of PE. Local bronchoconstriction also typically accompanies pulmonary embolism. The release of cellular mediators such as serotonin, histamine, and prostaglandins from platelets, as well as local areas of hypocapnia, and hypoxemia are all thought to be involved in causing the bronchoconstriction, although the exact etiology is unknown. Obstruction of blood flow to the lung tissue results in decreased surfactant production about 24 hours after the embolization. This leads to decreased pulmonary compliance, atelectasis, and more hypoxemia. If severe, the decreased compliance and atelectasis can lead to acute respiratory distress syndrome (ARDS).
Vascular occlusion and vasoconstriction cause an increase in pulmonary vascular resistance (PVR) and pulmonary hypertension. The increase in PVR increases the work of the right ventricle; the right ventricle must generate a pressure higher than the pulmonary arteries in order for blood flow. When pulmonary hypertension increases beyond the limits of the right ventricular function, right ventricular failure (cor pulmonale) occurs, with a fall in forward cardiac output. Leading to inadequate filling in the left side of the heart, resulting in systemic hypotension and eventually shock (peripheral vasoconstriction; diaphoresis; a weak, thready pulse; oliguria; and changes in level of consciousness). Shock from PE has a unique feature of having an elevated central venous pressure (jugular vein distension) from right ventricular failure and low pressures in the left side of heart. Approximately 50% or more occlusion of the pulmonary vasculature must occur in previously healthy individuals before sustained pulmonary hypertension develops and cardiac output falls. The severity of the hemodynamic compromise depends not only on the magnitude of the embolism but also on the patients preexisting cardiovascular and pulmonary status. Pulmonary or cardiovascular disease that limit reserve such as congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), and aortic or mitral valve disease, frequently result in greater than expected pulmonary hypertension compared to an otherwise healthy patient. Although pulmonary infarction (PI) is a potential consequence of embolism, death of lung tissue is uncommon. Usually there is some collateral blood flow via bronchial arteries, and oxygenation by the airways. Pulmonary infarction is more common in patients with left ventricular failure or COPD, probably because of the reduced cardiac output or reduced collateral blood flow, respectively, and only in the case of massive PE. Natural resolution of the thromboembolus begins shortly after the clot lodges in the pulmonary arteries. Fibrnolysis is the process of clot destruction in which blood-borne and vascular endothelial factors, such as tissue plasminogen activator (tPA), act to dissolve the clot. Resolution usually results in complete or partial return of flow within 7 to 10 days. Perfusion can be restored with as little as 20% of the vessel diameter being patent.
Clinical Features:
The clinical manifestations of PE are nonspecific and vary in frequency and intensity, depending on the extent of pulmonary vascular occlusion, pre-embolic cardiopulmonary function, and the development of pulmonary infarction (PI). Dyspnea, pleuritic chest pain, and hemoptysis (coughing up blood) are the classic symptoms. Most patients will have at least one of these symptoms, with dyspnea being the most common. Pleuritic chest pain and hemoptysis indicate pulmonary infarction and pleural involvement. Syncope, although uncommon, suggests massive PE, and severe hemodynamic compromise. A sense of impending doom and anxiety is a potential symptom and may be associated with large emboli and hypotension. Physical signs include tachypnea, tachycardia, and low-grade fever. The lower extremities are often normal but may reveal swelling and tenderness associated with a large DVT. The patient’s breath sounds may be normal or may reveal localized wheezing or crackles. A pleural friction rub may also be heard, particularly if infarction of the pleura is involved. Arterial blood gases (ABG’s) commonly show an uncompensated respiratory alkalosis (low PaCO2 and high pH) with mild to moderate hypoxemia on room air.
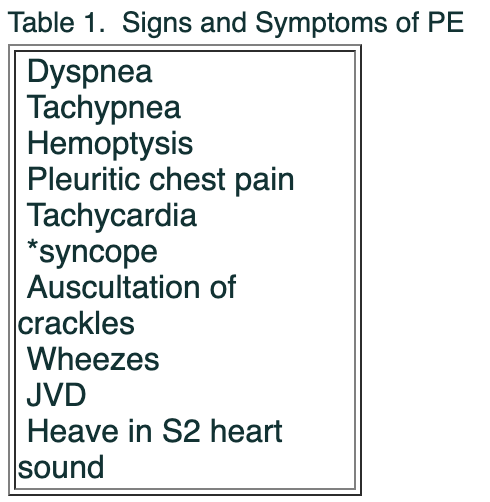
Cardiac assessment may reveal findings suggesting right ventricular strain (i.e. jugular venous distention). Auscultation of the heart sounds may identify loud pulmonic valve closure (P2) as part of the second heart sound (S2), also called a heave. The ECG is useful in the differential diagnosis, particularly in ruling out myocardial infarction. In pulmonary embolism it may be normal or reveal sinus tachycardia. Changes indicating acute right heart strain, such as right axis deviation or P pulmonale and PVC’s and PAC’s are common findings. Insertion of a pulmonary artery catheter will generally reveal an increased PAP, increased CVP, and a normal or low pulmonary capillary wedge pressure (PCWP).
Differential Diagnosis:
The diagnosis of PE requires a high level of clinical suspicion, and the appropriate use of investigations. The differential diagnosis of PE includes pneumonia, atelectasis, heart failure, acute myocardial infarction (MI), and septic shock.
The chest X-ray is often normal, or it may show only non-specific abnormalities, such as signs of volume loss or pleural effusion. Pulmonary vascular distention may be caused by pulmonary hypertension. A subtle, localized vascular narrowing in the areas of decreased perfusion distal to the emboli may be seen (Westermark’s sign). The chest X-ray is useful in identifying an alternative diagnosis, such as pneumonia, pneumothrorax, pulmonary edema, or pleural effusion.
Because ECG changes are typically transient, serial tracings are often helpful in diagnosing or excluding acute MI. Changes seen most often with PE include P pulmonale, right bundle branch block, right axis deviation, and supraventricular tachycardia.
The serum D-dimer level is useful for the exclusion of PE. Patients with PE often have an elevated D-dimer, however this is also the case for a wide variety of conditions, such as trauma, surgery, malignancy acute myocardial infarction, pneumonia, and heart failure. The two most useful D-dimer results are, 1) a normal level, which will exclude the likelihood of PE, or 2) an elevated level with no other systemic illness, which will raise the suspicion of PE. Ultrasonography of lower extremities may be useful in detecting the presence of lower-extremity DVT—which helps confirm the likelihood of PE. Ultrasound is highly accurate in symptomatic DVT (i.e. pain, swelling).
Lung ventilation/perfusion (V/Q) scans use IV injection of particles of biodegradable albumin labeled with technetium 99m. These particles ultimately lodge in the small precapillary arterioles of both lungs. Healthy patients have an even distribution of ventilation and perfusion. Typical findings of a pulmonary embolus include normal ventilation, but segmental defects in perfusion. Matching defects of ventilation and perfusion, such as those that occur with pneumonia, are non-diagnostic of pulmonary embolism. A normal scan rules out the possibility of pulmonary embolism. Normal ventilation in the presence of at least two segmental defects or one lobar defect in perfusion indicates a high probability of pulmonary embolism. (Graphic to follow)
Spiral computed tomography scan (spiral CT scan) is a more recent alternative to the V/Q scan. Spiral CT scan obtains multiple cross-sectional images of the organs and tissues of the chest. CT produces images that are far more detailed than a conventional chest x-ray. It can simultaneously show many different types of tissue, including the lungs, heart, bones, soft tissues, muscle and blood vessels and captures images from many angles. The images are then used to create cross-sectional pictures or “slices” of the area of interest.
Computed pulmonary angiography (CPA) is the diagnostic gold standard for pulmonary embolus and can accurately demonstrate the extent of vascular involvement. A radiopaque contrast is introduced via a catheter into the pulmonary artery (PA) and radiographs are taken as it circulates. Two signs are diagnostic of pulmonary emboli: 1) abrupt cut-off of a vessel and 2) intraluminal filling defects. Angiography requires catheterization of large veins and catheter manipulation through the right heart. Because there are high complications are associated with such maneuvers, pulmonary angiography should be a last resort.
Treatment:
During the initial thromboembolic event, treatment is supportive. Airway management and oxygen administration are paramount in the treatment of acute PE. O2 therapy is indicated when arterial hypoxemia is present. Continuous O2 should be given by mask or cannula, in a concentration sufficient to raise PaO2 and SaO2 blood pressure may be supported with judicious IV fluid administration and a vasopressor may be indicated. Analgesics are given if pleuritic pain is severe. Although anxiety is often prominent, sedatives should be prescribed cautiously. Appropriate drugs may be useful in converting and preventing supraventricular tachyarrhythmias. A flow-directed balloon pulmonary artery (Swan-Ganz) catheter can be used to determine pulmonary artery and wedge pressures, mixed venous blood O2 saturation and/or content and cardiac output.
Treatment after massive PE, particularly with hypotension, may involve thrombolytic therapy. Streptokinase, urokinase, reteplase, and tissue plasminogen activator (TPA) all enhance the conversion of plasminogen to plasmin, the active fibrinolytic enzyme. Contraindications to thrombolytic therapy include intracranial bleeding, recent stroke, active bleeding from any source, pregnancy, and surgery within the preceding several weeks. All patients undergoing thrombolytic therapy have an increased risk of bleeding, particularly from recent operative wounds, needle puncture sites, sites of invasive procedures, and the GI tract. Thus, invasive procedures should be avoided. Pressure dressings are usually required to stop oozing; serious bleeding requires stopping the thrombolytic drug and administering fresh frozen plasma or heparin antagonists (protamine sulphate). Periodic platelet counts together with hematocrits and tests for occult blood in stool, are recommended.
Surgical pulmonary embolectomy should be considered when there are no other treatment options, and the patient has a likely fatal massive PE. Indications for embolectomy include, massive PE with shock, thrombolytic agents are contraindicated, and patients who fail thromboysis. Angiographic confirmation of PE is strongly advised before embolectomy.
Prognosis:
Mortality after the initial thromboembolic event varies with the extent of PE and the patient’s preexisting cardiopulmonary status. The likelihood that a patient with markedly compromised cardiopulmonary function will die after significant PE is high (probably > 25%). However, a patient with normal cardiopulmonary status is unlikely to die unless the occlusion exceeds 50% of the pulmonary vascular bed. When the initial embolic event is fatal, death often occurs within 1 to 2 hours. The likelihood of a recurrent embolus in an untreated patient is about 50%, and as many as half of these recurrences may be fatal. Anticoagulant therapy reduces the rate of recurrence to about 5%; only about 20% of these will be fatal.
Prevention:
Prophylaxsis is the most important management aspect of DVT, and subsequent PE. The use of mobilization, graduated compression stockings, pneumatic compression devices, low-molecular weight heparin (LMWH), and even the insertion of an IVC filter may be indicated. The choice will depend on the underlying condition of the patient, and on the risk factors present for PE.
References: #
- Beers, Mark H. (M.D.); Berkow, R. (M.D), editors. The Merck Manual of Diagnosis and Therapy (seventeenth edition) 1999. Merck Research Laboratories, Whitehouse Station, N.J.
- Bernsten, A., and Soni, Oh’s Intensive Care Manual (5th Edition) 2003. N. Elsevier Ltd., London, England.
- Fink, M., Abraham, E., Vincent, JL., Kochanek, P. Textbook of Critical Care (5th edition) 2005. Elselvier Suanders, Philadelphia, Pennsylvania.
- Goldhaber SZ, Morrison RB. Cardiology patient pages. Pulmonary embolism and deep vein thrombosis. Circulation 2002; 106(12).
- Wood KE. Major pulmonary embolism: review of a pathophysiologic approach to the golden hour of hemodynamically significant pulmonary embolism. Chest 2002;121(3):877–905.