Description #
This unit is designed to help health care professionals develop a better understanding of the goals and components of patient self-management education in Chronic Obstructive Pulmonary Disease (AECOPD).
Learning Objectives #
By the end of this unit, you should be able to:
1. Explain the goals of patient self-management education in COPD Management
2. List the components of patient self-management education in COPD Management
3. Explain the purpose of a COPD Action Plan
Introduction #
Disease self-management education is important to the successful treatment of any chronic disease, and it is a key component of any COPD management plan.
Self-management refers to the ability of the patient to adapt to changes in their health status and cope effectively with their disease in at home. Patient education should provide patients with the knowledge and skills necessary to manage their own health and maintain an active and satisfying life . Education should also be individualized based on the patient’s learning needs and disease severity and it should include family members and caregivers whenever possible.
COPD self-management education may be provided by a variety of healthcare providers in both acute and community settings, including:
- Family doctors
- Respiratory therapists
- Nurses
- Physiotherapists
- Occupational therapists
- Pharmacists
As well as being able to provide self-management education to their patients, healthcare providers should be aware of the COPD resources and patient education materials accessible in their community. Clinicians and educators should ensure that referrals to the appropriate community resources are made, including pulmonary rehabilitation programs, smoking cessation counselors and other community services as appropriate.
This unit will identify the goals of COPD self-management education as well as some of the barriers to learning self-management skills. It will also discuss some of the main topics in COPD self-management. As well, resources including PDFs, videos, and web links are provided throughout this unit to assist clinicians in providing self-management education to COPD patients and their families.
Goals #
Some of the goals of disease self-management education include:
Decreased healthcare utilization:
Reduced number of emergency room visits and hospitalizations
– Reduced length of hospital stay
reduced exacerbations through enhanced self-care and improved ability to recognize flare-ups early.
improved compliance with treatment an active involvement in treatment
Patient satisfaction
improved or maintained QOL
– Increased self-confidence and autonomy; By understanding its pathophysiology and learning as much as you can about treatment options, you can help your patients stay independent as long as possible.
– Maintain periods of wellness and improve ability to recognize flare-ups early
– Improved symptom management
– maximized function
-Educate them about COPD pathophysiology, including how lung changes relate to symptoms.
Topics in Self-Management Education #
The skills that COPD patients require to self-manage their disease typically fall under the following topics:
- Medication knowledge (Including inhaler technique and oxygen therapy)
- Smoking cessation strategies
- Avoiding Exacerbations (Including use of Action Plans)
- Controlling breathlessness and anxiety
- Excercise
- Nutrition
- Oxygen Therapy
The remainder of this unit examines each of these topics in more detail and provides educational resources that may be useful for clinicians and their COPD patients.
Medication Knowledge #
Oxygen therapy
inhalers
inhaler technique
Provide education on prescribed medications, covering proper use of inhaled drugs (including spacers if indicated), proper sequence for taking medications to maximize their effects, and adverse effects. Make sure patients know how to determine the amount of inhaled medications left so they can avoid running out. Stress the importance of getting pneumococcal and influenza vaccines.
Inhaler Technique #
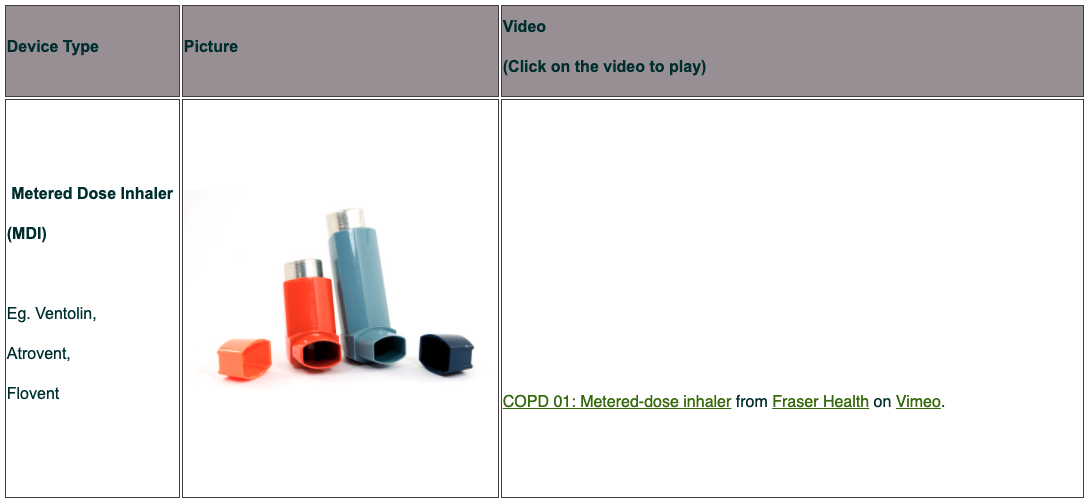
COPD 01: Metered-dose inhaler from Fraser Health on Vimeo.
COPD 02: Metered-dose inhaler with spacer device from Fraser Health on Vimeo.
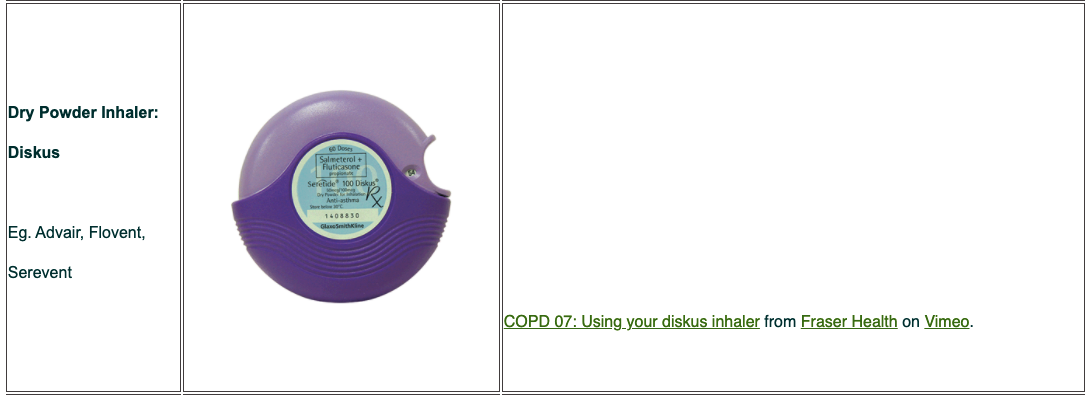
COPD 07: Using your diskus inhaler from Fraser Health on Vimeo.
Smoking Cessation #
Smoking cessation is the single most effective — and cost effective — intervention in most people to reduce the risk of developing COPD and stop its progression.
Counseling delivered by physicians and other health professionals significantly increases quit rates over self-initiated strategies. Even a brief (3-minute) period of counseling to urge a smoker to quit results in smoking cessation rates of 5-10%. Numerous effective pharmacotherapies for smoking cessation are available and pharmacotherapy is recommended when counseling is not sufficient to help patients quit smoking.
Brief Strategies to help the patient willing to quit:
- ASK Systematically identify all tobacco users at every visit
- ADVISE Strongly urge all tobacco users to quit
- ASSESS Determine willingness to make a quit attempt
- ASSIST Aid the patient in quitting
- ARRANGE Schedule follow-up contact
Brief Strategies to Help the Patient Willing to Quit
ASK
- Systematically identify all tobacco users at every visit
- Every patient at every visit should have tobacco-use queried and documented
ADVISE:
- Strongly urge all tobacco users to quit In a clear, strong, and personalized manner
ASSESS:
- Determine willingness to make a quit attempt Ask every tobacco user if he/she is willing to make a quit attempt
ASSIST:
- Aid in the patient quitting. Help with a quit plan, provide practical counseling (or refer to smoking cessation support person if available), help the patient obtain extra-treatment social support
ARRANGE:
- Schedule follow-up contact (ex. QuitNow fax referral form)
More information on community smoking cessation support programs can be found through the BC Lung Association website: www.bc.lung.ca
Smoking cessation is the single most effective intervention to reduce the risk of developing COPD and the only intervention that has been shown to slow its progression. It should be noted 70% of smokers visit a physician each year and advice from a physician is an important motivator to quit. Advice from physicians, health professionals and individual and group counseling has been shown to increase cessation rates. Stopping smoking produces only a small improvement in the FEV1 but the subsequent rate of decline returns to that of a non-smoker, thus helping to avoid disability or death depending on the time of cessation. MOH: Smoking is the most important cause of and contributing factor for COPD progression. Smoking cessation is the most important factor in slowing the progression of COPD. Smoking cessation is effective in preventing disease progression even in long-term smokers. Effective strategies exist to aid in smoking cessation. These include: nicotine replacement therapy which may need to be used long term other pharmacotherapy (note that these have significant side effects) Even minimal intervention may be helpful and should be offered to every smoker. Counselling may be appropriate. Consider referral of the smoker with COPD to the BC Smokers Helpline (refer Patient Guide). Smoking cessation of the patient and household contacts should be reinforced at every contact.
For additional information, refer to the guideline Cardiovascular Disease – Primary Prevention, Appendix A – Part 1:
Smoking Cessation available at www.BCGuidelines.ca
– Smoking cessation has the greatest capacity to influence the natural history of COPD.
– Health care providers should encourage all patients who smoke to quit.
– Pharmacotherapy and nicotine replacement reliably increase long-term smoking abstinence rates.
– Counseling delivered by physicians and other health professionals significantly increases quit rates over self-initiated strategies. Even a brief (3-minute) period of counseling to urge a smoker to quit results in smoking quit rates of 5-10%.
– Nicotine replacement therapy (nicotine gum, inhaler, nasal spray, transdermal patch, sublingual tablet, or lozenge) as well as pharmacotherapy with varenicline, bupropion, and nortriptyline reliably increases long-term smoking abstinence rates and are significantly more effective than placebo. Smoking Cessation Requires Multiple Attempts Reducing the risk from indoor and outdoor air pollution is feasible and requires a combination of public policy and protective steps taken by individual patients Reduction of exposure to smoke from biomass fuel, particularly among women and children, is a crucial goal to reduce the prevalence of COPD worldwide
Avoiding Flare-ups #
Potential strategies to avoid acute exacerbations of COPD include:
smoking cessation
Vaccinations (Influenza annually, pneumococcal every 5-10 yrs)
Self management education with a written action plan
Regular long-acting bronchodilators
Regular therapy with ICS/LABA
Oral corticosteroid for moderate to severe AECOPD
Pulmonary rehabilitation
encourage patients to stay indoors when air quality is poor, as air quality may have a significant effect on COPD
Reinforce the importance of good infection control, such as frequent hand washing and avoiding crowds when upper respiratory infections are prevalent.
Teach patients to observe their usual symptoms and to contact their healthcare provider when symptoms worsen.
Action Plans #
Data is now emerging to demonstrate the benefit of a self-management plan for patients who exacerbate frequently. The earlier treatment is started during an exacerbation, the better. Patients need to be advised to take action promptly. All patients need clear, written information about what to do and how to contact medical help.
Should address issues related to self-assessment of disease, related changes, how to recognize symptoms of a flare-up, how to self-manage exacerbation symptoms and when to seek help.
Patient must be able to recognize signs and symptoms of an exacerbation, and according to the change in symptoms, they should be able to respond with immediate adjustments to treatment
must have confidence to cope with their diseaseand manage symptoms.
The key elements of a self-management plan are:
- How to recognise an exacerbation
- What to do about it
- When and how to call for medical help
Some patients benefit from a self-management plan that includes stand-by courses of antibiotics and oral corticosteroids, so that they can initiate therapy. They should be advised to contact their doctor as well so that the use of these drugs can be effectively monitored and further advice given, as necessary.
Controlling Breathlessness #
This page explains the main medicines used to treat COPD and how they can help your symptoms.
COPD medicines cannot cure COPD, but they can improve your symptoms. By taking the right medicine at the right time, you can:
- be more active
- have less coughing and shortness of breath
- get fewer flare-ups
Shortness of breath on exertion is the most common presenting symptom and is also distressing and disabling.
Increasingly severe breathlessness not infrequently leads to exercise avoidance. The patient then enters a downward spiral of inactivity, loss of fitness and increasing disability. Eventually normal activities of daily living become difficult or impossible, and social isolation, loss of role and self-esteem follow.
It is not surprising that anxiety and clinical depression are common in patients with COPD, particularly amongst those who are significantly disabled by breathlessness.
“But dyspnea is more than just a physiologic phenomenon. It also has psychophysiologic components, triggered by such factors as anxiety and fear. Persons with COPD fear the sensation of dyspnea that results from inefficient breathing. Therefore, they avoid exercise; as dyspnea progresses, they begin to abandon activities, leading to a downward spiral of disability. Ultimately, they suffer increasing dyspnea even at rest.”
- Write a list of all the medicines you take so that your health care providers can check for possible drug interactions. If you take over-the-counter medicine or natural health products, write those down too. They could interact with your medicines and make your breathing worse.
- Go to the same pharmacy for all your medicines. If you fill all your prescriptions at the same place, your pharmacy record will show all the medicines you’re taking. This way the pharmacist can make sure you’re not taking any medicines that interact badly together.
- Make sure you can tell the difference between your inhalers, and make sure you know how to use them properly. You may use several different inhalers for the different medicines you take. You can tell the inhalers apart by their names and colours. Make sure you know which is your quick relief medicine to take when you’re short of breath. Keep it with you at all times.
- Work with your doctor to decide the best way to treat your COPD symptoms. Talk about your symptoms, activities and concerns. Tell the doctor how you think your medicines are working. Ask questions. Keep asking questions until you’re sure you understand.
- Speak up if you’re worried about side effects. Like all medicines, COPD medicines may cause side effects. If you have concerns, talk to your doctor, pharmacist or certified respiratory educator. They can help you understand the pros and cons of each treatment.
- Ask your doctor for a written COPD action plan to help you manage COPD flare-ups. This action plan will explain what to do if you notice your COPD symptoms getting worse. Follow your COPD action plan. To get a blank COPD action plan for your doctor to fill out, click here (PDF).
- Visit a COPD clinic to learn more about your COPD medicines and how to take them. Ask your doctor about COPD clinics in your area or find COPD clinics in your area by searching in our online directory.
Coping suggestions #
To help patients manage dyspnea, teach them about activities that reduce or control it, as described below.
- Breathing techniques. Techniques such as pursed-lip breathing help reduce respirations while improving the expiratory phase (by increasing laminar flow of expired air). Tell the patient that slow, controlled expiration postpones small-airway collapse, thereby reducing air trapping that occurs with forced expiration.
- Proper positioning. Explain that the tripod position, in which the patient sits or stands leaning forward with the arms supported, forces the diaphragm down and forward and stabilizes the chest while reducing the work of breathing. If the patient reports increased dyspnea when performing activities of daily living (ADLs), especially when raising the arms above the head, recommend supporting the arms during ADLs, as by resting the elbows on a surface. Point out that this reduces competing demands of the arm, chest, and neck muscles needed for breathing.
- Energy-conservation techniques. Advise patients to pace activities, take frequent rests, use assistive devices, and break activities into smaller tasks to help reduce dyspnea development.
Also help identify the patient’s best “breathing time” of the day, and recommend reserving strenuous activities for this period. Finally, stress the need to avoid environmental triggers of dyspnea, including temperature extremes and exposure to air pollution, pollen, cigarette smoke, chemical fragrances, and dust.
Breathing exercises for COPD help you strengthen breathing muscles, get more oxygen, and breathe with less effort. Here are two examples of breathing exercises you can begin practicing. Work up to five to 10 minutes, three to four times a day.
Pursed lip breathing:
- Relax your neck and shoulder muscles.
- Breathe in for two seconds through your nose, keeping your mouth closed.
- Breathe out for four seconds through pursed lips. If this is too long for you, simply breathe out twice as long as you breathe in.
Use pursed-lip breathing while exercising. If you experience shortness of breath, first try slowing your rate of breathing and focus on breathing out through pursed lips.
Diaphragmatic breathing:
- Lie on your back with knees bent. You can put a pillow under your knees for support.
- Place one hand on your belly below your rib cage. Place the other hand on your chest.
- Inhale deeply through your nose for a count of 3. (Your belly and lower ribs should rise, but your chest should remain still.)
- Tighten your stomach muscles and exhale for a count of six through slightly puckered lips.
INTRODUCTION
Dyspnea is an important and debilitating symptom in patients with chronic obstructive pulmonary disease (COPD) [1]. Some pathophysiological factors known to contribute to dyspnea include (1) increased intrinsic mechanical loading of the inspiratory muscles, (2) increased mechanical restriction of the chest wall, (3) functional inspiratory muscle weakness, (4) increased ventilatory demand related to capacity, (5) gas exchange abnormalities, (6) dynamic airway compression, and (7) cardiovascular effects [2]. The relief of dyspnea is an important goal of the treatment of COPD, an irreversible airway disease. In addition to some conventional treatments, such as bronchodilator therapy, exercise training, and oxygen therapy, controlled breathing is also applied to alleviate dyspnea.
Controlled breathing is an all-embracing term for a range of exercises, such as active expiration, slow and deep breathing, pursed-lips breathing (PLB), relaxation therapy, specific body positions, inspiratory muscle training, and diaphragmatic breathing. The aims of these exercises vary considerably and include improvement of (regional) ventilation and gas exchange, amelioration of such debilitating effects on the ventilatory pump as dynamic hyperinflation, improvement of respiratory muscle function, decrease in dyspnea, and improvement of exercise tolerance and quality of life. In patients with COPD, controlled breathing is used to relieve dyspnea by (1) reducing dynamic hyperinflation of the rib cage and improving gas exchange, (2) increasing strength and endurance of the respiratory muscles, and (3) optimizing the pattern of thoracoabdominal motion. In addition, psychological effects (such as controlling respiration) might also contribute to the effectiveness of controlled breathing (however, these effects are not discussed in this overview).”
http://www.rehab.research.va.gov/jour/03/40/5Sup2/Gosselink.html
see above website for more description of breathing techniques!!!!!
Excercise #
All patients with COPD benefit from regular physical activity and should be encouraged to remain active.
Remaining active despite symptoms of shortness of breath must remain a priority for all patients with COPD. Clinically stable COPD patients whose activities remain symptom-limited despite optimal therapy should be referred to an exercise training program. Formal pulmonary rehabilitation programs that include patient education and exercise can reduce symptoms, decrease exacerbations, and improve exercise endurance and quality of life.
All COPD patients should be encouraged to maintain, and preferably increase, their every-day level of activity, within the limits of any co-morbidity.
Reassure them that breathlessness is not harmful and that regularly getting moderately out of breath is beneficial. Many patients avoid exercise because of fear that breathlessness is harming their heart or lungs
Patients with mild disease may benefit from referral to a local exercise promotion scheme.
Patients who are overweight (BMI >25) should be advised and supported to lose weight, since weight loss can improve their exercise capacity.
Remaining active despite symptoms of shortness of breath must remain a priority for all patients with COPD. Clinically stable COPD patients whose activities remain symptom-limited despite optimal therapy should be referred to an exercise training program. Formal pulmonary rehabilitation programs that include patient education and exercise can reduce symptoms, decrease exacerbations, and improve exercise endurance and quality of life.
Nutrition #
Patients who have difficulty maintaining weight should consult…a webpage:
“Besides understanding how to properly use your medications and learning ways to reduce your risk of developing flare-ups, it’s important to maintain your body’s strength and muscle mass to order to support healthy breathing. That means checking your weight regularly, seeking nutritional advice from your physician, and exercising in order to maintain muscle strength. If you have late-stage COPD, maintaining body weight is even more crucial….maintaining your weight is more important than ever, as you need to preserve the muscles in your diaphragm in order to help you breathe.
There are many reasons why people with COPD, especially those with emphysema, may begin to lose weight and muscle mass. It’s very common for those with breathing problems to exercise less often because they feel tired or fatigued, which may decrease appetites. Patients with COPD and other respiratory diseases also often suffer from co-morbid diseases, such as depression, which can also contribute to weight loss. In addition, excess carbon dioxide in the blood (a symptom usually noted in those with emphysema because the body cannot exhale as fully to “push out” waste gases) can make you feel exhausted all the time because your body is using more and more of its energy to breathe. In fact, according to a recent study in the journal Chest, late-stage COPD patients with emphysema could be using as much as 20 percent more energy at rest than healthy individuals.
Complications of Weight Loss
Weight loss and decreases in muscle mass could lead to more serious complications in the lives of those with COPD, including a rise in infections, such as pneumonia.
Nutritionally depleted COPD patients have lower respiratory and skeletal muscle strength than non-depleted patients.Besides malnutrition, commonly used drugs in COPD may also contribute…
Causative factors for respiratory muscle dysfunction in COPD include disturbances in electrolytes,4hypercapnia,5 forward failure,6 and prolonged use of oral corticosteroids.7 In addition, the altered geometry of the thorax in severe emphysema compromises the ventilatory pump function of the diaphragm.8 Malnutrition, which frequently occurs in moderate to severe COPD,9 could also play a part in respiratory muscle dysfunction. Recent studies have indicated that wasting of fat free mass in COPD is associated with peripheral skeletal muscle weakness.10 However, few data are available regarding the effects of malnutrition on respiratory muscle strength
“COPD patients commonly have problems maintaining adequate nutritional intake. As the disease progresses, many experience cachexia. Inform patients with reduced nutritional status that the primary-care provider is likely to monitor their hemoglobin and serum albumin levels. To improve their nutritional status, advise them to eat small, frequent meals high in protein and avoid gas-producing foods. Instruct them to monitor their weight and food intake. If recommended, advise them to use high-calorie nutritional supplements”
Oxygen Therapy #
Teach patients who need oxygen therapy about the following:
- proper oxygen use, including the importance of avoiding nearby open flames
- oxygen prescription instructions
- correct equipment care
- back-up oxygen system in case of a power outage.
Oxygen delivery systems include liquid oxygen, compressed gas, and concentrators. Each system carries risks and benefits. Selection hinges on patient mobility and functional goals.
Portable oxygen concentrators are the newest innovation in oxygen delivery, eliminating the need for patients to carry oxygen with them. These devices have been shown to be safe and effective. In 2005, the Federal Aviation Administration adopted new rules that allow patients to fly with portable concentrators. However, the rule doesn’t require airlines to allow these systems on board; therefore, instruct patients to check with the airline regarding oxygen use when planning travel.
Other Topics #
Psychosocial issues: frustration, fatigue, pain and isolation, depression
Psychosocial concerns for COPD patients include increasing dependence on others, lack of control over symptoms, and decreased energy. Also, they’re at high risk for depression and anxiety because of symptom burden and functional limitations. These problems can affect their social interactions, role perception, and physical abilities.
Help them verbalize their feelings and develop healthy coping behaviors. However, know that as increasing dyspnea makes talking more difficult, conversation may grow burdensome.
Include family caregivers in your discussions when appropriate. If the patient has significant psychosocial issues, consider a referral to a social worker, psychologist, or psychiatrist.
Sexual intimacy is an area commonly overlooked by healthcare providers. COPD can decrease certain aspects of sexual functioning. Males may develop erectile dysfunction as lung function declines. What’s more, the physical exertion of sexual activity leads to dyspnea in most COPD patients. The effort required for intercourse resembles that needed to climb one flight of stairs at a normal pace. However, point out that sex doesn’t increase blood pressure, heart rate, or respiratory rate to dangerous levels. (For patient teaching related to sexual activity, see Teaching patients about sexual intimacy by clicking on the PDF icon above).
COPD is increasing in prevalence and burden worldwide. By understanding its pathophysiology and learning as much as you can about treatment options, you can help your patients stay independent as long as possible.
Sexuality,
Travel,
leisure, sleep, psychosocial, end-of life issues (advanced directives)
References #
BC Ministry of Health