Description #
This unit will provide the required information to the RN/RT on how to appropriately select patients for PSA to prevent unanticipated events,
identify pre-sedation risk factors, and on how to develop
an anaesthetic plan for each individual
Learning Objectives #
At the end of the module the student must be able to :
a) Describe and perform a detailed baseline patient assessment
b) Understand the different ASA levels and describe how they relate to a patients risk factor for receiving sedation
c) Understand the rationale for, and be able to identify patient suitablity for receiving sedation
PROCEDURAL SEDATION AND ANALGESIA (PSA)
Allows the patient to undergo diagnostic and interventional procedures safely and in a comfortable manner
Intravenous sedation has proven to improve patient satisfaction and procedural outcomes
PRESCREENING
PROCEDURAL SEDATION AND ANALGESIA (PSA)
Allows the patient to undergo diagnostic and interventional procedures safely and in a comfortable manner.Intravenous sedation has proven to improve patient satisfaction and procedural outcomes
WHY PRESCREENING IS IMPORTANT
- Appropriate patient selection to prevent unanticipated events
- Identify pre-sedation risk factors
- Develop an anesthetic plan for each individual
GOALS OF PRESCREENING
- Review patient’s health history
- Identify risks factors prior to admission
- Evaluate need for consult with Anesthesiologist or other specialist
- Potential to optimize patient’s health prior to procedure
- Provide communication tool between nursing and physician
- Inform and educate patient of plan for procedure thereby reducing anxiety and maximizing patient safety and satisfaction
- Obtain informed patient consent by explaining the benefits and risks of the procedure prior to admission
- Ensure patient has a responsible adult to escort him/her home after a scheduled procedure
PRESCREENING CRITERIA
a)Age:
Patient >65 years tend to have a longer medical history increasing prevalence to organ dysfunction
Patient >65 years tend to have a longer medical history increasing prevalence to organ dysfunction
b)Medical history and physical exam:
Completed by surgeon or family physician detailing systemic disease involvement, compliance of medications prescribed, over the counter vitamins and herbal supplements
c)Need for diagnostic testing:
Findings from the physical examination and patient history may require further investigation such as ECG, laboratory testing
Findings from the physical examination and patient history may require further investigation such as ECG, laboratory testing
d)Informed Consent:
Patient aware of the plan, benefits, risks and side effects of medications used
e)Anaesthetic plan:
Assess the overall health status of person
f)Allergy status:
Give a clear history of reactions to medications, food and latex, contrast agents
Age:
Patients 65 years and older have increased prevalence to organ dysfunction and health problems
Because aging alters renal and hepatic metabolism, medication metabolism will also be affected, potentially resulting in prolonged drug effects
Central nervous system is more sensitive to medications, so smaller doses are usually requiredMedical History:
Requires 2 sources – patient interview by the surgeon or family physician and medical chart
Evaluate various organ systems and history that are essential to planning sedation and or analgesics
Document history of difficult airway management
Document drug use including prescription, over the counter, vitamin / herbal supplements. Some of these agents may prolong the effects of sedation and increase the amnesic effect
Allergy status – important to clearly document the allergenic substances (drugs, food, latex, contrast agents) and their reactions in order to avoid exposure to them
Need for Diagnostics – findings from medical history and physical exam may require further investigations such as ECG, blood work, chest x-rays, etc.
Anesthetic Plan:
Nurse assess patient’s overall health status (ASA score) and develops an individualized PSA plan
NPO status:
Important to be specific about what this means for the patient
NPO means no food, no fluids
Follow hospital policy for NPO status
Recommendation:
***No solid food or full fluids for 6 -8 hours and no clears fluids for 3-4 hours prior to PSATake prescribed medications as usual-if in doubt, bring them in with you
Informed Consent:
Informed consent will reduce anxiety level
Patient should be aware of the plan for the day of procedure
Risks and benefits of surgery and PSA have been explained by surgeon prior to admission
- REASONS FOR COMPLICATIONS DURING PSA
- Inappropriate patient selection: follow the guidelines for ASA classifications as pertains to non- anesthetists
- Unanticipated events or responses from patient or equipment: RN should fully understand the equipment being used and its limitations and have the ability and knowledge to react quickly
- Overmedication: RN requires a solid knowledge base in pharmacology and an understanding of the many factors (age, weight, history) which impact effects of PSA
PRE SEDATION INSTRUCTIONS
Instructions must be pertinent to the planned procedure and administration of PSA.Also to prevent delay or cancellation of the procedure the patient must be given instructions about:
- Length of procedure
- Arrival time
- NPO status
- Medications
- Procedure guidelines about bowel preparation
- Prophylactic antibiotics, clothing, contrast agents
- Responsible adult to accompany patient home
- PATIENT ASSESSMENT
On the day of surgery, it is necessary for the RN to:
- Review patient history with patient as a significant amount of time may have lapsed since physician’s physical assessment and health may have changed
- Review medications for changes
- Make inquiry into how well patient understands the procedure and the delivery of Procedural Sedation
- Assess anxiety level
- Ensure the patient has a responsible adult to accompany them home postop
Measures to reduce anxiety are:
- Provide a peaceful environment
- Use a calm & unhurried pace so patient does not feel rushed
- Provide an explanation of all steps
- Have quiet music playing in background
- If patient anxious, have surgeon speak with patient prior to procedure
American Society of Anesthesiologists (ASA) Physical Classification System
The ASA classification system was developed in 1940 by the American Society of Anesthetists to standardize physical status and to assign potential risk classification for surgical intervention
This classification system was developed for anesthesiologists but is now used by RNs to determine appropriate patient selection for sedation and analgesia
Patients classified as ASA 1 or 2 are appropriate for monitoring by an RN
ASA 3 patient must be assessed on an individual basis to determine if systemic disease is stable; some patients may benefit from anesthetic consult
ASA CLASSIFICATION SYSTEM
ASA 1: A normal healthy patient
A normal healthy patientASA 2: A patient with mild systemic disease
A patient with mild systemic diseaseASA 3: A patient with severe systemic disease
A patient with severe systemic diseaseASA 4: A patient with severe systemic disease that is a
constant threat to life
A patient with severe systemic disease that is a constant threat to lifeASA 5: The moribund patient who is not expected to
survive 24 hours with or without surgery
The moribund patient who is not expected to survive 24 hours with or without surgery ASA 1:
Healthy, good exercise tolerance
Eg: woman having fibroid embolectomy
ASA 2:
Person will have disease of one system which is well controlled with medications, no exercise limitation
E.g. : controlled hypertension, controlled diabetes without systemic effects, smoking without evidence of COPD
ASA 3:
Person with disease of one or more systems, controlled but not incapacitating
E.g.: controlled angina, old MI, poorly controlled hypertension, morbid obesity
ASA 4:
Person with poorly controlled systemic disease that is a constant threat to life
E.g.: Unstable angina, symptomatic CHF or COPD
ASA 5:
Person with critical multisystem failure
E.g.: sepsis, hemodynamic instability, coagulopathy such as DIC
LABORATORY TESTS
- Laboratory testing will depend on the policy of each facility
- Medications may need to be held (e.g.. Metformin, Coumadin)
- ECG is recommended on all people over 50 years and younger if clinically indicated
- Coagulation test such as INR/PT/PTT if patient taking anticoagulants, antiplatelet therapy, NSAID’s
- Potassium if patient is taking insulin, beta-blockers, steroids and diuretics
- Creatinine & GFR if contrast to be used
- CXR for cigarette smoker greater than 20 pack years, cardiovascular disease or Congestive heart failure (refer to institutional guidelines)
- Liver function test for alcohol and drug abuse, recent weight loss, jaundice, bleeding disorder (check with Physician)
- Hemoglobin and platelets for people with blood dyscrasia, renal disease, anemia
SOCIAL HISTORY
Social history important to discuss as some patients may not realize the impact it has on health
When discussing social history, it is important to use open ended questions / wording on Nursing assessment as you will receive more information from the patient and will not be perceived as forming an opinion about their history
E.g.: “How much alcohol do you consume in 1 week?”
Tobacco use:
Increase risk for cardiovascular and pulmonary disease
Impaired respiratory function as result of smoking history at risk for complications since ventilatory response, airway protection decreased by sedation
Narcotic/ drug use:
Require knowledge of narcotic use in order to plan sedation
Increase chance of hepatitis B&C with IV drug user
If liver disease is present due to hepatitis, drug metabolism may be abnormal; so patient may only tolerate small doses of medications
Alcohol Use:
Heavy use of alcohol increases risk for sedation management
Long term alcohol use associated with liver disease which may affect the metabolism of drugs
Alcohol use may be associated with cardiovascular and respiratory diseases such as arrhythmias
A high percentage of alcohol users smoke; therefore, increasing pulmonary risks, hypertension, stroke & respiratory distress syndrome
Need to be aware if patient has ingested alcohol prior to procedure as there is an increased incidence of a prolonged recovery and increased delirium, may need to cancel procedure if confirmed
If patient denies alcohol use and is suspected by nurse, a blood alcohol level may need to be ordered to confirm
These patients may be more difficult and anxious as they will be advised to not drink prior to procedure
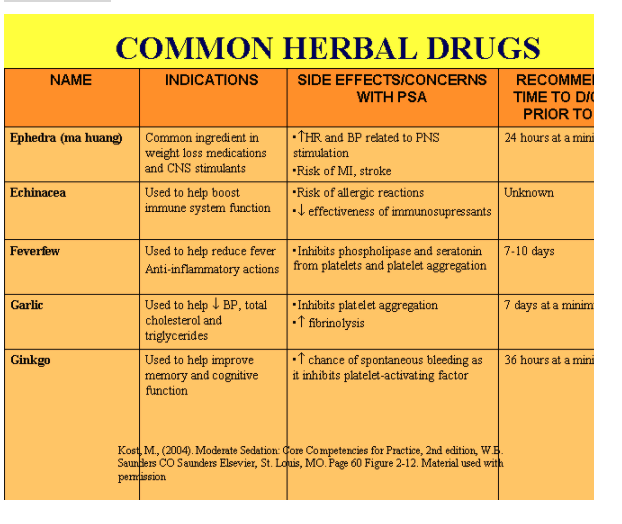
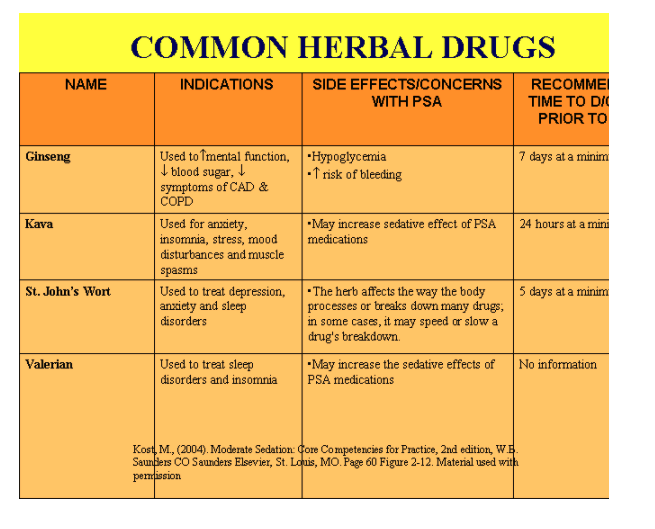
Herbal Drug use:
Many patients do not consider vitamin/herbal/ homeopathic substances to be drugs and therefore neglect to inform the physician of their use
It is important to know all the drugs the patient is taking as many of them have potentially undesirable effects related to the procedure or to the PSA medications e.g.. Anti-platelet effects, additive or antagonistic effects
It has been recommended by the ASA that all herbal medicines be discontinued 2 weeks prior to anesthesia/surgery
OBESITY
Obesity has a significant impact on cardiovascular, pulmonary, gastrointestinal, endocrine, and hepatic systems
Red flags for obesity are difficult airway due to short necks, because of increase body mass redundant oropharygneal tissue these patients must not be allow to progress into deep sedation
Prone to pulmonary aspiration due to increased gastric volume and reflux, these patient benefit from H2 blocker and gastric stimulants to increase gastric emptying time, medications such as Ranitidine and Maxeran
Obese people will benefit from supplement O2 during procedure
Cardiovascular effects:
CO and SV, hypertension
Pulmonary effects:
Pulmonary compliance, increased oxygen consumption, increased CO2 production and increased chest wall mass
GI effects:
Intra- abdominal and intra – gastric pressure, at risk of aspiration
Organ system review- Neurological System #
NEUROLOGICAL SYSTEM
Evaluation of medical history and patient assessment may guide optimization of patients health status prior to the procedure and can prevent unanticipated events
Assess for history of mental deficiency, cerebral vascular insufficiency, level of consciousness and pre- existing neurological disease
Cerebrovascular insufficiency
May present as transient attack (TIA), moderate or major strokeTIA symptoms will resolve in 24 hours
Assess frequency and severity of TIA, treatment of incidents
Document level of consciousness, slurred speech, unsteady gait and hemiparesis
Should be treated with anticoagulants or antiplatelet therapy
Seizure Disorder
Assess underlying cause of seizure, may be triggered by anxiety, non- compliance to medication, substance abuse, infection
Assess type of seizure, and last seizure
Assess compliance to medications
Should take regular medication on day of procedure
Necessary for RN to recognize signs of seizure
PULMONARY SYSTEM
Airway Assessment:
Should be done prior to PSA as this will alert the RN to potential airway problems
Grade airway using the Mallampati Classification
which provides information about how much of the pharynx is obscured by the tongue as well as the size of the tongue in relation to the size of the oral cavity
To perform the exam, have the patient:
Open their mouth as widely as possible
The airway should be classified by which oropharyngeal structures you see
Mallampati Classification: Based on what you see
Class I
Soft palate, fauces, entire uvula, tonsillar pillar
Class II
Soft palate, fauces, uvula
Class III
Soft Palate, base of uvula
Class IV
Soft palate only (uvula not seen)
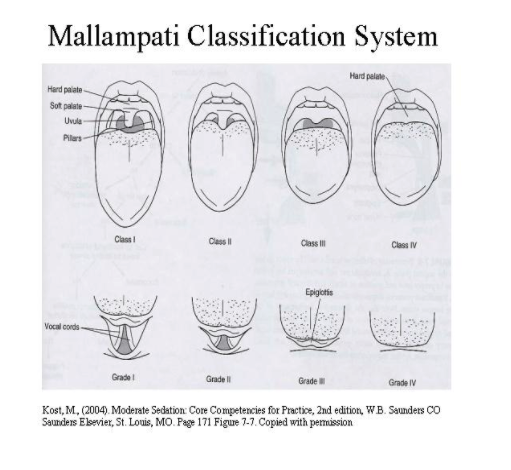
- The progression of classes from I to IV suggests increased difficulty in maintaining a patent airway without assistance during sedatio
Patients should be considered at increased risk for airway obstruction during sedation if they have a Mallampati Class III or Class IV airway
Assess for airway / respiratory / ventilation:
- difficult airway (including history of previous GA’s/PSA)
- asthma, allergies, COPD, dyspnea
- recent respiratory infections
- cough /sputum production
- history of snoring /sleep apnea, use of CPAP or supplemental oxygen
- Assess for dyspnea: inquire about activity level and shortness of breathe with activity
Red flag if the requirement for ventilation is greater than patient’s ability to respond to increase oxygen demand. This patient is not ideal for PSA and an Anesthesiologist should be consulted
- Patients should take their regular bronchodilators the day of procedure
- Smokers should attempt to stop prior to procedure
- Need to consider patient’s ability to lie flat for procedure as this position will reduce functional residual capacity therefore impede oxygenation
- COPD patient’s may be compromised
- Increase oxygen concentration as needed
- Necessary to closely observe at-risk patient’s for changes in respiratory ability such as increased respiratory rate, sternal retraction, ¯oxygen desaturation or stridor
- Sleep Apnea:
- Cessation of air movement despite ventilatory efforts for > 10 seconds
- These patients often have history of snoring and abnormal airways
- Should be seen by an Anesthesiologist before the procedure because history often involves pulmonary hypertension, stroke and cardiovascular disease such as dysrhythmias, hypertension and myocardial ischemia
- If patient uses an apparatus to sleep (CPAP, BiPAP) advise them to bring the device to hospital on the day of their procedure
- Due to increase chance of airway obstruction with sedation, can be difficult to intubate and usually require a longer recovery period post sedation
Sleep Apnea #
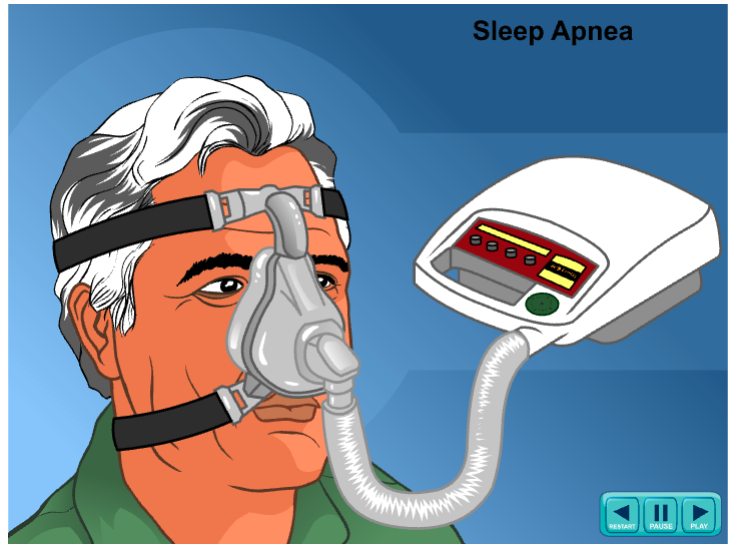
Sleep Apnea:
- Person with sleep apnea requires a device at night at prevent apnea periods.
- This device called a CPAP or BiPAP machine
- A CPAP monitor operates by pushing air through the airway at high pressure to prevent the apnea
- BiPAP monitor operates at two level of air pressure, one for inhalation and a lower level of pressure for exhalation
- the person is required to wear a maks over the nose with a tubing connected to the CPAP monitor
- Patient are asked to bring the monitors with them when admitted to hospital for surgery
CARDIOVASCULAR SYSTEM
Cardiovascular assessment provides important information about:
- Pre existing cardiovascular disease
- Disease severity, stability, treatment (previous and current)
- Presence of co morbidities (e.g. diabetes, COPD, obesity)
- Potential for inherent procedural risks
- Interventions that will decrease incidence of complications
Nurse should evaluate:
- Un/ & controlled Angina and symptomology (see slide 67)
- Chest pain
- Myocardial infarction/ischemia
- Procedures such as angioplasty, stent, pacemaker, automatic defibrillator
- Surgeries such as CABG, valve repair
- Cardiac dysrhythmias/abnormal ECG/ irregular heart rate
- Valvular heart disease, septal defects, endocarditis (may require prophylactic antibiotics)
- Daily activity level and exercise tolerance
Hypertension:
- End organs affected by hypertension are heart, brain and kidneys
- The heart is predisposed to hypertrophic changes related to working against increased vascular resistance ( > risk of ischemic heart disease, CHF)
- The brain is predisposed to hemorrhage or stroke
- Renal damage reduces glomerular filtration rate and blood flow > the risk of renal failure
When interviewing the patient it is important to assess:
- Duration of the hypertension (when initially diagnosed)
- Treatment (medication, diet)
- Compliance with treatment
- Effectiveness of the treatment
- Patient’s anxiety level
- ** Advise patient to continue their usual antihypertensive drug regime the day of their procedure**
Coronary Artery Disease (CAD):
- Myocardial ischemia develops when there is an imbalance between coronary blood flow and myocardial consumption
Assessment for CAD includes:
- Description of chest pain, tightness or heaviness, character, location, frequency, onset, duration, treatment, relief
- ** Advise patient to continue their usual BP/heart drug regime the day of the procedure)**
- Myocardial Infarction (MI):
- Important to know when MI occurred because of risk of reinfarction with surgery
- Incidence of re- infarction
- 3 months – 30%
- 3 -6 months – 15%
- 6 months – 5%
- (Tarhan et al, 1972, Steen et al, 1978)
- Therefore, it is recommended that elective procedures be delayed for 6 months after an MI
- Cardiac Dysrhythmias:
- Dysrhythmias are generally well-tolerated in people with normal cardiac reserve
Causes of dysrhythmias include:
- Hypoxemia
- Hypercarbia
- Hypotension
- Hypovolemia
- Anxiety
- Procedure-related
- Medications
- Protocol for dysrhythmias are discussed in the ECG unit
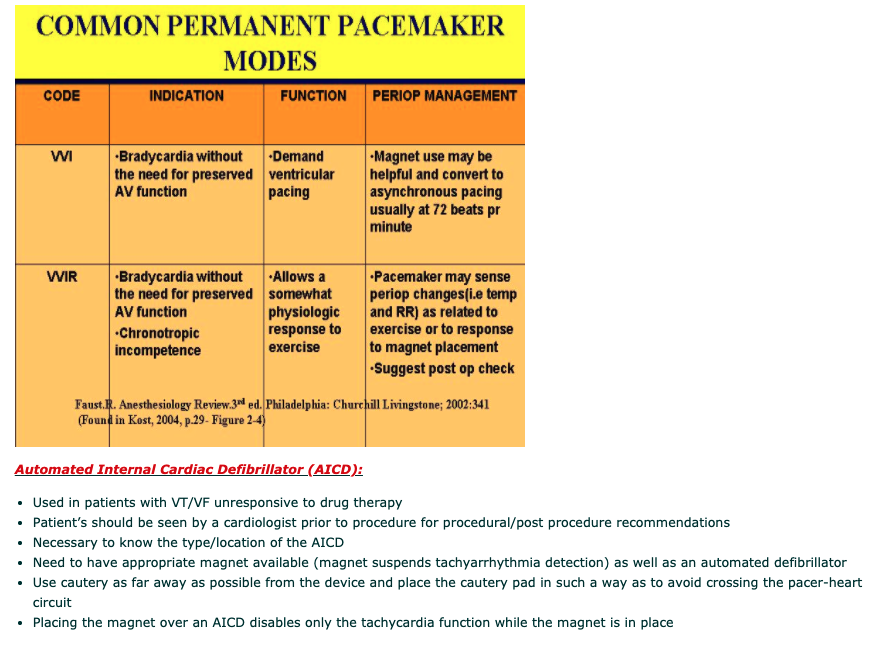
Pacemakers:
- Necessary to know type of pacemaker inserted as well as location, access of pacemaker magnet and alternate pacing modality
- If cautery is required for procedure, use bipolar rather than monopolar if possible
- Bipolar = electrical current returns directly to the generator, eliminating need for a grounding pad
- = electrical current returns directly to the generator, eliminating need for a grounding pad
- Monopolar = electrical current flows to the active electrode through the patient to the inactive electrode(grounding pad) and back to the generator. A grounding pad must be used with this form of cautery
- = electrical current flows to the active electrode through the patient to the inactive electrode(grounding pad) and back to the generator.
Pacemaker #
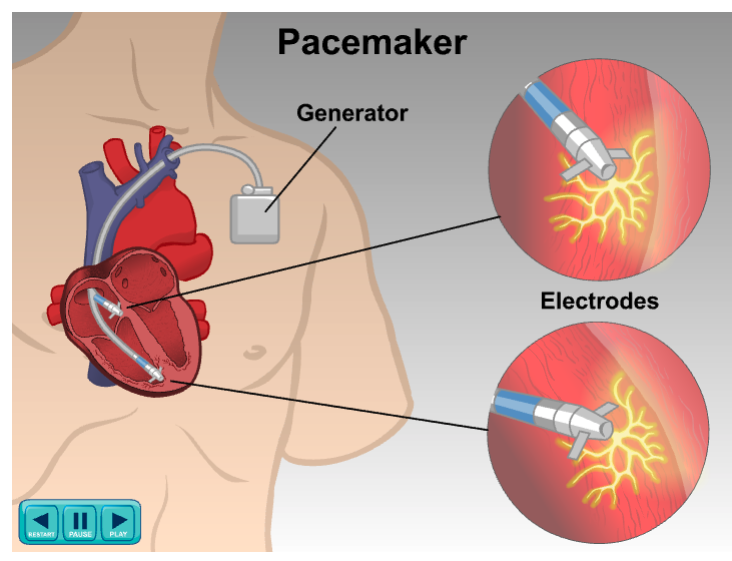
Pacemaker
- Implanted in the chest to regulate the heart’s rhythm
- Pacemaker sends electrical impulses to one or more chambers of the heart
- These impulses make the heart contract in a regular rhythm
- Used for abnormal rhythms such as Bradycardia, sick sinus syndrome, heart blocks
There are 3 types of pacemakers
- Demand pacemaker: which will monitor the rate of heart and only discharge an electrical impulse when the heart falls below programmed number of beats
- Fixed rated pacemaker: regulated with a fixed number of electrical impulses regardless of underlying heart rate
- Rate responsive pacemaker: changes heart rate according to physiological responses of the body such as respirations and physical activity
Another type of device is called implantable defibrillator used to correct rhythms that are too fast and unmanageable with cardiac medications such as anti arrhythmias
An example of irregular rhythm would be ventricular tachycardia or fibrillation
Hypertensive Heart #
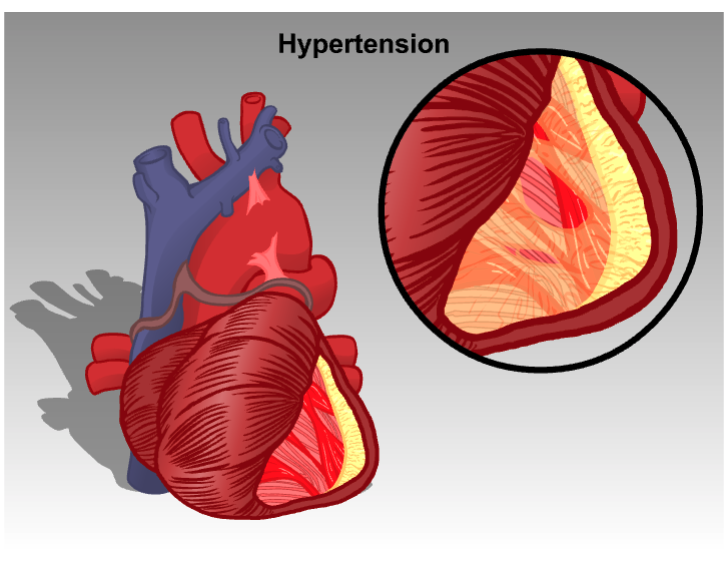
Hypertension:
- Affects 1 in 4 adults
- Is known as a silent killer as many people will have it for years prior to diagnosis
- Over time hypertension can lead to damage of blood vessels all over the body
- Hypertension can cause an abnormal widening and weakening of arteries this is called an aneurysm
- Thickening of blood vessel muscles from hypertension can cause a narrowing of the arteries therefore decreased perfusion to organs such as the brain, heart, eyes, kidneys eventually causing permanent damage or death to tissue.
- Increased prevalence to hypertension diabetes, obesity, increased cholesterol and previous myocardial infarct or stroke
Uncontrolled & increased hypertension can lead to variety of changes in the heart such as changes in the myocardial structures (left ventricular hypertrophy), coronary vasculature changes (atherosclerosis), and changes in the conduction system of the heart (first degree heart block)
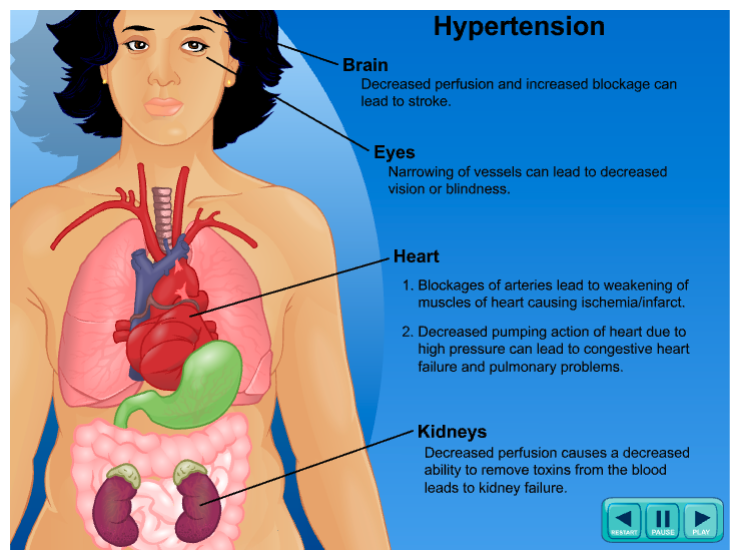
Brain
- Decreased perfusion and increased blockage can lead to stroke
Eyes
- Narrowing of vessels can lead to decreased vision or blindness
Heart
- Blockages of arteries lead to weakening of muscles of heart causing ischemia/ infarct
- Decreased pumping action of heart due to high pressure can lead to congestive heart failure and pulmonary problems
Kidneys
- Decreased perfusion causes a decreased ability to remove toxins from the blood leads to kidney failure
GASTROINTESTINAL SYSTEM
- Assess for nausea, vomiting, diarrhea, gastric reflux and GI bleeding
- All above conditions can cause electrolyte imbalances, anemia, hypovolemia
- These patients may be at risk for hypoxemia due to anemia and hypotension due to hypovolemia
ENDOCRINE SYSTEM
Endocrine Disorders may occur due to an overproduction or decrease in hormones or by alterations in the stress response
- Common Endocrine disorders:
- Diabetes
- Thyroid Disease
- Less Common Endocrine disorders:
- Pheochromocytoma
- Addison’s Disease
- Cushing’s Disease
- Conn’s syndrome
- Hypoaldosteroidism
- DIABETES:
- Chronic disease characterized by a disruption of glucose metabolism and resulting in high plasma glucose levels
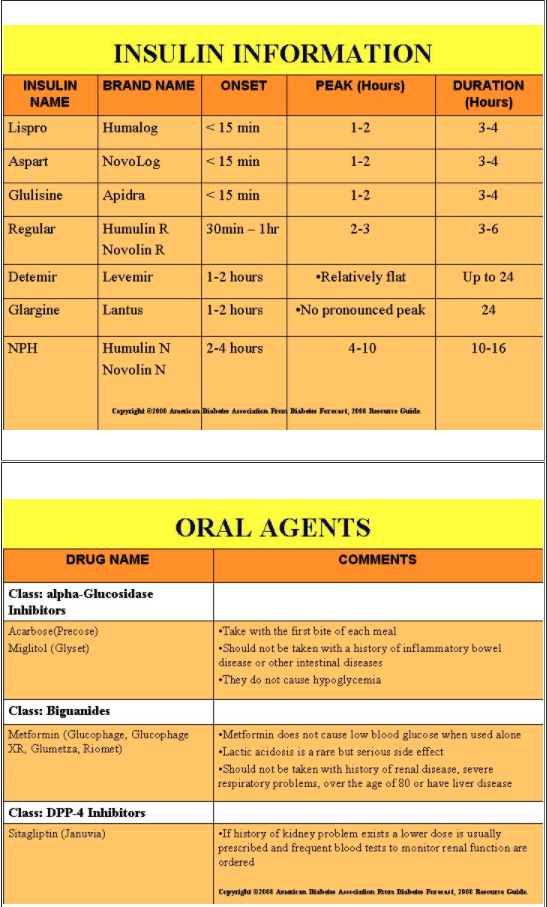
- TYPE 1 insulin – dependent diabetes (IDDM) :
- Insulin deficiency
- Childhood onset
- Predisposition to hyperglycemia, acidosis and ketosis
- TYPE 2 Non-insulin – dependent diabetes (NIDDM) :
- Insulin resistance
- Adult onset, also associated with obesity, pregnancy, disease
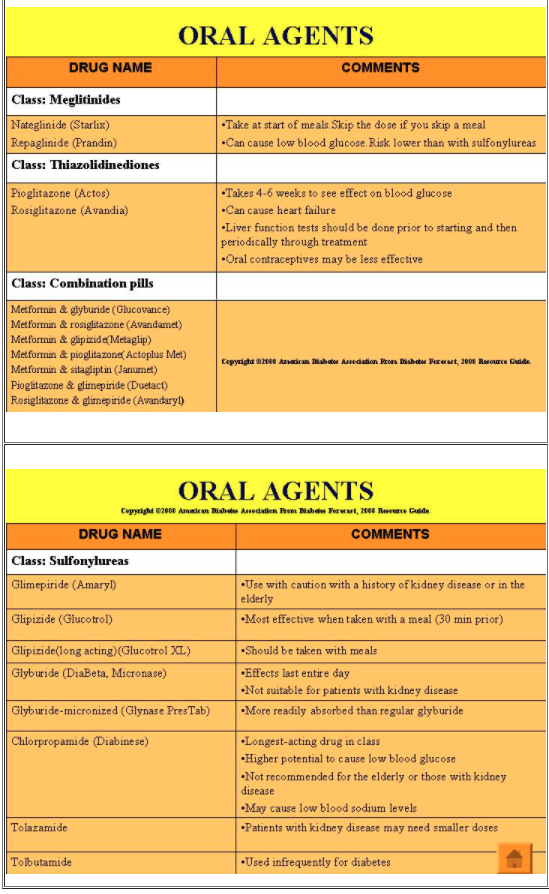
- Can be controlled through diet, exercise and weight control
- May need oral hypoglycemics (insulin release or peripheral response to insulin) and / or insulin
End -organ system impairment associated with diabetes:
- Cardiovascular : increase incidence of hypertension, coronary artery disease and silent myocardial infarction due to neuropathy
- Renal : increase incidence of nephropathy
- GI: slow emptying of the stomach due to autonomic neuropathy increases risk of aspiration and regurgitation
- Peripheral Vascular Disease: requires extra caution for positioning of patient during procedure
- Eyes : retinopathy
Diabetes -Important points:
- Need to have a clear understanding of Type 1 and Type 2 Diabetes and their treatments
- Associated with high incidences of comorbidities
- Pre-procedure assessment of diabetic treatment includes: blood sugar, name/type of medication(s) , time of last dose, patient sign and symptom profile
- Procedures should be scheduled early in morning to prevent hypoglycemia
- Risk for aspiration due to autonomic neuropathy and may benefit from antiemetic/GI motility agents pre procedure
HYPOGLYCEMIA :
- Defined as a blood glucose level < 4mmol
- Signs and symptoms:
- Are highly variable from one person to the next. Long standing diabetics may not be symptomatic, making glucose monitoring very important
- Skin pale and sweaty
- Headache, irritability, anxiety
- Trembling ,weakness and dizziness
- Difficulty concentrating , drowsiness, confusion
- Palpitations
- Hunger
- Treatment:
- Refer to institutional policies
HYPERGLYCEMIA:
- Defined as a blood glucose level 12mmol/L
- Signs and symptoms:
- Thirst
- Frequent urination
- Fatigue
- Potential causes:
- When food, activity and medications are not balanced
- Stress
- Illness
- Treatment:
- Refer to your unit
Diabetes #
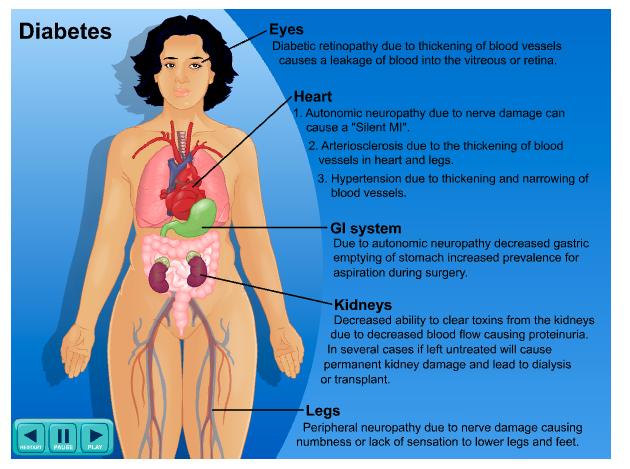
Diabetes
- Insufficient production of insulin
- Signs of hyperglycemia : dry mouth, thirst, frequent urination, decreased vision, fatigue / somnolence, weight loss
- Sign of hypoglycemia: sweating, shaking, nervousness, personality changes, hunger, dizziness, fainting, increased heart rate, confusion, irritability, headache, blurred vision, slurred speech
Organs affected by diabetes
- Eyes: diabetic retinopathy due to thickening of blood vessels causes a leakage of blood into the vitreous or retina
- Heart:
- Autonomic neuropathy due to nerve damage can cause a “silent MI”
- Arteriosclerosis due to the thickening of blood vessels in heart and legs
- Hypertension due to thickening and narrowing of blood vessels
- Kidneys: decreased ability to clear toxins from the kidneys due to decreased blood flow causing proteinuria, in severe cases if left untreated will cause permanent kidney damage and lead to dialysis or transplants
- GI system: due to autonomic neuropathy decreased gastric emptying of stomach increased prevalence for aspiration during surgery
THYROID DISEASE
Can present as hyperthyroid or hypothyroid disease
Hyperthyroid disease – excessive thyroxine resulting in an increased basal metabolic rate with potential for tachycardia and hypertension
Symptoms:
Tachycardia
Nervousness, tremors
Heat intolerance
Warm, moist skin
Nursing Considerations:
Important that patient be euthyroid prior to procedure
Assess patient for thyroid treatment, cardiovascular disease and anxiety level
Risk for airway difficulty due to increased thyroid tissue mass
Pharmacological effects of PSA may be reduced because of increased basal metabolic rate
Hypothyroidism:
Deficiency of thyroid hormone resulting in a lowered basal metabolic rate
Symptoms:
Bradycardia , cardiomegaly, CHF
Intolerance to cold
Dry skin, hair loss, periorbital edema
Fatigue, decreased mentation
Nursing Considerations:
sensitivity to PSA medications/hypnotics
¯ ventilatory response to PaCo2 and PaO2
Potential for large tongue mass
** These factors put the patient at risk for CNS & respiratory depression as well as airway management issues. Therefore, careful titration of PSA is advised
The following are less common endocrine diseases:
Addison’s disease:
Occurs due to a ¯ in the cortisol production
PSA preparation may include steroid supplementation to prevent adrenal insufficiency, based on the degree of stress and the magnitude of the procedure
Conn’s disease:
Excess production of aldosterone , a hormone that assists the body to respond to stress
PSA preparation includes K+ replacement, Antihypertensives, correction of fluid status
Cushing’s disease:
Glucocorticoid overproduction
PSA preparation includes correction of fluid & electrolyte imbalance, treatment of hypertension, regulation of blood sugars
Hypoaldosteronism:
Decreased aldosterone secretion
PSA preparation includes K+ balance, ¯ fluid & Na intake, mineralocortiosteroid administration
Pheochromocytoma:
Catecholamine (esp. norepinephrine)- secreting tumours causing palpitations, hypertension, cardiac dysrhythmias, and hyperglycemia
Surgical tumour resection should be done before non-urgent PSA procedures are considered
RENAL SYSTEM
Assessment of renal system is necessary:
• To determine kidney function, including regulation of fluid balance, acid – base system, excretion of waste
products and electrolyte balance, and detoxification of PSA medications
• The kidneys perform these tasks through filtration, absorption & secretion
• Renal disease, with it’s resulting decreased protein- binding, increases risk for accentuation of PSA
medications effects
• Accentuation of benzodiazepines may be greatly enhanced (Midazolam is 98% protein bound)
Renal Insufficiency:
• Hydration status is important and the goal is to preserve normal renal function throughout the procedure
and postoperatively
• Baseline GFR and creatinine should be obtained
• Pre-procedure assessment should also include: weight, blood pressure, heart rate, skin turgor and last void
• Volume status should be treated appropriately (e.g. hydration and/or diuresis)
Patients on dialysis:
• Usually associated with anemia caused by decreased erythropoietin (required for hemoglobin synthesis),
predisposing to hypoxia
• Avoid use of shunted arm for IV access / B/P monitoring
• PSA preparation focuses on fluid volume balance. BP control, electrolyte balance
• May be necessary to have dialysis day prior or on the the day of procedure, predisposing to hypovolemia
• Asepsis is vital as infection is the leading cause of morbidity
• Careful titration of PSA medications is vital to avoid hypotension and hypoxemia
HEPATIC SYSTEM
Liver:
• The largest organ in the body receiving 29% of cardiac output
• Is responsible for the filtering the blood, producing bile and proteins (esp. related to blood clotting),
metabolizing many drugs, storing may vitamins and minerals , and assisting in the breakdown and recycling
of red blood cells
• Patients with hepatic disease are predisposed to ascites, portal hypertension, decreased hematocrit,
electrolyte imbalances and arterial desaturation
Enzymatic Induction:
• An important pharmacological function of the liver is the breakdown of lipid-soluble medications into water-
soluble compounds
• The degree of pharmacological metabolism is dependent on hepatic blood flow and enzyme activity
• Significant liver damage may cause resistance or sensitivity to PSA medications.Therefore, careful titration
and monitoring of response to the PSA medications are required
Nursing Considerations pre procedure:
• Assess coagulation profile, nutritional & hydration status
Hepatitis
• Refers to syndromes or diseases causing liver inflammation, including inflammation due to viruses and
chronic alcohol abuse. Viruses causing hepatitis include Hepatitis A, B, C, E, and the delta factor
Nursing Considerations:
• Discourage the use of alcohol pre-procedure
• Assess coagulation profile and nutritional status
Cirrhosis
• Scar tissue replaces normal, healthy tissue, blocking the flow of blood through the organ and preventing it
from working as it should
• Slows the normal flow of blood through the portal vein blood from the intestines and spleen to the liver ,
which increases the pressure inside it
• Cirrhosis and portal hypertension may affect the cardio- pulmonary systems causing decreased oxygen
affinity for hemoglobin, resulting in oxygen desaturation and hypoxemia
Nursing Considerations:
• Predisposition to desaturation and hypoxemia requires careful titration and reduction of PSA medications
Cirrhosis of the liver #
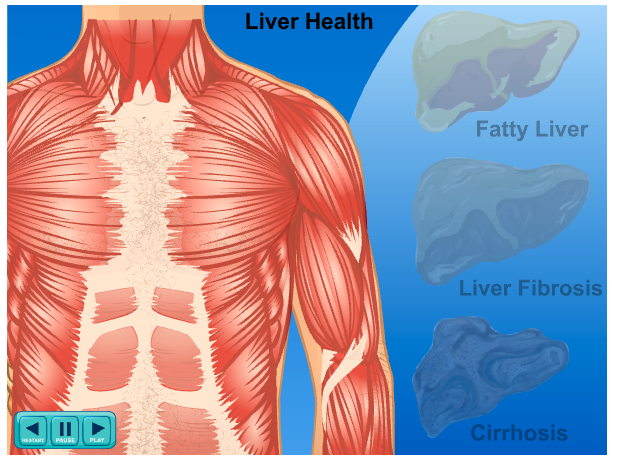
Cirrhosis of liver
- Occurs after years of liver inflammation
- Life threatening condition due to scarring of liver tissue which eventually replaces the normal liver tissue
- Scarred tissue causes a nodular tissue formation which can cause blockages to the bile duct, this causes edema of the tissue then causing a backup of bile into the liver and the blood stream
- Scar tissue also causes a decreased blood flow to the liver, therefore blood vessels delivering blood to the liver can be enlarged and then lead to hypertension in the veins that flow from the intestines. Commonly known as portal hypertension
- Common causes of cirrhosis are alcoholism and hepatitis C
Normal liver functions are
- Remove toxins from the body
- Produces immune agent to control infection and removes germs and bacteria from blood
- Produces proteins that regulate blood clotting and bile to help absorb fat and fat soluble vitamins
- ELDERLY
- Concerns:
- Growing aging population in the world due to advance medical technology
- Organ systems gradually become less efficient
- 3 changes occur in body composition of the elderly: decrease body muscle mass, increase fat storage and decrease body water
- These changes affect women more than men
- **** The full pharmacological effect of PSA medications may be delayed for more than 6-10 min depending on the patient’s cardiac output
Cardiovascular Changes:
- Cardiac output may decrease by 1% every year after the age of 50
- There a loss of tissue elasticity predisposing to hypertension and ventricular hypertrophy
- Decline in beta-receptor responsiveness impacting response to stressors, medications, positioning etc.
- Diminished parasympathetic nervous system tone leading to a reduced ability to adjust cardiac output and BP/HR
Pulmonary Changes:
- Physiologic changes such as a decrease in tissue elasticity and lung space result in :
- Decreased total lung capacity and vital capacity
- Residual volume and dead space
- Decreased PaO2
- Decreased ventilatory response to hypoxia and hypercapnia
Hepatic System changes:
- Liver blood flow at age 65 is decreased to approximately 40% of liver blood flow in patients half that age
- Hepatic enzymes responsible for oxidization of drugs is decreased
- Decreased albumin leads to decreased plasma protein binding, resulting in available free drug
Nursing Considerations:
The decreased conversion of lipid-soluble drugs to water-soluble metabolites leads to:
- Longer duration of action for many PSA medications
- Longer recovery period post sedation
- Chance of adverse effects
- **Must titrate PSA medications in smaller doses and longer intervals to assess effects of drugs
Renal Changes:
- There’s a 6 % decrease in renal function per decade
- Loss of kidney mass, vascular changes, decreased renal blood flow, and decreased GFR
- Ability to concentrate urine, conserve free water and sodium is decreased which predisposes the elderly to dehydration, electrolyte imbalances
- Nursing Considerations:
- Decreased renal blood flow and GFR increases half-life of drugs resulting in prolonged effects of PSA medications
- Recommend using drugs with short half-lives and no active metabolites
- Important to assess fluid and electrolyte status pre-procedure
- ***Must titrate PSA medications in smaller doses and
- longer intervals to assess effects of drugs
CNS Changes:
- Loss of neuronal density, decreased cerebral blood flow and oxygen uptake
- Constriction of carotid arteries susceptibility to cerebral ischemia
- Age-related CNS changes result in incidence of confusion, delirium, sensitivity to drugs
- Nursing Considerations:
- Recommend PSA dosage reduction of 30-50%
- Administration of PSA medications may lead to prolonged recovery time
- ***Must titrate PSA medications in smaller doses and
- longer intervals between doses to assess effects of drugs
- Thermoregulation Changes:
- Geriatric patients may not regulate body temperature efficiently
- Shivering increases O2 consumption as much as 100-200%, myocardial strain with the potential for tissue hypoxia
- Nursing Considerations:
- Keep patient warm
- Hypothermia ¯’s clearance of medication resulting in a pronounced and prolonged pharmacological effect
PATIENT ASSESSMENT UNIT REFERENCE LIST
American Diabetes Association. Diabetes Forecast, 2008 Resource Guide. Reprinted with permission from The American Diabetes Association.
American Heart Association website: www.americanheart.org .2008-Cardiac Medications At- a- Glance chart. Reprinted with permission
Gilbertson, L., (1999). Conscious sedation, Lippincott Williams & Wilkins, Philadelphia
Kost, M., (1998). Manual of conscious sedation, W.B. Saunders CO
Saunders Elsevier, St. Louis, MO
Kost, M., (2004). Moderate Sedation: Core Competencies for Practice, 2nd edition, W.B. Saunders CO Saunders Elsevier, St. Louis, MO. Permission obtained for 14 pages only including 2 Figures and 5 Tables
Skelly, M., Palmer, D., (2003). Conscious sedation: A handbook for nurse practitioners, WHURR publishing for Professionals, London & Philadelphia
Steen, PA., Tinker, JH., Tarhan, S., (1978). JAMA. 239:2566
Tarhan, S., Moffit, EA., Taylor, WF., Guilani, ER.,(1972). Myocardial infarction after general anesthetic. JAMA. 220:2566
Wiener – Kronish, J.P., (2001). Conscious sedation. Hanley & Belfus