Ultrasound Guided Blockade Of The Ilioinguinal And Iliohypogastrics Nerves #
Description #
This unit will review participants knowledge of the anatomy and sensory distribution of the Ilioinguinal and Iliohypogastric nerves. Participants will be able to demonstrate the correct ultrasound image view and safe needle insertion.
Learning Objectives #
On Completion of this unit participants will be able demonstrate their knowledge of the anatomy and nerve distribution of the inguinal region by identifying the relevant structures via ultrasound scanning. they will understand how to safely apply an appropriate amount of local anesthetic to the visualized nerves.
Performing an Ultrasound Guided Ilioinguinal/Iliohypogastric nerve block #
The ilioinguinal and iliohypogastric nerve block is commonly performed in children. Regional techniques improve post operative analgesia, reduce the stress response to surgery and reduce the perioperative opioid requirements. The advent of high resolution, portable ultrasound imaging has enabled visualization of nerves and surrounding structures. Ultrasound guidance has been shown to reduce block onset time, prolong duration of nerve block with reduced volumes of local anesthetic and hence improve success rates and safety profiles.
Unit Goals #
- Review gross anatomy of lower abdominal wall
- Identify lower abdominal wall anatomy with ultrasound guidance.
- Define the theoretical approach to performing an ultrasound guided Ilioinguinal/Iliohypogastric nerve block.
Indications and Contraindications #
Indications #
Post operative pain control for the following operations:-
- Inguinal hernia repair
- Orchidopexy
- Hydrocoele repair
- Removal of spermatic cord cyst
Pain from peritoneal traction, manipulation of the spermatic cord and testes is not adequately covered intraoperatively due to sensory input from the genitofemoral nerve.
Contraindications #
Absolute: #
- Local infection
- Patient/Parental refusal
- Mechanical nerve lesions at location of block
- Local anesthetic allergy
Relative: #
- Coagulopathies
- Thrombocytopenia
- Certain neurological conditions
- Previous inguinal surgery or anomolous inguinal anatomy
Anatomical Considerations #
Description of nerve pathway 1 #
The 1st Lumbar primary ventral ramus receives a branch from the 12th thoracic nerve which then pierces the Psoas Major muscle. The Ilioinguinal and Iliohypogastric nerves appear as two distinct nerves on the lateral border of the Psoas muscle, the products of the ramus bifurcation. They initially pass across the anterior surface of the Quadratus Lumborum muscle before piercing the lumbar fascia to take up positions between the muscles of Internal Oblique and Transversus Abdominis and Transversus Abdominis and peritoneum (Ref: Van Schoor et al.)
Picture 1: Anatomical pathway of the ilioinguinal and iliohypogastric nerves. The psoas muscle has been removed to demonstrate the nerve roots as they pass infront of Quadratus Lumborum.
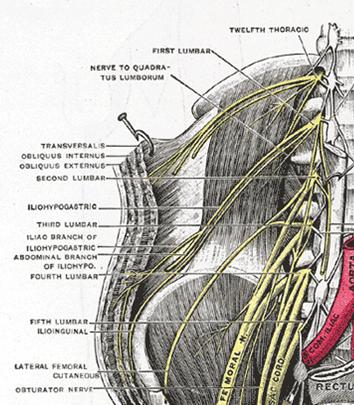
Reprinted from Gray’s Anatomy, 20th Edition, Editor: Warren H Lewis, “The Lumbar Plexus And It’s Branches”, Figure 823, Copyright 1918, with permission from Elsevier and Published May 2000 by Bartleby.com; © 2000 Copyright Bartleby.com, Inc.
Path of the Iliohypogastric nerve #
The Iliohypogastric nerve runs superiorly and more superficially relative to the Iioinguinal nerve. It progresses anteriorly between the muscles Internal Oblique and Transversus Abdominis. At the Iliac Crest, the Iliohypogastric nerve splits into two branches, the lateral cutaneous branch which supplies the skin over the ventral part of the buttocks, and the medial cutaneous branch which continues medially piercing the Internal Oblique muscle and External Oblique aponeurosis. Here it supplies the skin covering the abdominal wall in the suprapubic region.
Path of the Ilioinguinal nerve #
The Ilioinguinal nerve only pierces the Transversus Abdominis muscle at the level of the Iliac Crest to run anteriorly under Internal Obllique. It gradually pierces Internal Oblique and the External Oblique Aponeurosis to join the lower border of the spermatic cord in males or the round ligament of the uterus in females. Its sensory distribution covers the skin of the upper medial aspect of the thigh and either the skin of the upper part of the scrotum and the root of the penis in males or the labium majus and mons pubis in females.
Picture 2: Pathway of the Ilioinguinal and Iliohypogastric nerves.
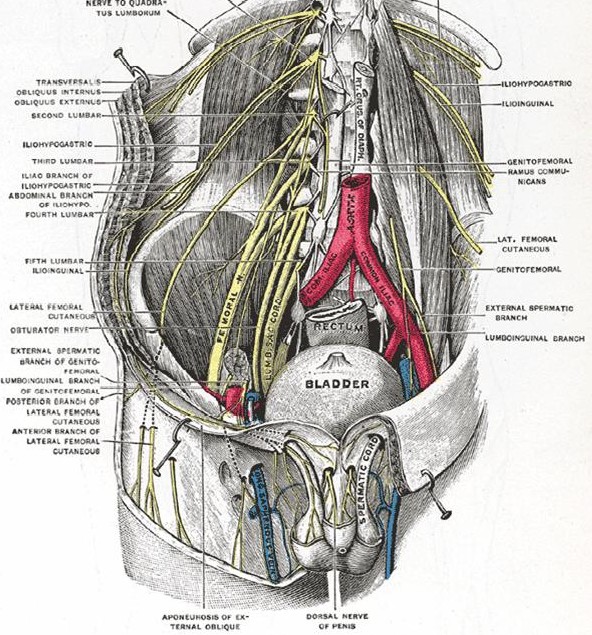
Reprinted from Gray’s Anatomy, 20th Edition, Editor: Warren H Lewis, “Deep and Superficial Dissection of the Lumbar Plexus”, Figure 824, Copyright 1918, with permission from Elsevier and Published May 2000 by Bartleby.com; © 2000 Copyright Bartleby.com, Inc.
Anatomical Variation in Children #
There is a large amount of variability in the positioning of the Ilioinguinal and Iliohypogastric nerves with respect to the anterior superior iliac spine and the depth at which these nerves are found. This variability is born out by several different recommended points of entry when conducting this block using a blind technique and the variability of reported failure rates 10-30%(Lim et al.)
Nerve Position #
From cadaveric work in neonates and infants, Van Schoor et al.showed that the Ilioinguinal nerve lies on average approximately 2.0 mm away from the anterior superior iliac spine whilst the iliohypogastric nerve lies on average approximately 3.6 mm away. Ultrasonographic work by Willschke et al. showed the Ilioinguinal nerve to lie on average 6.7 mm away from the anterior superior iliac spine and 8mm away from the skin in children between 1 month and 8 years. They also demonstrated that the ilioinguinal nerve on, for this age group was only 3.3 mm away from the peritoneum. These descriptions put the nerves closer to the anterior superior iliac spine than previously thought.
Nerve Depth #
Willschke et al have shown there is no correlation between thickness of subcutaneous tissue and weight. Adult work has shown that both nerves can be found with 90% reliability between the internal oblique and transversus abdominis muscles 5 cm cranial to the anterior superior iliac spine (Eichenberger et al.). This point delineated in adults is obviously a variable point in children, however it does direct the insertion point of the needle to a place superior and medial to the anterior superior iliac spine.
Muscle Plain Variation #
The muscle layers have been described so far as clear separate entities. However the outer most muscle, external oblique, becomes an aponeurosis covering the internal oblique muscle as it progresses medially. In the study by Willschke et al they noted that 50% of subjects only had an external oblique aponeurosis rather than an identifiable muscle belly on ultrasound imaging. This has important implications when trying to illicit 2 fascial clicks using the blind technique.
Before starting an Ilioinguinal/Iliohypogastric nerve block It is important that all the following have been done before performing the nerve block.
Preoperative Visit #
Confirm no contraindications
Explain procedure
Explain risks and benefits, pointing out common or severe risks
Clearly explain any anticipated weakness or altered sensation post-operatively and give an explanation of how long these effects may last
Give clear guidance of other analgesia required and when this should be taken post-operatively.
Prior to commencing block #
Inform OR staff of regional block and have equipment laid out ready
Resuscitation facilities available, tilting bed and working suction
Confirm correct side with patient or that site has been marked
Secure IV access
Required Equipment #
The ideal probe for this block in children is the hockeystick. It gives good resolution of structures close to the skin, operating at a maximum frequency of 15MHz. It has a small footprint allowing easier access to the area with the needle.
The block is conducted under sterile conditions. The probe is placed in a sterile sheath with aqueous gel between probe and sheath. This ensures the probe does not come into contact with blood and keeps the site sterile. Further sterile gel is required between sheath and skin to provide optimal image quality.
At the end of the case, the probe should be wiped with a dry cloth/towel to remove aqueous gel. Alcohol wipes or gel should not be used as they corrode the probe.
Hockeystick probe

Ultrasound Image Recognition Of The Ilioinguinal Region #
Structure Identification process #
Identify an imaginary line between the anterior superior iliac spine and the umbilicus.
Apply the hockey stick probe to the skin with the long axis of the probe running parallel along this line and the heel of the probe over the anterior superior iliac spine (ASIS).
Muscle Plane Identification #
The probe is then adjusted to achieve the optimum picture of the muscle planes. This occurs when the ultrasound beam cuts the muscle plane at 90 degrees. Adjustment of near/far and overall focus should be carried out at this stage. The muscle planes should be easily identifiable, remembering that the external oblique muscle may not be present in up to 50% of patients.

Nerve Identification #
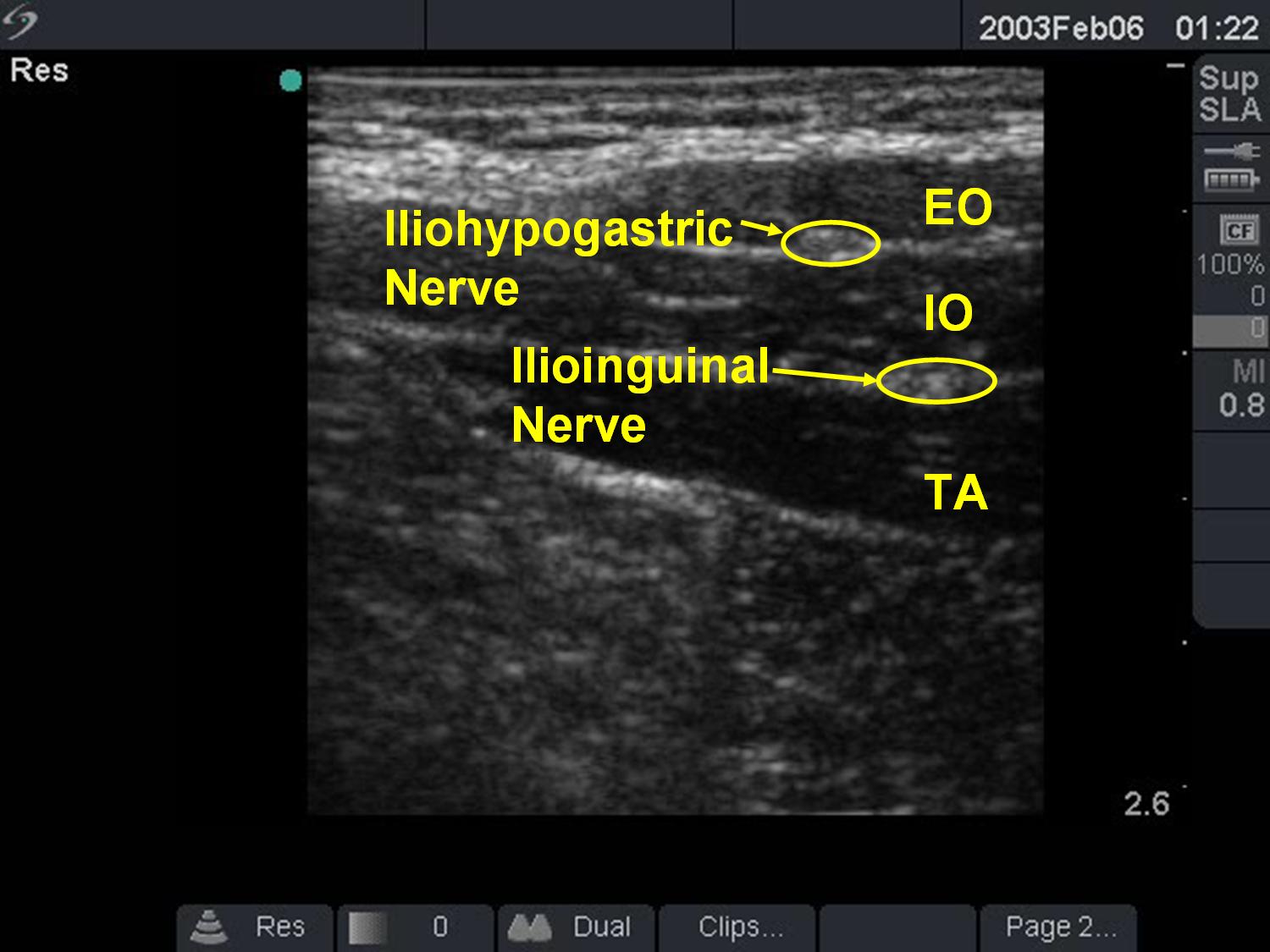
Having identified the plane between the internal oblique and transversus abdominis muscles, the hockeystick probe should be rotated around the ASIS moving 20 degrees superiorly and inferiorly of the line joining the ASIS and the umbilicus looking for the ilioinguinal and iliohypogastric nerves. They are identified as hyperechoic (white) signals sat between the muscle layers.
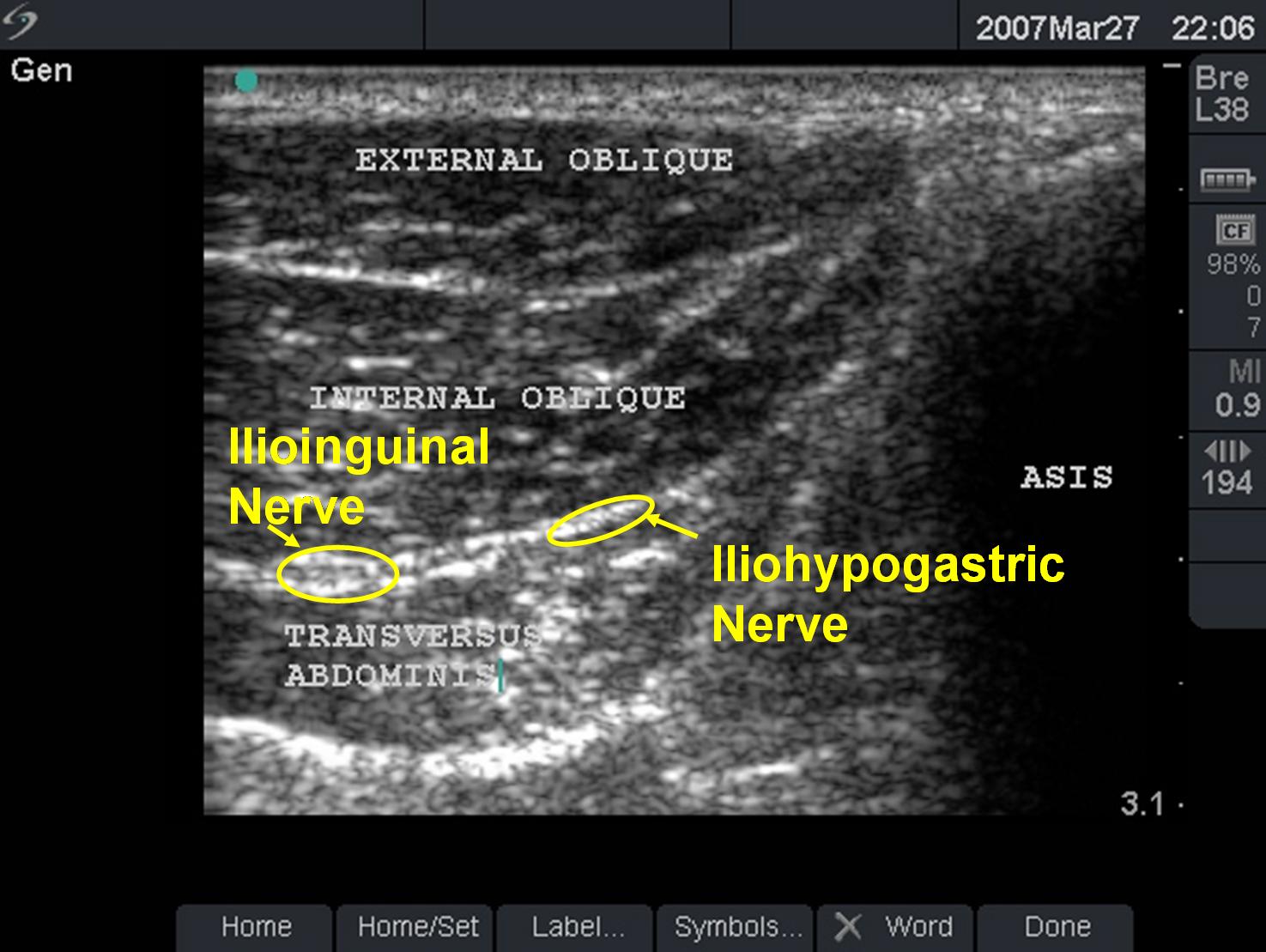
Depending on where the nerves pierce the muscle layers, the two nerves may be seen in the more classical positions running in two separate muscle planes as shown below.
Needle Insertion #
The needle can be inserted in one of two ways, either from the medial end of the hockey stick probe with the needle tip angled back towards the anterior superior iliac spine or via a short axis approach with the needle introduced almost vertically down onto the muscle plane. The needle is inserted and the tip visualized throughout the whole procedure. IT IS IMPORTANT THE NEEDLE IS NEVER ADVANCED WITHOUT NEEDLE TIP VISUALIZATION. The short axis vertical approach does not allow the visualization of the needle tip at all times, so is not an appropriate technique near sensitive structures.
Target #
If the nerves are clearly identified, then the needle tip is directed to lie immediately adjacent to the nerve and a small amount of local anesthetic injected. If in the correct position, the local anesthetic will flow around the nerve surrounding it with a hypoechoic (black) ring or hollow. If this is not the case, ensure you have the needle tip visualized and reposition the needle and try again.
If the individual nerves are unable to be visulaized, then the local anesthetic should be placed between the internal oblique and transversus abdominis muscles. This potential space will open up as you inject the local anesthetic and the nerves should be visualized.
Complications #
General: #
- Infection
- Hematoma
- Local anesthetic toxicity/allergy
- Intrarterial injection
- Nerve injury
- Damage to surrounding structures if needle tip is not correctly visualized
Local: #
- Bowel perforation/hematoma
- Inadvertant blockade of femoral nerve, lateral cutaneous nerve of thigh.
Please click to complete a brief evaluation questionnaire. Thank you!
-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=
Additional Resources:
Ultrasonography for ilioinguinal/iliohypogastric nerve blocks in children
British Journal of Anaesthesia 95 (2): 226–30 (2005) doi:10.1093/bja/aei157 Advance Access publication May 27, 2005
Leg weakness is a complication of ilio-inguinal nerve block in children
British Journal of Anaesthesia 92 (2): 273±4 (2004) DOI: 10.1093/bja/aeh045
Ilioinguinal and iliohypogastric nerve block revisited: single shot versus double shot technique for hernia repair in children
Pediatric Anesthesia 2005 15: 371–377 DOI: 10.1046/j.1460-9592.2002.00832.x