Functional Reach Test (FRT) #
#
Description #
This unit will describe the correct administration, scoring and interpretation of the Functional Reach Test (FRT) performed for TJA patients.
Learning Objectives #
By the end of this unit, the learner will be able to perform the following tasks for TJA patients:
– Administer the Functional Reach Test (FRT)
– Score the Functional Reach Test (FRT)
– Interpret the Functional Reach Test (FRT)
What is this test? #
What is the Functional Reach Test? #
The Functional Reach Test (FRT) is a valid and reliable measure that is useful for assessing THA and TKA patients and falls within the WHO’s ICF domain of Activity (Figure 1). The FRT measures static balance through maximal forward reach from a fixed base of support. In addition, it can be completed relatively quickly requiring approximately 5 minutes to administer and score.
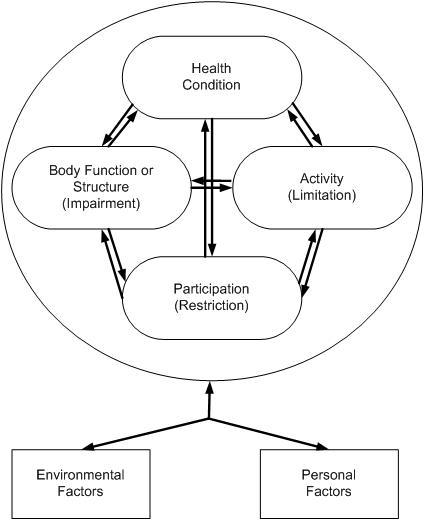
Figure 1. The International Classification of Functioning, Disability and Health (ICF) Conceptual Model. Taken from Riddle, D. & Stradford, P. (2013). Is this Change Real? Interpreting Patient Outcomes in Physical Therapy. Figure 2-1.
When do I use it? #
When do I use the Functional Reach Test? #
The Functional Reach Test (FRT) can be used in a number of phases along the TJA Continuum of Care. Specifically, as seen in Figure 2, the FRT is recommended for use in the Pre-Operative, Post-Acute, and Active Living phases. Health professionals can therefore use this outcome measure to monitor change in the patient’s status as he or she moves through these phases of care (*note that it is not recommended in the Acute Phase).
Figure 2. The phases along the TJA Continuum of Care for which the FRT is recommended.

Equipment needed #
What equipment is used to perform the Functional Reach Test? #
To perform the Functional Reach Test (FRT) with a patient, only one piece of equipment is required:
. A tape measure or pre-measured intervals (in centimetres) marked on the wall at shoulder height.
How do I do it? #
How do I administer the Functional Reach Test? #
To learn how to administer the Functional Reach Test (FRT), please review the instructional video below.
- A written version of the instructions can be found at the following link → Functional Reach Test Instructions
- Do you want all the module information on a single piece of paper? If so, click this link! → FRT One Pager
How do I score it? #
How do I score the Functional Reach Test? #
Scoring the Functional Reach Test (FRT) is easy to do:
- Measure the difference between the start and end positions
- The patient should complete two trials
- The final score is taken by averaging the score of the two trials
What does it mean? #
How do I interpret the Functional Reach Test? #
It is simple to interpret the Functional Reach Test (FRT): the greater the distance a patient can reach, the better their balance and the less their risk of falling. For example a FRT of:
- < 17.5 cm in community dwelling older adults suggests limited mobility skills, an inability to leave the neighborhood without help, and restrictions in ADLs
- < 18.5 cm in frail elderly patients indicates a falls risk
- Is your patient better than the median? In the Canadian Study of Health and Ageing, the median FRT value among 2305 elderly individuals without cognitive impairment is 29cm (interquartile range 23 to 34 cm).
Example #
Example #
A family GP has referred a frail 84 year old female to you as they suspect she is at risk for falls. You have the patient perform a Functional Reach Test (FRT) on which she scores 16.0 cm. Is this patient at risk for falls?
< 18.5 cm in frail elderly patients indicates a falls risk
16.0 cm < 18.5 cm
Yes, according to the FRT, this patient is at risk for falls.
References #
- Westby MD, Brittain A, Backman CL. Expert consensus on best practices for post-acute rehabilitation after total hip and knee arthroplasty: A Canada-US Delphi study. Arthritis Care Res. 2014;66(3):411-23.
- Rehab Measures: Functional Reach Test / Modified Functional Reach Test (2013). Available at www.rehabmeasures.org/Lists/RehabMeasures/PrintView.aspx?ID=950
- Weiner DK, Duncan PW, et al. Functional reach: a marker of physical frailty. J Am Geriatr Soc. 1992; 40(3):203-7.
- Duncan PW, Weiner DK, et al. Functional reach: new clinical measure of balance. J Gerontol. 1990;45(6):M192-7.
- Lau MCK, Lam JKS, et al. Physiotherapist-designed aquatic exercise programme for community dwelling elders with osteoarthritis of the knee: a Hong Kong pilot study. Hong Kong Med J 2014;20(1):16-23.
- Thomas JI, Lane JV. A pilot study to explore the predictive validity of 4 measures of falls risk in frail elderly patients. Arch Phys Med Rehabil 2005;86(8):1636-40.
- Rockwood K, Await E, Carver D, & MacKnight C. Feasibility and measurement properties of the Functional Reach and the Timed Up and Go Tests in the Canadian Study of Health and Aging. J Gerontol 2000;55A(2):M70-73.
- WHO International Classification of Functioning, Disability, and Health – http://www.who.int/classifications/icf/icf_more/en/
- Riddle, D. & Stradford, P. (2013). Is this Change Real? Interpreting Patient Outcomes in Physical Therapy. F.A. Davis Company: Philadelphia.