Description #
This unit is designed to help health care professionals develop a better understanding of the diagnosis of Chronic Obstructive Pulmonary Disease (COPD).
Learning Objectives #
By the end of this unit, you should be able to:
1. Explain the importance of early diagnosis of COPD
2. Define spirometry and explain its relevance in the diagnosis of COPD
3. Explain the classification of COPD severity
4. Explain how to differentiate COPD from asthma and other causes of chronic breathlessness
Diagnosis #
Despite the prevalence of COPD, it remains an underdiagnosed disease. As well it is often diagnosed late in the disease progression. Symptoms may not become apparent until late in the disease process, but the changes to the lung begin many years earlier. Often by the time a diagnosis is made, 50% or more of the lung function has been lost. This has implications for effective disease management, symptom control, quality of life, and long-term survival.
There are many reasons that COPD is underdiagnosed and diagnosed in the later stages.
- COPD is a slowly progressive disease. Signs and symptoms in the early stages of disease may be absent or overlooked.
- Individuals often learn to adjust to their symptoms and exercise limitations.
- Symptoms are non-specific. Shortness of breath on exertion is a common symptom and misdiagnosis is common.
- Symptoms may be attributed to the normal aging process, lack of fitness, or as a consequence of smoking.
- Medical care may be avoided in smokers out of guilt or denial or fear that they will have to quit smoking or be unable to quit.
- There is a lack of awareness of COPD.
Investigations #
(put prev page) Establishing an early diagnosis in COPD patients is important in providing prompt disease management, both pharmacological and non-pharmacological. Early diagnosis and early initiation of management leads to improved health status, exercise capacity, and survival. In order to reach a diagnosis of COPD, the following investigations are generally used:Patient historyPhysical examination Spirometry, and confirming the presence of airflow obstruction with spirometry. – Targetted clinical history. Such a diagnosis should be considered in any patient who has symptoms of cough, sputum production, or dyspnea (difficult or labored breathing), and/or a history of exposure to risk factors for the disease. A clinical diagnosis of COPD should be considered in any patient who has dyspnoea, chronic cough or sputum production, and/or a history of exposure to risk factors for the disease – Physical examination of patients, although important, is not usually diagnostic and can underestimate the presence of significant air flow limitation. Clinical symptoms and signs, such as abnormal shortness of breath and increased forced expiratory time, can be used to help with the diagnosis. Exclude other causes:
Examination and investigations (e.g. chest x-ray, ECG, FBC) to help rule out alternative diagnoses. These include pulmonary function tests, chest x-ray, arterial blood gases, complete blood cell count, and alpha1-antitrpysin deficiency screening (in Caucasian patients under the age of 45 with a strong family history of COPD). – An important part of the diagnostic process for COPD is excluding other causes of symptoms. Table X list some common conditions that present with similar symptoms of COPD Table 1. Differential diagnosis of chronic breathlessness Asthma Bronchiectasis Cardiovascular conditions (eg. Congestive Heart Failure) Tuberculosis Pulmonary vascular disease Severe de-conditioning Obesity Anemia Interstitial lung disease Obliterative Bronchiolitis Diffuse Panbronchiolitis Neuromuscular disease
Table. 1 – Confirmation of the presence of airflow obstruction with a spirometer. The post-bronchodilator FEV1 is used to classify the degree of airflow obstruction. Spirometry is the only accurate means of measuring and quantifying airflow obstruction in COPD and is essential for making a confident diagnosis. Spirometers are now widely available in primary care, but the tests must be performed and interpreted by someone appropriately and adequately trained for the task. Where spirometry is unavailable, the diagnosis of COPD should be made using all available tools. The diagnosis should be confirmed by spirometry. A post-bronchodilator FEV1/FVC ratio <0.70 confirms the presence of airflow limitation that is not fully reversible. Both the diagnosis of COPD and the classification of the severity of the airflow obstruction should be based on the post-bronchodilator FEV1. – Examination and investigations (e.g. chest x-ray, ECG, FBC) to help rule out alternative diagnoses. These include pulmonary function tests, chest x-ray, arterial blood gases, complete blood cell count, and alpha1-antitrpysin deficiency screening (in Caucasian patients under the age of 45 with a strong family history of COPD). – An important part of the diagnostic process for COPD is excluding other causes of symptoms. Table X list some common conditions that present with similar symptoms of COPD Table 1. Differential diagnosis of chronic breathlessness Asthma Bronchiectasis Cardiovascular conditions (eg. Congestive Heart Failure) Tuberculosis Pulmonary vascular disease Severe de-conditioning Obesity Anemia Interstitial lung disease Obliterative Bronchiolitis Diffuse Panbronchiolitis Neuromuscular disease
Spirometry #
Evidence of airway inflammation is present even in early disease where spirometric abnormalities are minor.
What is Spirometry?
Spirometry is a simple breathing test used in the early detection and diagnosis of lung diseases such as COPD and asthma. It is also used to assess disease progression, assess severity of lung function impairment, and evaluate response to therapy. Spirometry is performed with the use of a spirometer, an instrument which measures volumes and flows of air into and out of the lungs.
What is spirometry? #
Spirometry is an important tool in diagnosing COPD. Spirometry is a breathing test that shows how well a patient’s lungs are working. The test measures the amount of air a patient can breathe out and the amount of time it takes to do so. When administered by a trained medical professional, spirometry may help to:
- Confirm a diagnosis of COPD
- Show the severity of a patient’s COPD
- Help decide what medicines and health instructions are appropriate for each patient
- Show how well the prescribed treatment and disease management activities are working
- Targeted Testing:
COPD should be suspected in any patient over 40 years of age who has been exposed to a risk factor (usually smoking) and who presents with any of these symptoms. In these patients, spirometry testing should be ordered in order to assess for the presence of airway obstruction.
In order to establish an early diagnosis of COPD, The Canadian Lung Association recommends that physicians screen their patients for COPD using spirometry if they meet the following criteria:
Smokers or ex-smokers* who are older than 40 years of age, and answer yes to any one of the following questions:
1. Do you cough regularly?
2. Do you cough up phlegm regularly.
3. Do even simple chores make you short of breath?
4. Do you wheeze when you exert yourself or at night?
5. Do you get frequent cold that persist much longer than those of other people you know?
*Some patients with COPD may not have used tobacco. Other risk factors include: occupational exposures, alpha-1 antitrypsin deficiency, early childhood lung infections, and exposure to air pollutants, particularly where wood is burned indoors. Patients with these risk factors should be considered for spirometry testing is they have the respiratory symptoms described above.
Spirometry Measurements:
Forced vital capacity (FVC): The total volume (in litres) of air exhaled using maximal effort after a full inspiration. The normal is higher than 80% of the predicted value. Patients with obstructive lung disease usually have a normal or only slightly decreased vital capacity.
Forced expiratory volume in 1 second (FEV1): The volume (in litres) of air exhaled during the first second of a maximal expiratory effort. A normal value for FEV1 is greater than 80% of the predicted value. Patients with COPD may have a reduced FEV1.
FEV1/FVC ratio: The percentage of the vital capacity which is expired in the first second of maximal expiration. Normally, the FEV1/FVC is about 0.7-0.8. It decreases with age and in patients with obstructive lung disease.
Spirometry should be performed after the administration of an adequate dose of a short-acting inhaled bronchodilator (e.g. salbutamol). A post-bronchodilator FEV1/FVC less than 0.70 confirms the presence of airflow limitation that is not fully reversible and is required for a diagnosis of COPD. Where possible, values should be compared to age-related normal values to avoid false positive diagnosis of COPD in the elderly.
Spirometry is required to make the diagnosis; the presence of a post-bronchodilator FEV1/FVC < 0.70 confirms the presence of airflow limitation that is not fully reversible and establishes a diagnosis of COPD.
The ratio of FEV1 to FVC (FEV1/FVC) identifies the presence of airflow obstruction. The post-bronchodilator FEV1, expressed as a percentage of the reference value for FEV1 for someone of that age, gender, height and ethnic group, is used to classify the severity of that obstruction.
Although it is a useful guide, the severity of the airflow obstruction does not always reflect the severity of the underlying disease. Spirometry is essential, but is only one part of a full assessment.
A comprehensive assessment of disease severity needs to include:
The FEV1
Smoking status
An assessment of breathlessness – Medical Research Council Dyspnoea Score (MRCDS)
Health status
Presence of depression
Exercise capacity
Body mass index (BMI)
Pulse oximetry
The presence of complications, such as cor pulmonale
COPD severity is multifactorial; mild airflow obstruction can be associated with disabling symptoms in some people, and vice versa. Someone with moderate airflow obstruction, can have chronic respiratory failure and therefore severe disease.
Targeted Testing: #
COPD should be suspected in any patient over 40 years of age who has been exposed to a risk factor (usually smoking) and who presents with any of these symptoms. In these patients, spirometry testing should be ordered in order to assess for the presence of airway obstruction.
In order to establish an early diagnosis of COPD, The Canadian Lung Association recommends that physicians screen their patients for COPD using spirometry if they meet the following criteria:
Smokers or ex-smokers* who are older than 40 years of age, and answer yes to any one of the following questions:
1. Do you cough regularly?
2. Do you cough up phlegm regularly.
3. Do even simple chores make you short of breath?
4. Do you wheeze when you exert yourself or at night?
5. Do you get frequent cold that persist much longer than those of other people you know?
*Some patients with COPD may not have used tobacco. Other risk factors include: occupational exposures, alpha-1 antitrypsin deficiency, early childhood lung infections, and exposure to air pollutants, particularly where wood is burned indoors. Patients with these risk factors should be considered for spirometry testing is they have the respiratory symptoms described above.
Severity #
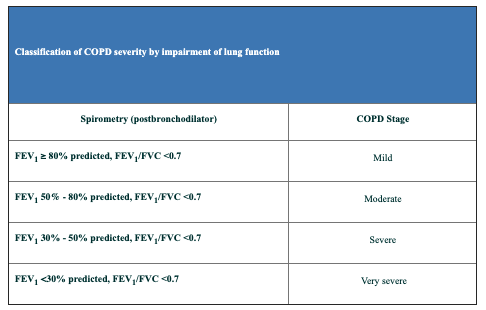
STAGING — The FEV1 (expressed as a percentage of predicted) is often used to stage disease severity [57]. The FEV1/FVC ratio is not used for this purpose because measurement of FVC becomes less reliable as the disease progresses (the long exhalations are difficult for the patients). Different clinical practice guidelines use different cut-off values, but most are similar to the GOLD staging system (table 4) [5].
The GOLD staging system has been criticized for underestimating the importance of the extrapulmonary manifestations of COPD in predicting outcome. The BODE index, which is calculated based on weight (BMI), airway obstruction (FEV1), dyspnea (Medical Research Council dyspnea score), and exercise capacity (six-minute walk distance) (calculator 1), addresses this criticism. This index provides better prognostic information than the FEV1 alone and can be used to assess therapeutic response [58-61].
Spirometry confirms the diagnosis but it is important to remember that there is only a modest relationship between FEV1, dyspnea, functional impairment and health-related quality of life (QOL). Some patients with FEV1 ≤ 35% predicted) may be relatively asymptomatic with a sedentary lifestyle, whereas other patients will be more symptomatic with lesser degrees of airway obstruction because of a more active lifestyle.
COPD is generally classified according to disease severity using FEV1. The FEV1 measurement, while necessary for diagnosis and follow-up, correlates poorly with symptom intensity, exercise capacity and quality of life. There is increased support to use scales such as the Medical Research Council (MRC) scale to assess the type and magnitude of activity that elicit dyspnea and disability. To assess dyspnea (shortness of breath) as objectively as possible, ask your patient to briefly describe how various activities affect her/his breathing. Then document her/his response using this grading system:
In the context that one major purpose of staging systems is to establish prognosis, attention has focused on the value of including weight (i.e., body mass index [BMI]), dyspnea, and exercise capacity (i.e., the 6-minute walk distance), with FEV1 in staging COPD.16 Indeed, the resultant index, called BODE (for BMI, obstruction, dyspnea, and exercise capacity) has been shown to better predict survival in COPD than FEV1 alone. BODE scores of 0 to 10 (most impaired) are stratified into four quartiles, which discriminate mortality risk better than FEV1 alone.
Respiratory symptoms status is not a reliable indicator of the presence of airflow obstruction. Individuals with normal spirometric values may report respiratory symptoms, whereas individuals who have severe to very severe airflow obstruction by spirometry may report no symptoms.
A simple, reproducible measure of the disability caused by breathlessness is the Medical Research Council Dyspnoea Score (MRCDS).
The results are Read coded for inclusion in general practice computer templates and the MRCDS is included in QOF points for patient review.
An MRCDS of 3 or more means that breathlessness is impacting on the patient’s everyday life.
It should prompt you to consider reviewing and possibly stepping up bronchodilator therapy, or referring the patient for pulmonary rehabilitation.
It is important to assess the impact of the disease on a patient’s general health status and quality of life. Many people with COPD lack self-esteem and feel a ‘burden’ to their relatives – it’s useful to ask some prompting questions:
“How fatigued have you been feeling of late?”
“Do you feel in control of your breathlessness?”
“Have you been feeling anxious or depressed recently?”
Formal health status questionnaires, developed as research tools, have been cumbersome to use in primary care, but the COPD Assessment Test (CAT) has been specifically developed for use in this setting (see Resources for a link to the website).
Alternative Diagnoses #
Examination and investigations (e.g. chest x-ray, ECG, FBC) to help rule out alternative diagnoses. These include pulmonary function tests, chest x-ray, arterial blood gases, complete blood cell count, and alpha1-antitrpysin deficiency screening (in Caucasian patients under the age of 45 with a strong family history of COPD). – An important part of the diagnostic process for COPD is excluding other causes of symptoms. Table X list some common conditions that present with similar symptoms of COPD Table 1. Differential diagnosis of chronic breathlessness Asthma Bronchiectasis Cardiovascular conditions (eg. Congestive Heart Failure) Tuberculosis Pulmonary vascular disease Severe de-conditioning Obesity Anemia Interstitial lung disease Obliterative Bronchiolitis Diffuse Panbronchiolitis Neuromuscular disease
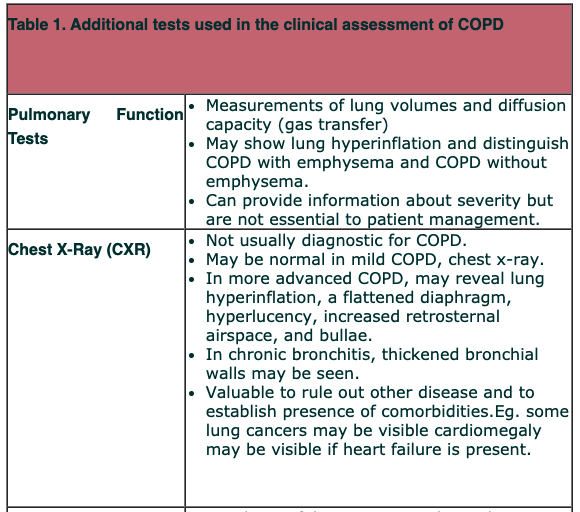
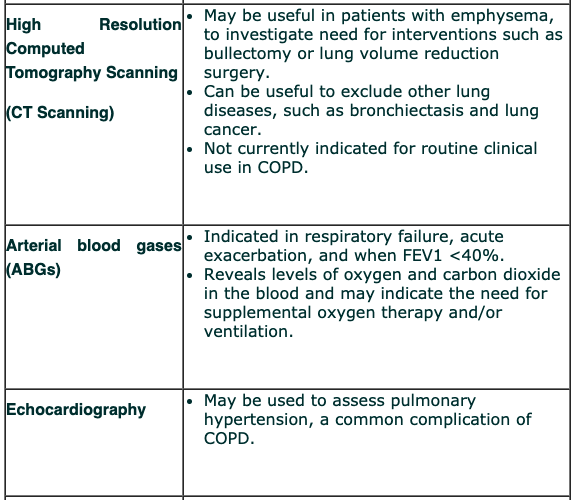
Other Tests #
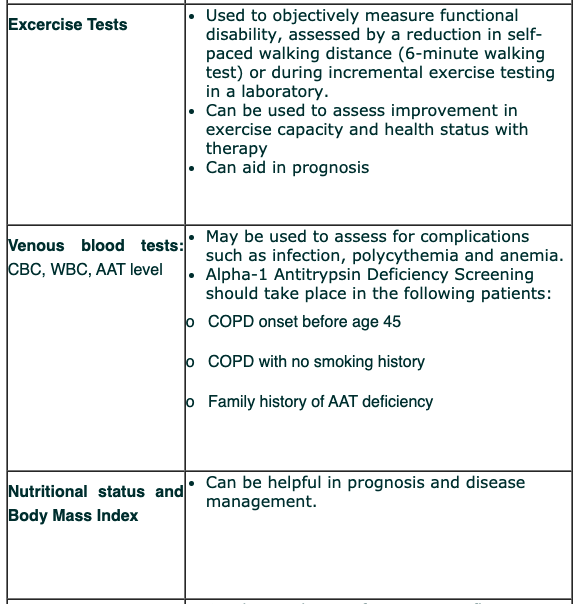
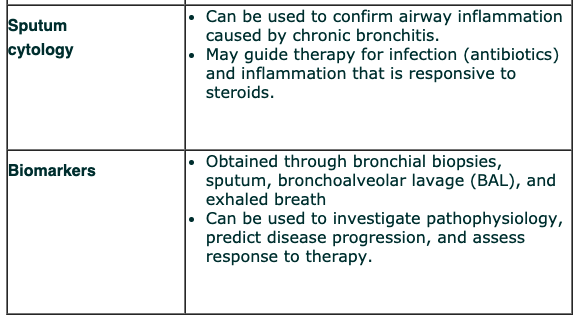
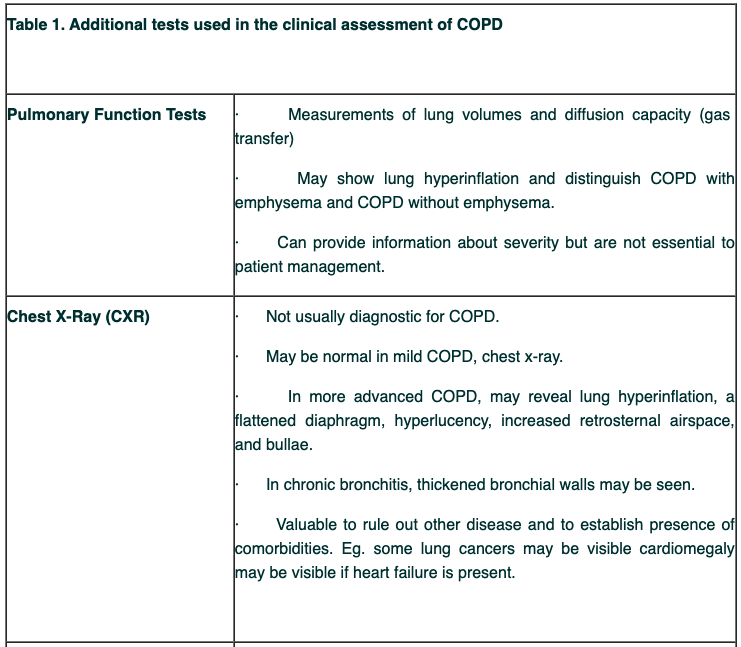
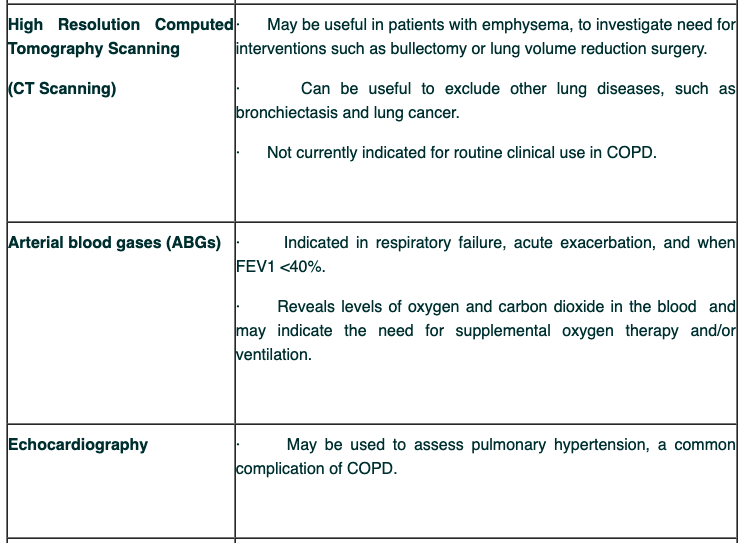
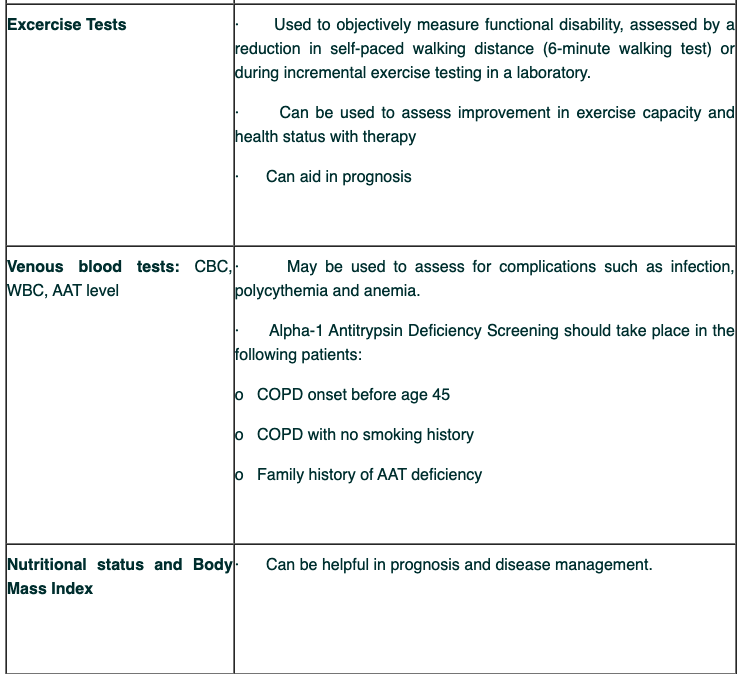
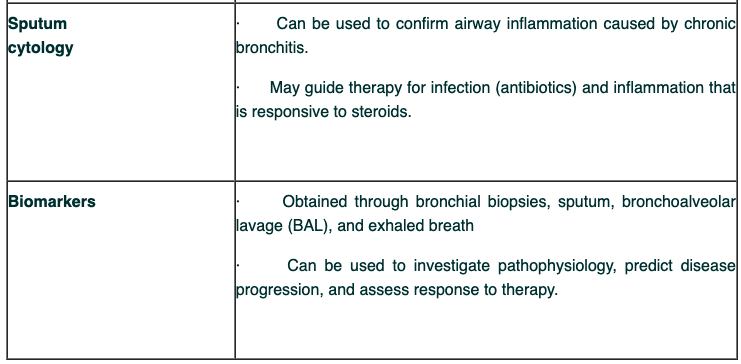
Besides spirometry, a number of additional tests may be performed in the investigation of COPD. Table 1. lists some of the tests that may be patient’s may undergo.
While these tests are NOT diagnostic of COPD, they may be useful to identify comorbidities, assess disease severity, and exclude other lung diseases. A definitive diagnosis of COPD requires spirometry.
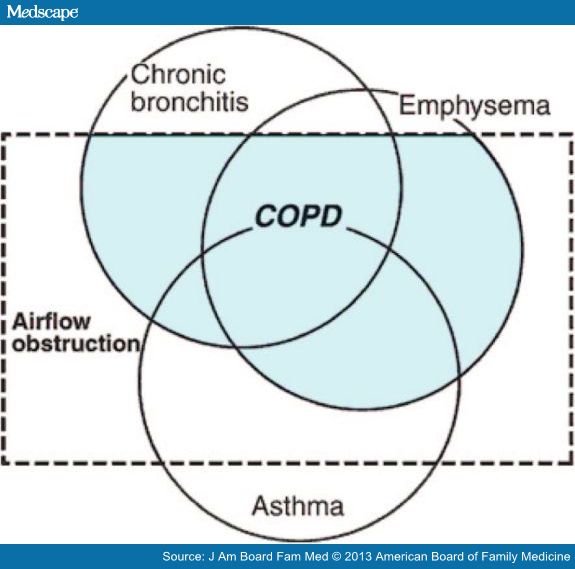
COPD and Asthma #
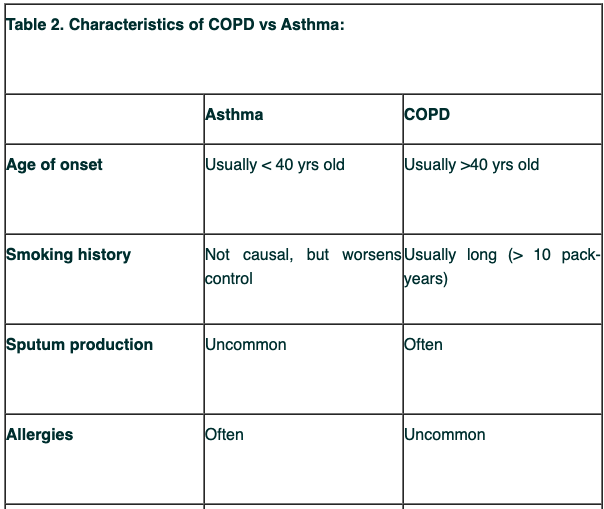
When a diagnosis of COPD is suspected, asthma is an important diagnosis to exclude. Although the two disease are distinct, some of the signs and symptoms are similar and misdiagnosis is common. Separating the two diseases can be difficult, especially when they coexist in the same patient.
Distinguishing asthma from COPD is important as the management of these diseases is different.
While a detailed patent history may be adequate to distinguish COPD from asthma, measurement of airflow obstruction after bronchodilator therapy can help determine the correct diagnosis. In asthma, the airflow obstruction is often fully reversible with bronchodilator therapy, whereas in COPD it is not. Spirometry remains the gold standard test to determine reversibility of airflow obstruction, although additional tests may still be necessary.
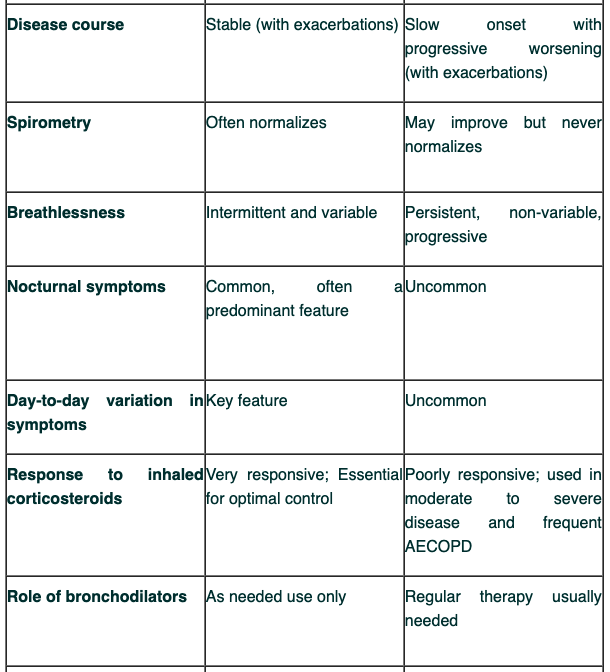
Table 2 shows the most important clinical and management differences which distinguish asthma from COPD.

Overlap Syndrome: #
“Therapeutic Responses in Asthma, COPD, and Overlap Syndrome #
A comprehensive review of the available treatments for obstructive airway diseases is beyond the scope of this article; however, it is important to appreciate that the nature of the underlying inflammation differs between asthma and COPD, as does the response to different classes of medications. Although specific interventions vary by disease, the treatment goals of asthma and COPD are similar and driven primarily by patient-centered outcomes such as controlling symptoms, optimizing health status and quality of life, and preventing exacerbations (ie, reducing their frequency and severity).
In general, therapies for COPD have a much more limited effect compared with those for asthma. While inhaled corticosteroids (ICSs) are the cornerstone of the pharmacologic management of patients with persistent asthma, inhaled bronchodilators (β2-agonists and anticholinergics) are the therapeutic mainstay for patients with COPD. There are no disease-modifying medications currently available that can alter the progression of AO in either asthma or COPD. Smoking cessation, however, is an essential component of the successful management of any obstructive airway disease.
At present there is no randomized clinical trial data to help guide therapeutic interventions in asthma-COPD overlap syndrome. In fact, patients with overlapping asthma and COPD are frequently excluded from treatment trials for either condition, which limits the generalizability of these trials in this neglected patient population. However, practical treatment principles are similar to those for asthma or COPD and involve a comprehensive therapy directed toward airway inflammation, AO, and AHR.” Taken from: Asthma, Chronic Obstructive Pulmonary Disease (COPD), and the Overlap Syndrome Mohammad Obadah Nakawah, MD, Clare Hawkins, MD, Farouk Barbandi, MD J Am Board Fam Med. 2013;26(4):470-477.