Description #
This unit is designed as an introduction to Chronic Obstructive Pulmonary Disease (COPD). It provides and overview of the definition, epidemiology and signs and symptoms of COPD.
Learning Objectives #
By the end of this unit, you should be able to:
1. Define COPD, chronic bronchitis and emphysema
2. Describe the prevalence and mortality
3. Describe the burden of COPD on patients, families and the health care system
4. Identify the common signs and symptoms of COPD
What is COPD? #
Chronic Obstructive Pulmonary Disease (COPD) is a common respiratory disorder which is most often caused by smoking.
COPD is characterized by a limitation of airflow in and out of the lungs. Unlike the airflow limitation seen in asthma, the obstruction is only partially reversible with inhaled medications. Airway obstruction can lead to lung hyperinflation which interferes with normal breathing, causing shortness of breath and increased work of breathing. These symptoms are typically worse during times of higher respiratory demand, such as during exercise.
In the later stages of the disease, even walking short distances can lead to severe shortness of breath. Advanced COPD may also be accompanied by systemic symptoms. Episodes of worsening, called exacerbations, often occur with increasing frequency and severity as the disease progresses.
Although COPD is a progressive disease, it is both preventable and treatable. COPD management strategies focus on establishing an early diagnosis, slowing the progression of the disease, patient education, and maximizing quality of life.
Chronic Bronchitis and Emphysema #
The term COPD includes two disease processes that affect the airways: ‘chronic bronchitis’ and ’emphysema’. Most people with COPD have a combination of both of these conditions, although in some cases, one condition will be dominant.
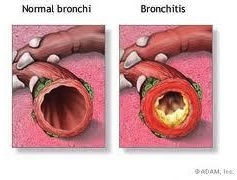
Chronic bronchitis is a condition which involves inflammation and excessive mucous secretion in the airways. It is clinically defined as a cough with sputum production for at least 3 months in a year, for more than 2 consecutive years.
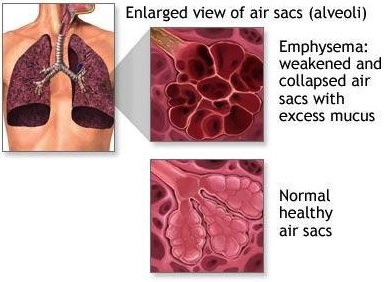
Emphysema is a condition characterized by an abnormal enlargement of the air sacs, or alveoli, in the lungs. Inflammation damages the fibers around the walls of the alveoli, causing them to lose their natural elasticity and eventually to rupture. This destruction of lung tissue can create one large air space instead of many small ones, causing pockets of trapped air and also reducing the surface area available for gas exchange.
Emphysema and chronic bronchitis initially have different symptoms, but as the disease progresses and airflow decreases symptoms are similar for both diseases.
The pathophysiology of COPD is described in greater detail in the next unit, COPD-102: Risk Factors and Pathophysiology.
Prevalence and Mortality #
The prevalence of COPD has been increasing in most of the world. Estimations of COPD prevalence are 10% among adults aged 40 years and older with considerable amount of variation across countries, genders and age groups.
While the disease was once more common in men than women, it is now being reported more in women under age 75. This is partly owing to an increase in smoking prevalence among women over the past 50 years. The proportion of individuals diagnosed with COPD increases with age.
In a 2005 survey of Canadian adults over the age of 34, 4.4% (3.9% of men and 4.8% of women) reported that they had been diagnosed with COPD. However, the prevalence of COPD is thought to be underestimated by at least 50%. Since the early symptoms of the disease are often not recognized, many individuals do not seek treatment. As well, symptoms of shortness of breath may be attributed to the normal aging process by many undiagnosed sufferers. Unfortunately, misdiagnosis and late diagnosis are also common, owing to a lack of public and physician awareness and an under-use of spirometry, the breathing test used to diagnose COPD.
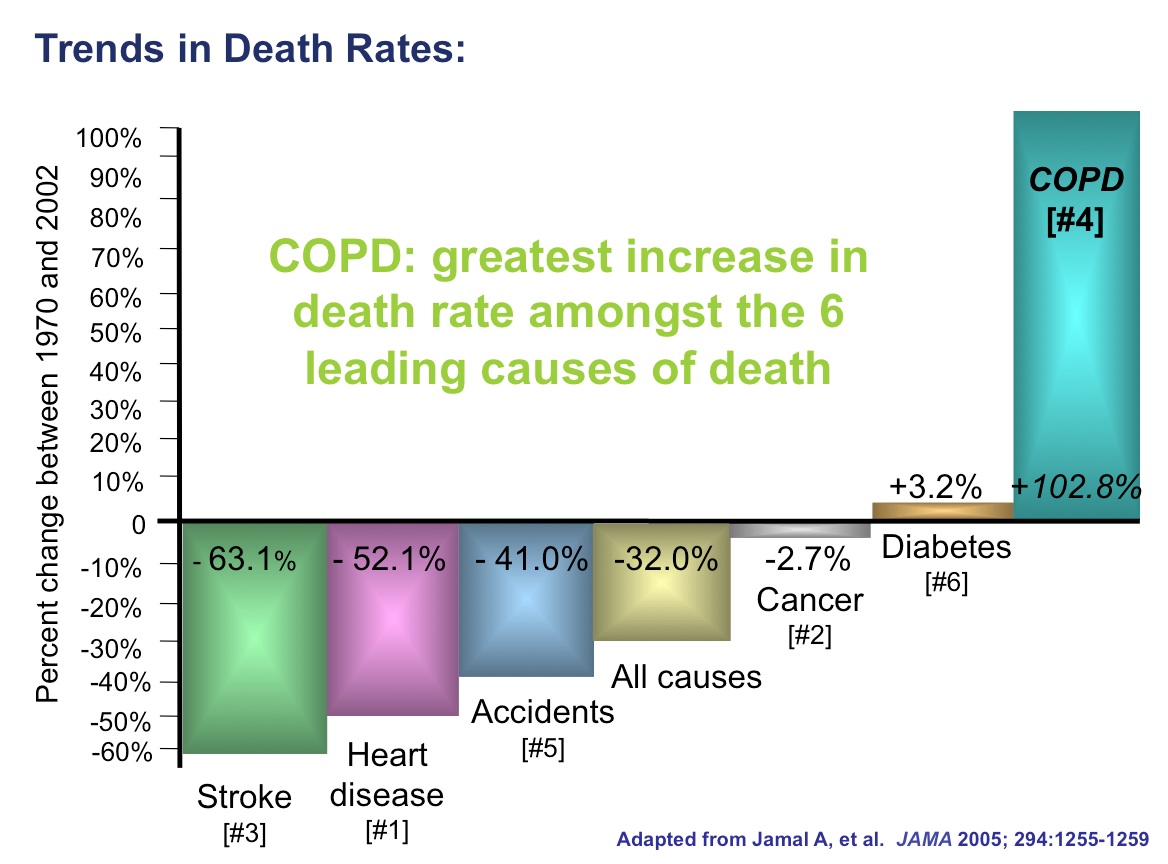
COPD is among the leading causes of hospital admission and it is the fourth leading cause of death. It is the only leading cause of death for which mortality rates continue to increase.
Like prevalence rates, mortality rates may also be underestimated in COPD. This is because the systemic complications of COPD, such as pneumonia and heart failure, may be listed as the cause of death for individuals with COPD.
While accurate prevalence and mortality rates for COPD have been difficult to obtain, it is certain that COPD presents a growing burden on Canadians.
The Burden of COPD #
The high prevalence, morbidity and mortality present a substantial burden for patients, families and health care systems in Canada. The impacts of the disease are social, emotional, and economic.
Patient Burden:
For patients, COPD is a disease that has a profound effect on quality of life and it is often the cause of premature death in these individuals.
As the disease progresses, breathlessness on exertion usually increases, severely limiting tolerance for physical activities. This can lead to a downward spiral of limited physical activity, reduced excercise capacity, and further worsening of breathlessness on exertion.

The disability seen in advanced COPD can often mean that patients experience great restriction in their daily activities. Patients may lose time at work and eventually have to give up work entirely. Patients who are homebound can become socially isolated. COPD can have a great emotional impact on some patients causing frustration, anxiety, depression, loneliness and the fear of becoming a burden to family.
Family Burden:

As patients with COPD require an increasing level of care, the role of caregivers can also become stressful, both emotionally and ecomomically. Families experience the emotional strain of watching the disease progress in their loved ones. They might experience anxiety, depression and social isolation. In advanced COPD, the cost of additional services and therapies may present a financial burden to families. Financial costs can also be associated with loss of productivity of both the patient and family.
Caregiver fatigue is not uncommon among family members of those with COPD.
Health Care System Burden:
COPD places an enormous strain on Canada’s health care system. It is among the leading causes of hospital admission in Canada and it has the highest readmission rate of any chronic disease. Acute exacerbations of COPD and comorbid conditions, such as depression and cardiovascular disease, greatly contribute to the high hospitalization rate for the disease.

Even in stable COPD, patients require a broad range of chronic therapy, health care programs, and community services. They typically experience frequent physician visits and may require home care or supportive housing.
Signs and Symptoms #
Clinical signs and symptoms of COPD are often absent early in the course of the disease. As well, symptoms may not be consistently present at any stage of the disease. When symptoms are intermittent, they are often provoked by irritants such as cigarette smoke. Severity of symptoms is generally related to the amount of lung damage present.
It should be remembered that COPD is a slowly progressive disease. Early symptoms are non-specific and may be missed or wrongly attributed to lack of fitness, the normal aging process, or an inevitable consequence of smoking. As previously mentioned, misdiagnosis is also common, since the symptoms of COPD are common to many other diseases.
Although physical examination and assessment of symptoms are important when COPD is suspected, a formal diagnosis requires spirometry testing. The diagnosis of COPD and spirometry testing are addressed in more detail in the unit COPD-103: Diagnosis And Severity.
Common Signs and Symptoms
- Persistent Cough
- Shortness of breath (Dyspnea)
- Changes in sputum
- Wheeze
- Frequent lung infections
Persistent Cough: Coughing is often the first symptom to develop in COPD. It can be an intermittent cough or chronic and persistent. The cough may be a dry, non-productive cough or it may be accompanied by an increase in sputum production, often known as a “smoker’s cough”.
Shortness of Breath (Dyspnea): The feeling of shortness of breath, or dyspnea, is the most common symptom of COPD. It can become very uncomfortable and distressing and it is often the main symptom that brings patients to first seek medical attention, particularly when it interferes with daily activities. Initially, most patients will be short of breath during exercise only, but as the disease progresses, dyspnea tends to gradually worsen so that it can occur during everyday activities or even at rest.
Patients who experience shortness of breath, also often complain of tiredness and fatigue. These symptoms can present a great challenge for patients with COPD as they discourage maintaining an active lifestyle. A decreased exercise tolerance leads to further decline in fitness and stamina.
Changes in sputum: Another common symptom of COPD is a change in sputum. These changes might include an increase in the amount of sputum produced, an increase in the thickness or stickiness of sputum, and changes in sputum color to yellow or green. Changes in sputum are seen more often in chronic bronchitis than in emphysema, and are often provoked by irritants such as cigarette smoke. Patients with COPD often experience difficulties in coughing up their sputum. A lot of energy can be used in coughing and clearing secretions from the airways, further contributing to feelings of fatigue and breathlessness.
Wheeze: When the airways of the lung become obstructed in COPD, air has difficulty escaping. Airway narrowing can occur from a tightening of the airway muscles, inflammation of the tissues, or an accumulation of mucus. When air is squeezed out through these narrowed passages, a wheezing sound is the result. This is generally heard during auscultation of the lungs, but in severe situations it may be audible without a stethoscope. During times of wheezing, the patient may be seen trying to force the air out of their lungs, with a prolonged exhalation time and use of accessory breathing muscles.
Frequent lung infections: Patients with COPD may experience lung infections more frequently than usual and these infections may may persist longer than what is considered normal. Sputum that accumulates in the airways can trap bacteria and viruses causing colds, influenza, acute bronchitis or pneumonia.
Advanced COPD #
COPD ultimately affects more than just the lungs. As the disease progresses, severe airway obstruction and compromised gas exchange can lead to pronounced physical and systemic changes. Evidence of these changes is seen with laboratory testing, physical examination, and radiology. The effects of advanced COPD are outlined below.
Blood gas changes:
As COPD progresses, gas exchange often becomes more severely impaired across the surface of the lung. Hypoxemia, or low blood oxygen levels, may be seen using pulse oximetry or by measuring arterial blood gases. Cyanosis, or blue discoloration of the face, might occur as a result of hypoxemia. Clubbed fingers and polycythemia might also be seen as a physiological response to chronically low blood oxygen levels.
Hypercapnea, or high carbon dioxide levels, might also seen during arterial blood gas measurement. Hypercapnea often progresses slowly in COPD and may have few symptoms. However in severe cases it can cause confusion, drowsiness and muscle twitches.
Hypoxemia and hypercapnea might also be seen in earlier stages of COPD progression, during flare-ups or “acute exacerbations”.
Changes in physical appearance:
Severe weight loss and generalized muscle wasting is commonly seen in patients with advanced COPD. This may be owing to the high energy requirements associated with an increased ventilatory demand related to capacity of the respiratory muscles. As well, symptoms of fatigue, tiredness and depression may lead to a lack of exercise and decreased appetite.
Over time, COPD patients can develop a barrel-shaped chest as a result of chronically overinflated lungs and breathing at higher lung volumes. In order to cope with hyperinflated lungs and expiratory flow limitation, COPD patients often exhibit abnormal breathing patterns. Pursed-lip breathing, or breathing out slowly through pursed lips, assists with expelling of trapped air from the lungs. ( Click here to see a video of pursed-lip breathing. ) Paradoxical abdominal movement and increased use of the muscles of the neck and shoulders might also be seen in late stage COPD. COPD patients may adopt body positions that relieve breathlessness while sitting or standing. This includes the “tripod position” – leaning forward with arms outstretched with weight supported on the knees or a table.
In late stage COPD, physical signs of right-sided heart failure may appear. Cor pulmonale occurs as a result of chronic hypoxemia and an enlargement of the right ventricle of the heart. Signs of cor pulmonale include peripheral edema (swelling of the ankles and feet), and enlargement of the jugular veins
Radiological changes:
Although chest x-rays are not always useful in COPD management, radiological changes can sometimes be seen in advanced COPD. For example flattened diaphragms may be present, resulting from hyperinflation of the lungs. As well an increased lucency of the lung fields may indicate a loss of lung tissue and increased air spaces.
Acute Exacerbation #
As described earlier in this module, COPD is characterized by episodes of worsening of symptoms, called acute exacerbations. Acute exacerbations tend become more frequent and severe as the disease progresses. Exacerbations account for the majority of health care usage in COPD, and one of the main goals of COPD management is to prevent these flare-ups from occurring.
Signs and Symptoms of Acute Exacerbation of COPD (AECOPD):
During acute exacerbations, particularly severe ones, patients may show signs of respiratory distress. These signs indicate the need for a change in routine therapy or even hospitalization.
Typical signs of distress in AECOPD include:
- Tachypnea (respiratory rate >25)
- Wheezing, crackles or quiet breath sounds over the lung fields on auscultation
- Prolonged expiratory time
- Active use of accessory muscles of breathing (eg. neck muscles, abdominal muscles)
- Retraction of the lower costal interspaces during inspiration
- Breathing through pursed lips
During AECOPD, patients will often complain of an increase in shortness of breath either at rest of with minimal exertion. Sputum thickness and quantity increases and it generally changes colour from white to yellow, green, or brown. Patients typically feel tired and unwell and cold symptoms or a fever may also be present.
The causes and management of AECOPD is addressed in module COPD-106: Acute Exacerbation.
References #
- Life and Breath: Respiratory Diseases in Canada (PHAC) 2007 (http://www.phac-aspc.gc.ca/publicat/2007/lbrdc-vsmrc/index-eng.php)
- O’Donnell DE, Aaron S, Bourbeau J, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease – 2007 update. Can Respir J. 2007;14(Suppl B):5B-32B.
- O’Donnell DE, Hernandez P, Caplan A, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease – 2008 update – highlights for primary care. Can Respir J. 2008;15(Suppl A):1A-8A.
- Pauwels RA, Buist AS, Calverley PM, et al: GOLD Scientific Committee: Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001, 163: 1256-1276
- Gershon AS, Warner L, Cascagnette P, Victor JC, To T. Lifetime risk of developing chronic obstructive pulmonary disease: a longitudinal population study. Lancet 2011; 378: 991–96
- WHO. World Health Statistics 2008. Switzerland: World Health Organization, 2008.
- Canadian Community Health Survey (CCHS) of 2005
- Canadian Thoracic Society. The Human and Economic Burden of COPD: A leading cause of hospital admission in Canada. Feb 2010. 8 p.
- Guidelines and Protocols Advisory Committee. Chronic obstructive pulmonary disease. Medical Services Commission, BC Ministry of Health; 2005.
- Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary diseases (GOLD) guidelines (updated 2009).
- Bourbeau J, Nault D, Borycki E. Comprehensive management of chronic obstructive pulmonary disease. Hamilton: BC Decker Inc, 2002