Description #
This unit will review the potential adverse reactions of the Bier block with a brief discussion of management and prevention.
Learning Objectives #
1) To understand and be able to apply the technique of a Bier block for fracture reduction
2) To understand the management of potential complications of Bier blocks including drug and pneumatic cuff related complications
3) To be able to clearly communicate the risks and benefits of the Bier block procedure to patients and their families
Introduction: #
Fractures, and in particular distal radial and ulnar fractures, are among the most common injuries presenting to the Pediatric Emergency Department (PED) [1]. These fractures can usually be managed by closed reduction in the PED [2]. Pain from reduction of upper-extremity fractures is generally mediated by the use of procedural sedation using a variety of intravenous and intramuscular medications [3]. Alternatively, the pain from reduction can be controlled by regional intravenous anesthesia (Bier block). Currently in our tertiary care PED, most fractures are reduced using procedural sedation with intravenous (IV) Ketamine.
PED procedural sedation protocol requires that an emergency physician administer medications and be present throughout the procedure in case of airway or other complications. While procedural sedation is an excellent way to manage fractures, it requires considerable physician, nursing and other staff resources, and may involve a long recovery period. For older children and adolescents, there is a higher rate of psychotomimetic reactions from Ketamine, and a higher incidence of adverse airway events and nausea/vomiting [3,4]. These increased side effects make this protocol less desirable for older patients. Having the ability to avoid Ketamine in certain patients while still providing adequate pain control would be an excellent option for fracture reduction management.
The Bier block is a proven and effective alternative means of controlling pain from reduction, without the negative side effects of systemic medications or the demands on departmental resources. The technique was developed in the early 1900s and has come in and out of popularity throughout the last century [5]. The Bier block consists of inserting an intravenous catheter into the fractured arm, elevating the arm for several minutes and placing a pneumatic cuff on the upper arm. Once the cuff is inflated, a solution of Lidocaine is injected into the arm and within approximately 15 minutes, there is good anesthesia. The fracture is reduced and casted, and then the cuff is deflated slowly to prevent a large Lidocaine bolus entering the circulatory system [5].
Advantages of Bier Blocks over Procedural Sedation #
The advantages of Bier blocks over procedural sedation can be summarized in the following acronym:
What is a Bier Block? #
The Bier block is a technique of limb anesthesia which does not require systemic medication. An intravenous catheter is placed in the patient’s broken limb, which is then elevated for two minutes to allow passive blood drainage. Following elevation, a blood pressure cuff is placed proximal to the fracture, with soft-roll underneath for comfort, and inflated to pressures well above systolic to occlude blood flow to the limb. The picture below shows the Bier block set-up.

Page 1 #
Once the limb blood flow has been occluded, Lidocaine is injected into the arm (note the normal mottling of the skin in the picture below). After Lidocaine injection, the IV is then removed prior to fracture reduction. Within 10 or 15 minutes, the limb is anesthetized allowing closed reduction of the fracture.
 #
#
Page 2 #
Once the fracture is reduced and satisfactory alignment is confirmed by imaging, the limb is casted.
 #
#
The cuff is deflated slowly using a deflation then re-inflation technique over several minutes. The length of time needed to reduce the fracture and cast the arm allows the Lidocaine to be tissue bound so that no bolus is delivered to the systemic circulation. For greater detail, please see the linked Bier block protocol for the Montreal Children’s Hospital.
Absolute contraindications include:
- Allergy to local anesthetics (rare)
- Pathologic hypertention
- Seizure disorders
- Blood dyscrasias (ex: Hemophelia, sickle cell)
- Crush injury or compromised circulation (compartment syndrome, Reynaud’s disease or peripheral vascular disease)
- Complex medical condition
- Open fracture
- Infection of the limb
- Methemoglobinemia
- Morbid obesity
- Procedure required in both arms
- Patients not eligible for procedural sedation
- Parent/Patient refusal
Relative contraindications include:
- Age < 6 years
- Patient anxiety
- Morbid obesity
- Inability to tolerate cuff inflation
- Anticipated procedure time > 1 hr
Complications of Bier Blocks can be divided into two categories: #
In a series of over 1800 patients receiving Bier blocks at the Whistler Health Care Centre, there were no significant morbidity or mortality [5]. In addition, a recently published two year retrospective review comparing pediatric reductions done with Bier blocks to procedural sedation at the Atlanta Scottish Rite Hospital found no major complications in the 600 patients reduced using Bier blocks for analgesia of the limb. Although the Bier block has been shown to be safe in the literature and in practice, awareness of potential complications allows providers to be prepared for the worst.
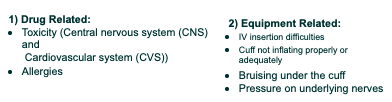
Drug Related Complications: #
CNS Toxicity:
Local anesthetics are lipophilic, weak bases that easily cross the blood-brain barrier. Animal models have shown that hypercapnia or acidosis increases the risk of CNS toxicity from local anesthetics [6]. In general, because the CNS is more susceptible than the CVS to the actions of local anesthetics, CNS symptoms normally precede CVS symptoms.
Notes:
1) The maximum dose for Lidocaine is 3 mg/kg without Epinephrine.
2) Aminoamides (such as Lidocaine) are metabolized primarily by hepatic cytochrome P450-linked enzymes.
3) Systemic toxicity (neurologic and cardiac) is increased in patients with right-left cardiac shunts.
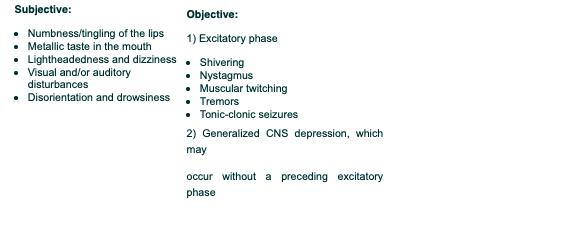
Progressive Symptoms and Signs of CNS Toxicity: #
Management: Routine CNS depression and seizure management are recommended, however, in the management of lidocaine induced seizures, should it become necessary start a second line agent after benzodiazepines, barbiturates ( phenobarbital) are recommended rather than phenytoin ( Dilantin), as phenytoin shares pharmacologic properties ( i.e., sodium channel blockade) with lidocaine and may potentiate toxicity.
Direct Cardiac Effects of Local Anesthetics: #
Local anesthetics primarily act on sodium channels by decreasing the rate of depolarization [7]. Extremely high concentrations of local anesthetics depress pacemaker activity in the sinus node, resulting in sinus bradycardia and sinus arrest.
All local anesthetics exert a dose-dependent negative inotropic action on cardiac muscle proportionate to their potency. In addition, Bupivacaine binds irreversibly to cardiac muscle. Thus, bupivacaine is a more potent cardiodepressant than Lidocaine [8].
Ventricular arrhythmias may occur after rapid intravenous administration of a large dose of Bupivacaine but far less frequently with Lidocaine [9]. For the above reasons, Lidocaine is the local anesthetic of choice for Bier blocks.
Direct Peripheral Vascular Effects: #
At low concentrations, Lidocaine and Bupivacaine produce vasoconstriction, whereas high concentrations cause vasodilation. Local anesthetics also increase pulmonary vascular resistance, but this response may reflect circulatory or respiratory depression from the drugs’ effects on the CNS.
Management #
Studies suggest that a bolus of 20% Intralipid followed by infusion until the patient is stable may improve outcomes in cases where Bupivicaine was accidentally used instead of Lidocaine, or where severe toxicity persist from any local anesthetic. It is thought that the IV fat emulsion works by extracting the lipid soluble local anesthetic molecules from the aqueous plasma phase [10]. Thus, in addition to routine management of cardiac arrest, one should consider Intralipids if symptoms of local anesthetic toxicity persist. Please see MCH treatment algorithm below for more details:
MCH Bupivacaine Toxicity Algorithm:
Summary of Signs and Symptoms of Lidocaine Toxicity #
The symptoms (italics) and signs of Lidocaine toxicity can be easily remembered using the following mnemonic:
#
#
Allergies: #
Allergic reactions to Lidocaine are very rare.
Prospective studies indicate that very few suspected reactions are confirmed to be allergic reactions [11]. Although the aminoamide anesthetics, such as Lidocaine, appear to be relatively free of allergic-type reactions, solutions of these drugs may have come in contact with latex or contain a preservative, methylparaben, which may cause anaphylaxis [12]. Routine anaphylaxis treatment would be appropriate in such cases. Click here to see MCH Anaphylaxis Guideline (https://cyberpatient-assets.s3-us-west-2.amazonaws.com/production/assets/EducationalResources/Diagnostic+and+procedural+imaging+/Medical+imaging/thoracic+radiology/ACUTE_TREATMENT_OF_ANAPHYLAXIS.pdf)
Note: Local anesthetics are available in a preservative-free preparation.
Equipment Related Complications #
The Bier block machine, known as the Automatic Tourniquet System 3000, needs to be checked prior to every usage for leaks in the bladders of the cuff or tubing. Usually, cuffs with two bladders are used so that there is a back-up cuff. The second cuff can also act as an alternative when the cuff pressure becomes uncomfortable for the patient (the second cuff can be inflated then the inital cuff deflated).
Mohr and collegaues, in their patient series of 1816 Bier block procedures had only 3 cases of improper cuff inflation (a rate of 0.17%) none of which resulted in mortality or morbidity [5]. Given that the patient is conscious throughout the procedure, they are able to report lack of pressure or changes in the cuff feeling reducing the possiblity of significant morbidity or mortality.

Prevention and Precautions: #
The following recommendations are suggested to decrease the risk of adverse reactions with Bier blocks:
- Set machine pressure above baseline BP
Remember to always set the machine’s pressure above the patient’s baseline BP. We will cover how to calculate and adjust proper limb occlusion pressure and return to profusion pressure on the day of the course.
- Fully inflate cuff and test cuff pressure prior to injection
Prior to injection, test the cuff with a quick squeeze to ensure that it is inflated and tight, and to ensure that pressure is well maintained.
- Inject IV Lidocaine slowly over 1-2 minutes
Observe for normal blanching or mottling of the skin, and for signs of toxicity (remember the LIDOCAINE mnemonic).
- Resuscitation Equipment and Medications:
The potential for respiratory depression, seizures and even cardiac arrest necessiates full monitoring. Resuscitation equipment and medications should be immediately available in the emergency cart.
Note: Attention to the ECG may be the difference between a toxic and lethal dose.
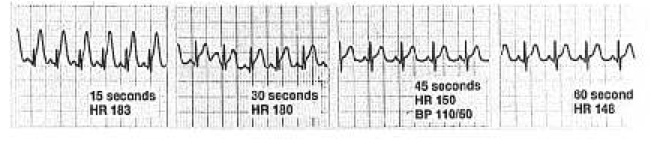
Figure 2: Profound ST elevation and increased T-wave amplitude 15 seconds after an intravascular injection with Bupivacaine with Epinephrine followed by decreased heart rate and rapid resolution of ST-T changes after stopping the injection [13].
A few more tips: #
- Choose your local anesthetic solution wisely
Plain Lidocaine is the anesthetic of choice for Bier blocks and will be the only one available in our department for this procedure.
- Repeating blocks after a failed reduction (this may be an indication for the OR)
Repeated blocks can be done within two hours, at the physician’s discretion. However, failed reduction may be an indication for the O.R. not for a trial of procedural sedation.
- Post-block care
Two sets of vital signs need to be done after cuff release. The patient is fit for discharge after 20 minutes post-cuff release, and if needed may go for confirmatory x-rays after the two sets of vital signs are taken. Ideally, the patient should not need to go to the observation room post-procedure.
Summary #
The Bier block is a relatively quick method of intravenous anesthesia for fracture reduction. It is low risk and does not require fasting or sedation.
Using the Bier block avoids the risks of systemic drugs used for procedural sedation.
Being knowledgeable of the potential adverse reactions to local anesthetics will better prepare you should one occur, and help you to safely perform this technique on your patients.
Thank you for taking the time to do the online component of the course.
References: #
[1] Migita RT, Klein EJ, Garrison MM. Sedation and analgesia for pediatric fracture reduction in the emergency department. Arch Pediatr Adolsec Med. 2006;160:46-51.
[2] Blasier RD, White R. Intravenous regional anesthesia for management of children’s extremity fractures in the emergency department. Pediatric Emergency Care. 1996;12(6):404-6.
[3] Kennedy RM, Luhmann JD, Luhmann SJ. Emergency department management of pain and anxiety related to orthopedic fracture care: A guide to analgesic techniques and procedural sedation in children. Pediatr Drugs. 2004;6(11):11-31.
[4] Green SM, Roback MG, Krauss B, Brown L, McGlone RG, Agrawal D, et al., Predictors of airway and respiratory adverse events with ketamine sedation in the emergency department: an individual-patient data meta-analysis of 8,282 children. Ann Emerg Med. 2009;54(2):158-68.
[5] Mohr B. Safety and effectiveness of intravenous regional anesthesia (Bier block) for outpatient management of forearm trauma. Can J Emerg Med. 2006;8(4):247-50.
[6] Englesson S: The influence of acid-base changes on central nervous system toxicity of local anaesthetic agents. I. An experimental study in cats. Acta Anaesthesiol Scand 1974; 18:79-87.
[7] Wagman IH, De Jong RH, Prince DA: Effects of lidocaine on the central nervous system. Anesthesiology 1967; 28:155-172.
[8] Lynch 3rd C: Depression of myocardial contractility in vitro by bupivacaine, etidocaine, and lidocaine. Anesth Analg 1986; 65:551-559.
[9] Kotelko DM, Shnider SM, Dailey PA, et al: Bupivacaine-induced cardiac arrhythmias in sheep. Anesthesiology 1984; 60:10-18.
[10] Weinberg GL: Current concepts in resuscitation of patients with local anesthetic cardiac toxicity. Reg Anesth Pain Med 2002; 27:568.
[11] Baluga JC, Casamayou R, Carozzi E, et al: Allergy to local anaesthetics in dentistry. Myth or reality?. Allergol Immunopathol 2002; 30:14-19.
[12] Shojaei AR, Haas DA: Local anesthetic cartridges and latex allergy: A literature review. J Can Dent Assoc
[13] Claudio RE, Hadzic A, Shih H, Vloka JD, Castro J, Koscielniak-Nielsen Z, Thys DM, Santos AC: Injection pressures by anesthesiologists during simulated peripheral nerve block. Reg Anesth Pain Med 2004; 29: 201-5
[14] Freid,E B M.D; Bailey, A G M.D; Valley, R D M.D: Electrocardiographic and Hemodynamic Changes Associated with the Unintentional Intervascular Injection of Bupivacaine with Epinephrine in Infants, Anesthesiology 1993; 79: 394-398.
[15] Google images
[16] Dr. Weinberg, Bupivacaine Toxicity in a Rat Rescued by Lipid emulsion video clip