Description #
This unit is designed to review the skills involved in respiratory assessment. This unit will be administered online followed by a pre and post quiz. Accumulated knowledge from all of the units will be practiced and evaluated via case scenarios using the simulated patient.
Learning Objectives #
At the completion of this module the student will be able to:
1. Describe the techniques for completing a respiratory assessment.
2. Be able to undertake a basic respiratory assessment of a patient.
3. Identify normal and abnormal clinical findings including physical assessment findings, lab and diagnostic results.
Introduction #
Basic Respiratory Assessment #
It is vitally important for all physiotherapists, in all practice settings, to be able to perform a basic respiratory assessment. This includes taking a patient history, the use of the techniques of inspection, palpation, percussion, and auscultation and review of relevant diagnostic tests.
A complete respiratory assessment should include a full multisystem assessment. This allows therapists to accurately identify the aspects of pathophysiology that are amenable to treatment and helps to highlight any further complications that may impact treatment choices.
Outline of topics:
- Patient Interview (subjective assessment)
- Physical assessment (objective assessment)
- Including a video of basic hands on respiratory assessment
- Physiotherapy problem list and treatment options
Key Points for Assessment #
Multisystem Assessment #
A multisystem assessment is essential when completing a respiratory assessment. The elements of a multisystem assessment are listed below:
Interview #
- History of Present Compliant
- Past Medical History
- Function
Physical assessment #
- Vitals
- Inspection
- Palpation
- Auscultation
- Respiratory Tests – CXR, ABGs
- MSK assessment
Diagnosis #
Four main respiratory physiotherapy problems should be considered:
- Sputum Retention
- Decreased Lung Volume
- Increased Work of Breathing
- Respiratory Failure
Patient Interview #
You should always attempt to begin your respiratory assessment by completing a patient interview. Starting the assessment with an interview helps you establish rapport with the patient and may lessen the patient’s anxiety. During the history, you will be gathering information about the patient’s current and any previous respiratory problems. You may interview the patient, and in some cases, family members or significant others.
When undertaking your patient interview you will want to include:
Consent for treatment #
History of Presenting Complaint (HPC) #
Events leading to admission, surgery/medical condition.
Cardinal Signs #
- Pain – Cardiac chest pain is likely to be central, crushing and radiating to the left arm and neck. For other sources of pain ensure there is adequate analgesia to allow treatment.
- SOB – leads to fatigue, what can you do to relieve the WOB?
- Cough +/- Sputum (consistency/quantity/colour, what and how much is normal for the patient) – remember a cough will only clear the central airways. Is the patient wasting energy on a unproductive cough?
- Wheeze – what is the cause, swelling, bronchospasm or sputum. Are there any clues in the PMH as to the most likely causes?
Past Medical History (PMHx) #
- Lung disease eg asthma COPD lung ca, Previous Surgery, Environmental Exposure, allergies, Sleep Apnea, Orthopnea, Heart Disease/Cardiac Hx, Medical conditions.
- Recent hospital admission
Think about – underlying pathologies that may impact on patients care? Contraindications to treatment/previous or similar admissions/previous physiotherapy treatments and there effectiveness
Medications #
- Take note of any meds. Look for Cardiac meds/Diuretics/Inhalers (Bronchodilators/steroids etc)
- Home Oxygen – If on any, what type (exertional based, 18 hr/day, 24 hr/day). Its important to note how much Oxygen prescribed, and how often it is used.
Baseline Function and Exercise Tolerance #
How far can the walk? How long to recover? SOBOE?
Usual Activity Levels?
Social history #
- Employment
- House set up. Eg stairs
- Supports system – family, home care friends
 #
#
Do they? How much, and for how long? Important to also ask if they are interested in smoking cessation material (most people who want to quit don’t know where to find the resources). From this information can also calculate number of Pack Years (Packs per day x years smoking)
Baseline Arterial Blood Gas and Saturation Measurement #
Important with COPD Patients to also try and find normal ABG’s from previous admissions prior to discharge, so can determine when patients is returning to baseline, also to give guidance about realistic medical goals with regards to O2/CO2 levels.
BORG Scale #
Useful outcome measure. Can ask a patient how they would feel after walking up a flight of stairs/a city block.
The following are a selection of questions that you may want to consider asking during your patient interview: #
Are you having any trouble breathing?
Do you have any chest pain with breathing? If so, what is the pain like, when does it occur, and what relieves it?
Do you have a cough? If yes, what does the cough sound like, when does it occur, do you bring up any sputum when you cough?
What does the sputum look like?
Are you ever short of breath? If so, does your shortness of breath occur at rest or with activity? Do you have any problems breathing at night? If so, do you use pillows to help you get in a position to breathe easier?
Do you have any allergies? If yes, how does your allergy affect your breathing?
Do you smoke now or have you ever smoked? If yes, how many years did you smoke and how many packs of cigarettes did you smoke daily?
What kind of work do you do/did you do? In your work are/were you exposed to substances such as asbestos, chemicals, or cigarette smoke?
Predisposing Factors to Respiratory Complications #
Predisposing Factors
The following are factors that can predispose an individual to respiratory complications. They should be considered as a whole and used as part of your respiratory assessment. They include:
Age
>50 increases predisposition to various medical complications
Past Medical History
Anything likely to “slow down” mobility (orthopaedic/neurological/medical conditions)
Cardiopulmonary history is especially of note
Obesity

Increases risk of diabetes/cardiac problems and a host of other medical complications
Ranges of mobility from decreased to complete immobility
Leads to basal atalectasis
Smoking
Depresses sputum motility
Can be a useful motivator to get people mobile
Substance Abuse
Can lead to withdrawal/DT’s/personality issues
Can delay/prolong recovery as person comes out of withdrawal, or may be unsafe to mobilise whilst in early stages
Anaesthetic
Spinal v General
Length of time under
Increased age has higher risk of post anaesthetic delirium
Patients undergoing heart surgery with Heart Bypass Pump often develop ‘pump brain’ delirium
Surgical Location/Length
Surgical incision in the “Strike Zone”
Most patients have false sense of what they will not be allowed to do, or unanticipated pain levels… reassurance is required.
Objective Assessment #
General observation #
You should do a full multisystem assessment in order to fully understand the pathophysiological problems you find. Many respiratory issues can secondary to other disease processes. In this section we will look at the following items:
CNS #
- Level of consciousness
Cardiovascular #
- Heart rate
- Blood pressure
- ECGs
- Temperature
- Edema
Respiratory #
Inspection
- Mode of ventilation
- Oxygen therapy
- Pulse oximetry
- Breathing pattern/RR/WOB
- Cough and sputum
- Chest Shape
- Skin
- Hands
Palpation
- Expansion
- Tactile fremitis
- Subcutaneous emphysema
- Tracheal deviation
Percussion
Auscultation
- Breath sounds
- Added sounds
Tests
- ABGS
- CXR
- Blood work
Renal #
- Urine output
- Fluid balance
Musculoskeletal #
- ROM
- Strength
- Mobility
General Observation #
As you begin to observe your patient, it is important to be thinking about the following things.

Comfort – Does the patient look comfortable, or unwell and distressed?
Position – What position do you find them in? Position has a real impact on lung volumes and work of breathing
Size – Are they obese? Is there manual handling and treatment choice issues as a result? Are they malnourished?
Diaphoresis – Are they Sweating? Do they have clammy skin?
Lines/Tubes – What equipment is attached to the patient?
- IV Pumps, NG Tubes, PEG tubes
- Catheters (Foleys), Ileal conduit, Suprapubic Catheter
- Intercostal Catheters (Chest Drains), Pigtail Catheters, Pleurovac, Haemovac, VAC dressing, Abdominal drains
- Colostomy bag, Rectal tube
- Arterial and central lines
- ECG lines
Scars
New scars from recent surgery – where are they will they impact treatment choices?
Old scars from previous surgery – From position of scars will be able to get rough of idea of what surgery has been performed?
Level of Consciousness #
What is their level of consciousness?
If it is decreased, why might this be?
- Drugs?
- Respiratory status?
- Neurological impairment?
- Pain?
Cardiovascular System #
What to look for #
Look for trends #
- What is the normal status of this patient?
- What physiological stress is the patient under?
- Is there circulation compromised?
Blood Pressure #
- Normal range is 90/60 to 140/90
- 90/60 can indicate Hypotension or Shock
- >170 SBP can indicate a Hypertensive Emergency
- Mean Arterial Pressure (MAP) of around 65 mmHg is required to maintain perfusion to most organs, especially kidneys
Heart Rate/Rhythm #
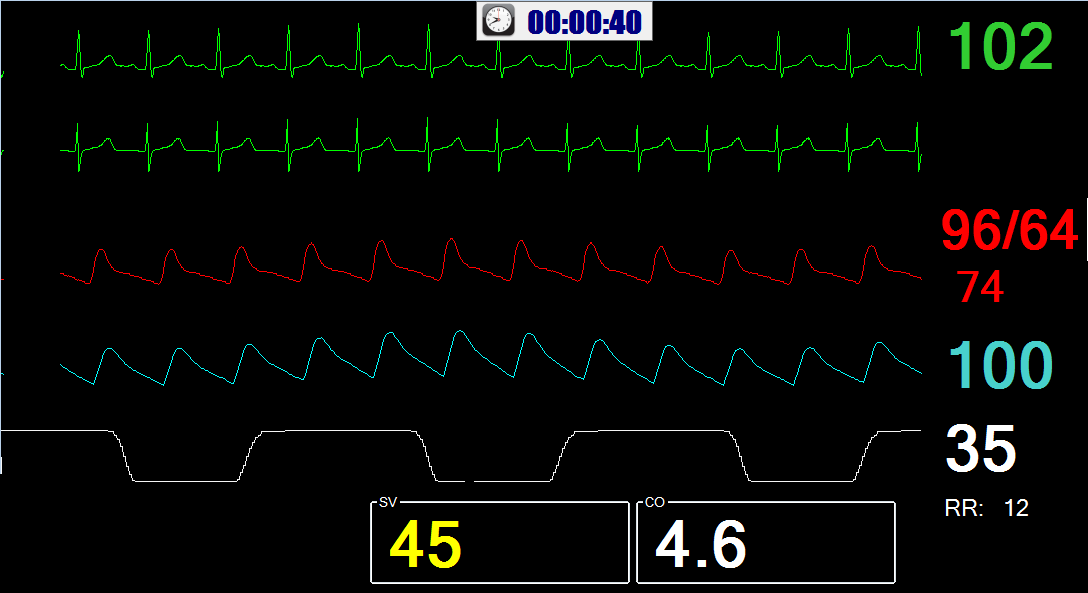
- 70-80 bpm normal
- A rough guide to max HR = 220-age
- ECGs – Check to see if rhythm is regular/irregular (also take note if patient has history of Atrial Fibrilation)
Temperature #
- 36.5oC – 37.5oC Normal
- Increase temperature indicates possible infection
Edema #
Respiratory System #
The following pages will discuss each of the Inspection, Palpation, Percussion and Ascultation (IPPA) sections in greater detail.
Inspection #
You should be looking at the following things in the Inspection portion of your Respiratory Assessment
Chest Wall Shape #
Do they have kypohisis or scoloisis? Is this impacting there breathing?
Oxygen #
Are they on Nasal Prongs, Face mask, High Flow Oxygen Therapy?
What percentage of oxygen is being delivered?
Is the flow rate sufficient to meet the patients demands?
For more details refer to CanHealth Unit on Oxygen Therapy.
Work of Breathing/Breathing Pattern #
Is it laboured?
Can they speak in sentences?
Is there Accessory muscle use?
Is there Supraclavicular/intercostals indrawing?
Is it paradoxical (as in Quadraplegic’s)?
Are they diaphragmatically breathing, or are they splinting?
How would you describe/document their breathing? Apical? Diaphragmatic? Shallow? Deep? Rapid? Slow?
Note: A Respiratory Rate of 12 – 16 is considered normal. >24 breaths per minute can indicate Respiratory Distress
Pulse Oximetry /Oxygen Saturation #
- >95% considered normal without lung pathology
- >90% acceptable in patients with severe lung disease
Be mindful of trends when looking at Saturation levels. If the patient normally saturates in the high 90’s and has trended down to the low 90’s (over hours or sometimes days), this could be the beginning of something more sinister.
Do not forget that the older the patient is, the lower the normal saturation is likely to be, however if a patient without significant lung pathology is <95%, further investigation is warranted.
Cough #
How would you describe it?
- Strong or Weak?
- Effective or ineffective?
- Wet or Dry?
- Productive of sputum?
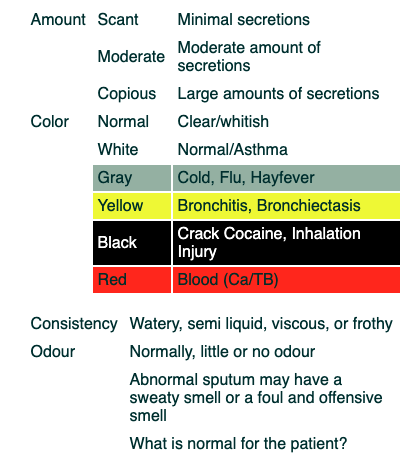
Sputum #
Sputum is mucous material that is expelled (coughed up) from the lungs. It is not saliva. Saliva is produced by the salivary glands in the mouth to keep the mouth moist and to help in the chewing and swallowing of food.
Possible descriptions of sputum include:
Skin Color #

Palpation #
Palpation #
Chest Wall Expansion #
Is there adequate expansion at upper and lower zones of lung fields?
Is it symmetrical?
Paradoxical rib movement?
Tactile Fremitis #
The transmission of secretion vibration in the airways to the chest wall.
Subcutaneous Emphysema #
Subcutaneous Emphysema (or Surgical Emphysema) occurs when air gets into the subcutaneous layer of the skin. This usually occurs in the skin covering the chest wall or neck, but can also occur in other parts of the body.
Subcutaneous emphysema can often be seen as a smooth bulging of the skin. When you palpate the skin, it produces an unusual crackling sensation as the gas is pushed through the tissue. This sensation has been described as similar to touching Rice Krispies. In cases of subcutaneous emphysema around the neck, there may be a feeling of fullness in the neck, and the sound of the voice may change.
If Subcutaneous Emphysema is particularly extreme around the neck and chest, the swelling can interfere with breathing. When seen on XRAY, Subcutaneous Emphysema typically travels in the direction of muscle fibres. It can also take the appearance of dark spots in fatty tissue. Possible causes include:
- Collapsed lung (pneumothorax), often occurring with a rib fracture
- Ruptured bronchial tube or esophagus – Breathing in cocaine Forceful vomiting” (Boerhaave’s syndrome),Pertussis (whooping cough), Corrosives or chemical burns of the esophagus, Diving injuries
- Blunt trauma – Gunshot wounds, Stabbing, Facial bone fracture
- Certain medical procedures that insert a tube into the body, such as chest tubes, a central venous line, intubation, and bronchoscopy
Tracheal deviation #
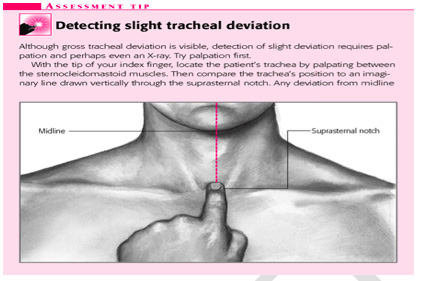
Tracheal Deviation results from unequal intrathoracic pressure within the chest cavity. When Tracheal Deviation is present, the Trachea will be displaced in the direction of less pressure. Meaning, that if one side of the chest cavity has an increase in pressure (such as in the case of a Pneumothorax) the trachea will shift towards the opposing side.
It is most commonly associated with traumatic peumothorax but it can be caused by a number of both acute and chronic health issues. For example:
- Pneumonectomy
- Atelectasis
- Pleural effusion
- Pleural Fibrosis
- some Cancers (tumors within the bronchi, lung or pleural cavity).
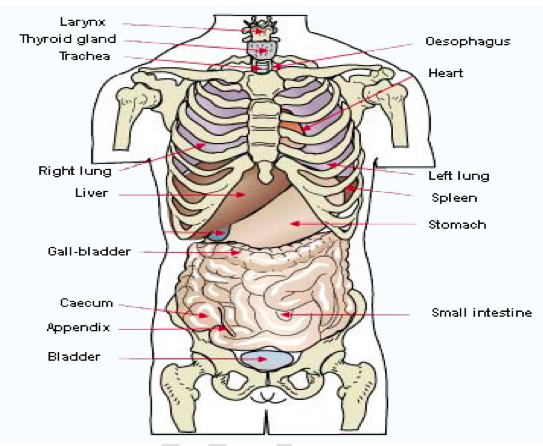
In its normal position, the trachea can be seen and felt directly in the middle of the anterior (front side) neck behind the Jugular Notch of the Manubrium and superior to this point as it extends towards the larynx.
Percussion #
Percussion is a method of tapping body parts with fingers, hands, or small instruments as part of a physical examination.
Percussion was initially used to distinguish between empty and filled barrels of liquor, and Dr. Leopold Auenbrugger introduced the technique to medicine.

The purpose is to evaluate the size, consistency, borders, and presence or absence of fluid in body organs.
There are four types of percussion sounds:
- resonant,
- hyper-resonant,
- stony dull
- dull.
Percussion of a body part produces a sound — like playing a drum — that indicates the type of tissue within the organ:
lungs sound hollow on percussion because they are filled with air.
Bones and joints sound solid.
The abdomen sounds like a hollow organ filled with air, fluid, or solids.
There are two types of percussion:
- A dull sound indicates the presence of a solid mass under the surface.
- A more resonant sound indicates hollow, air-containing structures.
Percussion of the thorax
It is used to diagnose pneumothorax, emphysema and other diseases. It can be used to access the of the thorax
Each zone of the lung should be percussed, comparing side to side, not upper and lower portions of the same lung
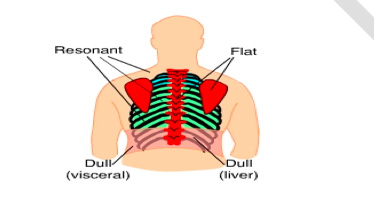
Abnormal Percussion findings:
Dullness: which may be produces by pneumonia, tumour,infarction or fluid collection
Hyper resonance (tympany): which may result from confluent air collection, as seen in pneumothorax or emphysema
Auscultation #
Why Auscultate? #
To assess air entry in different parts of the lungs
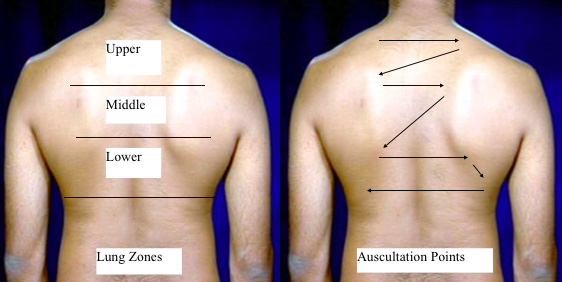
Where? #
Over lung fields
Anterior Chest
Posterior Chest
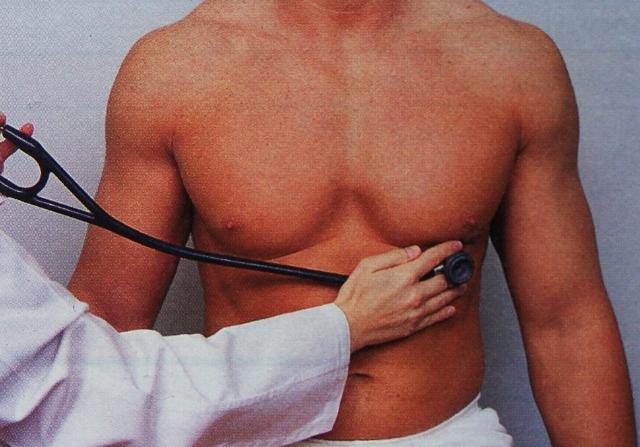
How to Ausculate? #
Use the diaphragm of stethoscope and press firmly with it.
- The stethoscope should be placed on bare skin.
- Patient should breathe through the mouth – slightly deeper than normal breaths (to enhance your ability to hear breath sounds)
- Be sure patient doesn’t hyperventilate, give them rest breaks as needed.
- Need to ensure correct placement used
- Alternate between lungs to compare left to right (or vice versa) rather than upper to lower of same lung
- Evaluate at least one breath in each pulmonary segment.
- Compare intensity, pitch and quality of the breath sounds between lungs.
What will you hear? #
Normal Breath Sounds #
Vesicular – soft and low pitched sound, normally heard over the most of the lung, inspiration is louder and higher pitched than expiration
Altered breath sounds #
Decreased A/E or absent breath sounds can be caused by:
- Atelectasis
- Emphysema
- Pleural effusion
- Hemothorax
- ARDS
- Asthma
- Pulmonary fibrosis
- Neuromuscular weakness
- Musculoskeletal deformities
- Pain
- Pneumothorax
- Obesity
Bronchial breathing: #
Bronchial breath sounds are hollow, tubular sounds that are lower pitched. Inspiration and expiration are both the same pitch and there is distinct pause between the phases of breathing. Often described as “darth vader” breath sounds.
They can be auscultated over the trachea and main bronchi where they are considered normal but if heard else where they are abnormal.
Causes: Bronchial Breath Sounds over the periphery of the lung indicate consolidation and/or lobar collapse or sometimes pleural effusion
Added breath sounds: #
Extraneous noises produced over the broncho-pulmonary tree usually indicate presence of an abnormal process or condition.
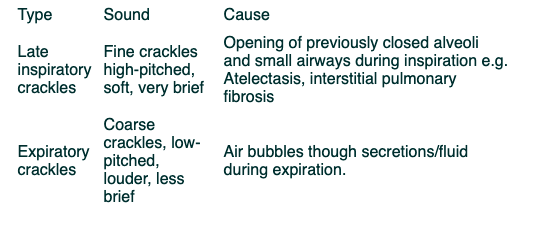
Crackles: #
Discontinuous, nonmusical, brief sounds, heard more commonly on inspiration.
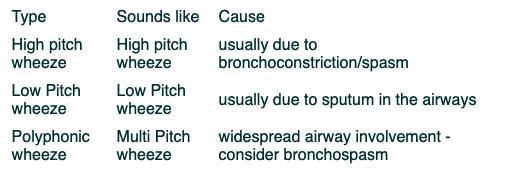
Wheezes: #
Continuous sounds, can be high pitch, low pitch or polyphonic. Heard normally on expiration but sometimes also on inspiration. The wheeze is created by air flowing through airways narrowed by secretions, foreign bodies or obstructive lesions.
Stridor: #
Inspiratory musical wheeze heard loudest over the trachea during inspiration.
Cause: Suggests an obstruction or narrowing of the trachea or larynx. May be life-threatening – no physio – consult the doctors
Other Tests #
In addition to the basic respiratory assessment the following tests can help to form a physiotherapy diagnosis of the respiratory complaint:
- Arterial Blood Gases
- Chest X RAY
- Blood Work
- Pulmonary Function Tests
- CT and V/Q Scan
For more information on any of the above, please follow the hyperlink.
Potential Respiratory Problem List #
Sputum Retention #
Clinical signs may include:
- Increased Work of Breathing
- Inspiratory Crackles, Wheeze, reduced or absent breath sounds
- Secretions audible at the mouth, or secretions palpable through the chest wall
- Audible secretions or coarse wheeze on cough/huff
- ↓ Saturations or PaO2
- Increased PaCO2
- CXR shows patchy shadowing or atelectasis
- Infection
- Increased Temperature
- Increased Heart Rate
- Elevated inflammatory markers
- Patients may describe difficulty clearing secretions with associated clinical deterioration
- Possible associated tachycardia, restlessness, or cyanosis
Clinical Signs in Ventilated patients also include:
- Increased airway pressures if ventilated in volume control modes
- ↓ tidal volumes if pressure control modes (consider alternative reasons for these changes)
- Secretions on suction, with associated clinical deterioration. Alternatively secretions may be difficult to access.
Treatment Options #
Exercise
ACBT
Postural Drainage
Manual Techniques
Humidification
Intermittent Positive Pressure Breathing (IPPB)
Manual Hyper-Inflation (MHI)
If Ineffective Cough
Educate Re: Effective Cough Technique
Assisted Cough (if appropriate)
Suction
Additions with Dr’s Order
Saline Nebuliser
Inhaled Mucolytics
Decreased Lung Volume Signs #
#
Clinical signs will depend on the underlying cause of collapse, but will include:
- ↑ Respiratory Rate
- ↓ Oxygen Saturation
- ↓ Breath Sounds and/ or added breath sounds on auscultation
Causes #
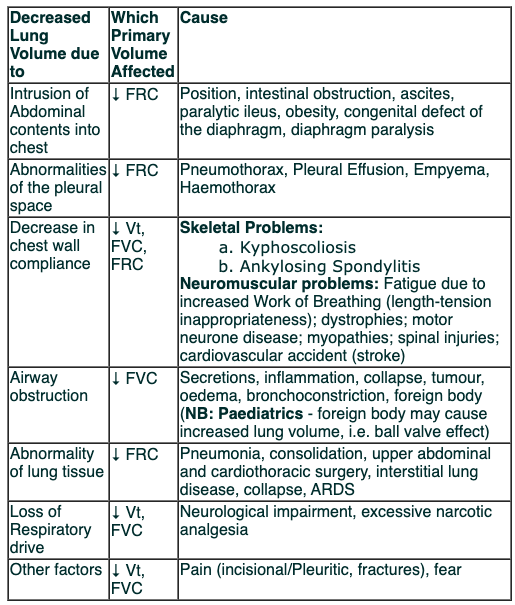
Not all volume loss can be treated by physiotherapy, the diagnosis of underlying cause is important.
Treatment #
Thoracic expansion exercises – inspiratory holds and sniffs
Secretion clearance if inidicated
Positioning
Exercise
IPPB
Incentive spirometry, bubbles
Hands on facilitation techniques
MHI/ ventilator hyperinflation
Pain control
Increased Work of Breathing Signs #

- ↑ Respiratory Rate
- ↓ Heart Rate
- Mouth Breathing
- Altered depth and pattern of breathing (e.g. deep, shallow, irregulat, apnoeas, pursed lip breathing)
- Accessory muscle use
- Reduced SpO2
- Deranged arterial blood gases
- Carbon dioxide retnetion (hypercapnia) may cause:
- peripheral vasodilation; warm hands
- bounding pulse
- flapping tremor of hands
- Secondary signs:
- cerebral – restlessness/irritability/confusion/seizure/coma
- cardiac – tachycardia/hypertension/bradycardia/hypotension/cardiac arrest
- fatigue
Causes and Treatment #
Sputum Retention (see above)
decreased lung volume (see above)
Bronchospasm
- Check bronchodilator technique and compliance
- Use breathlessness positioning to aid relaxation
- Ensure adequate oxygen therapy to meet o2 sat goals set by doctors
- Humidified oxygen therapy should be prescribed
- Breathing control exercises
- Avoid manual techniques
Respiratory Failure #
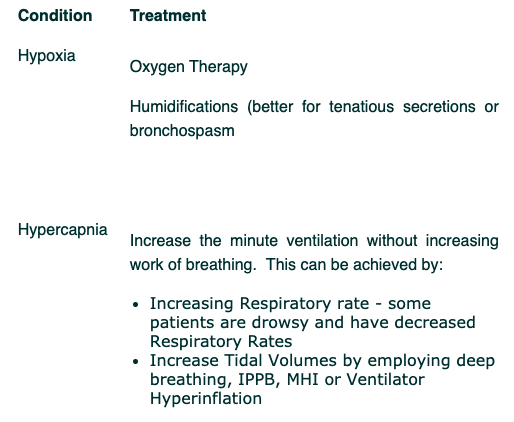
Type 1 Respiratory failure #
Hypoxiaemia with normal or reduced CO2
Type 2 Respiratory failure #
Hypoxiaemia and hypercapina (increased CO2), also know as ventilatory failure
Signs #
Clinical signs of Hypoxemia
- Central cyanosis
- Perpheral cyanosis
- Increased R/R
- Tachycardia
- Low o2 sats
- Confusion and agitation
Clinical signs of Hypercapnia
- Respiratory acidosis
- Agitation and confusion
- Patients is flushed and peripherally dilated, (CO2 is a potent vasodilator)
Causes #
Respiratory Failure can be caused by:
- Respiratory disease
- Cardiac disease -CHF
- Neurological disease/ injury – eg SCI, Guillian Barre
- Fatigue – muscle weakness
- Sleep related breathing disorders – OSA
- Renal failure
- Restriction of the chest wall eg trauma or burns
- Neuromuscular blockade ie poison or anesthesia
- CNS depression
Physiotherapy Treatment #
If primary cause of the respiratory failure is respiratory in nature, treat the cause (e.g. sputum retention, volume loss, bronchospasm).
If the primary cause of the respiratory failure is renal or cardiac in nature, the effects of Physiotherapy treatment are somewhat limited. Liaise with the medical team.
Differential Diagnosis #
What does this all mean? #
The table below is an attempt to provide a tool that can be used to assist you in determining a physiotherapy diagnosis. Please review it to see if it would help you in your clinical practice.
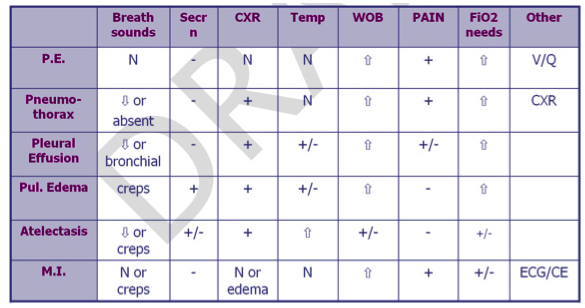
Key: N = normal, – = not apparent, + = apparent, creps = crackles
References #
1. CURRENT Surgical Diagnosis & Treatment, G.Doherty
McGraw-Hill Medical; 12th Edition, 2005
2. Handbook of Surgery: T.R. Schrock
Jones Medical Publications, 10th Edition, 1994
3. The Brompton Hospital Guide to Chest Physiotherapy: B. A. Webber
Blackwell Science 5th Edition, 1988
4. www.rnceus.com
5. Respiratory Physiotherapy, 2nd Edition – An On-Call Survival Guide Edited by Beverley Harden, MSc, MCSP, SRP, Jane Cross, EdD, MSc, Grad Dip Phys, Mary Ann Broad, Matthew Quint, Paul Ritson, MCSP, Grad Dip Phys and Sandy Thomas. Churchill Livingstone.
6. Harden, B, Cross J, Broad, M, Quint, M, Ritson,P & Thomas,S.(2009). Respiratory physiotherapy, an on call survival guide, 2nd edition. Edinburgh: Churchill Livingstone Elsevier.
7. Reid, D & Chung,F. (2004). Clinical management notes and case histories in cardiopulmonary physical therapy. New Jersey: SLACK Inc.