Incision and Drainage of Abscess
From http://www.anwresidency.com/simulation/guide/i&d.pdf
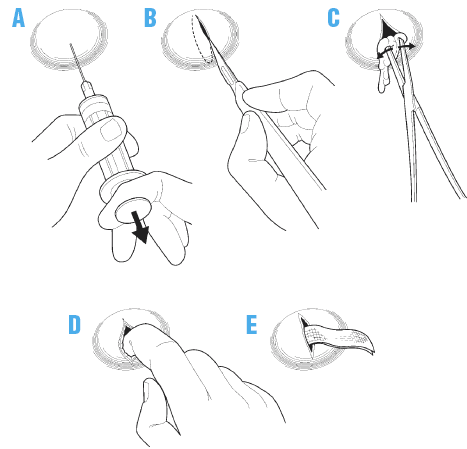
1. Obtain informed consent after discussing the procedure and its risks and benefits with the patient. Wash your hands with antibacterial soap and water before beginning the procedure. Because many abscesses are under pressure, make sure you wear gloves and a face shield at all times during the procedure to avoid exposure to bodily fluids. Apply a skin cleanser, such as chlorhexidine or povidone iodine, in a circular motion, starting at the peak of the abscess. Cover a wide area outside the wound to prevent contamination of equipment.
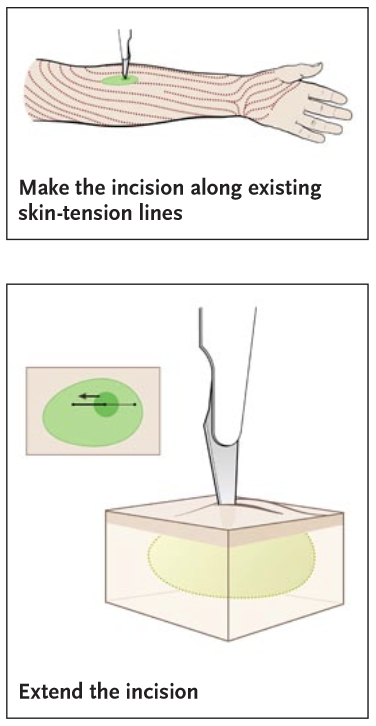
2. Anesthetize the top of the wound by inserting a 25-gauge or 30-gauge needle just under and parallel to the surface of the skin. Inject anesthetic into the intradermal tissues. Make an incision with a scalpel directly over the center of the cutaneous abscess; the incision should be oriented along the long axis of the fluid collection. Purulent drainage will begin when the abscess cavity has been entered successfully. Extend the incision to create an opening large enough to ensure adequate drainage and to prevent recurrent abscess formation; the incision may need to extend the length of the abscess borders.
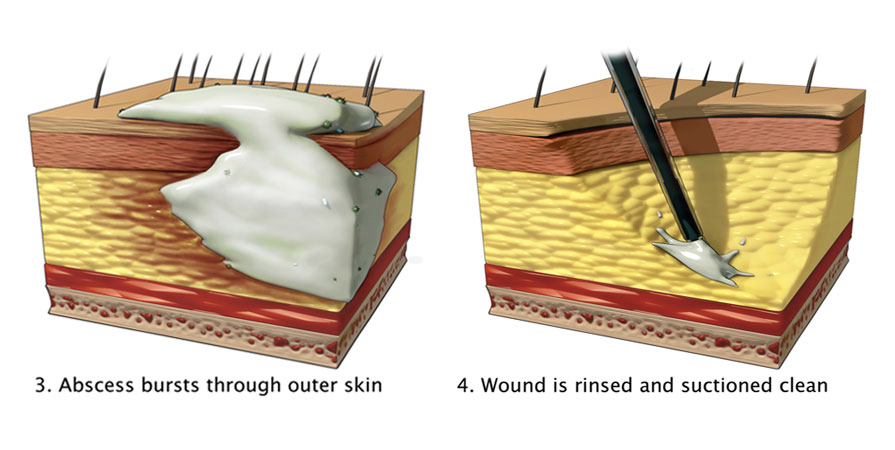
3. After allowing the wound to drain spontaneously, gently express any further contents.
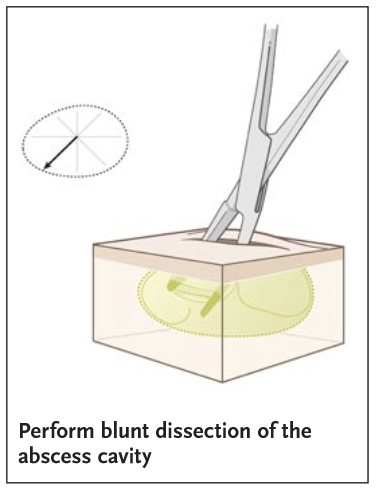
4. Use curved hemostats for further blunt dissection to break loculations and to allow the abscess cavity to be opened completely. Insert a curved hemostat into the wound until you feel the resistance of healthy tissue, then open the hemostat to perform blunt dissection of the internal portion of the abscess cavity. Continue to break up loculations in a circular motion until the entire abscess cavity has been explored.
5. Gently irrigate the wound with normal saline, using a syringe with splash shield or a needleless, 18-gauge angiocatheter, to reach the interior of the abscess cavity. Continue irrigation until the effluent is clear.

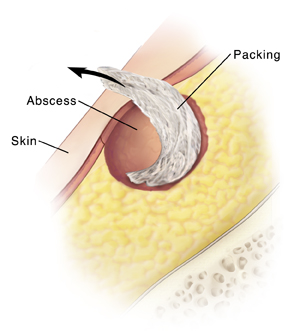
7. Cover the abscess wound with a sterile, nonadherent dressing.
Summary of Steps: