Description #
The use of bedside ultrasound by clinicians to guide invasive emergency procedures has been proven to improve success and reduce complications, and is rapidly becoming established as the standard of care.
UGEMP-Advanced provides an opportunity for physicians to acquire and maintain the skills required to perform the following procedures using Ultrasound-guidance:
1. Abcess drainage
2. Subcutaneous Foreign Body localization and removal
3. Arthrocentesis
4. Lumbar Puncture
5. Paracentesis
Learning Objectives #
At the end of the course, the student should be able to know the cognitive aspects and perform the psychomotor aspects of these procedures with the use of ultrasound guidance:
1. Abcess drainage
2. Subcutaneous Foreign Body localization and removal
3. Arthrocentesis
4. Lumbar Puncture
5. Paracentesis
Abscess drain #
Ultrasound Guided Abscess diagnosis and drainage
Abscess and cellulitis are two of the most frequently-encountered soft-tissue infections seen in the emergency department. It may be difficult to differentiate cellulitis from an abscess based purely on clinical signs. Both may present with warmth, tenderness, erythema, and swelling. An abscess and cellulitis can occur concomitantly. Fortunately, they have different ultrasound characteristics.

Is this a drainable abscess or severe cellulitis ?
Treatments – Abscess is treated with incision and drainage and may or may not require antibiotics, while cellulitis is treated with antibiotics alone
Ultrasound can also help to guide the treatment of an abscess based on its location, depth and size.
The common features to help distinguish an abscess on ultrasound are:
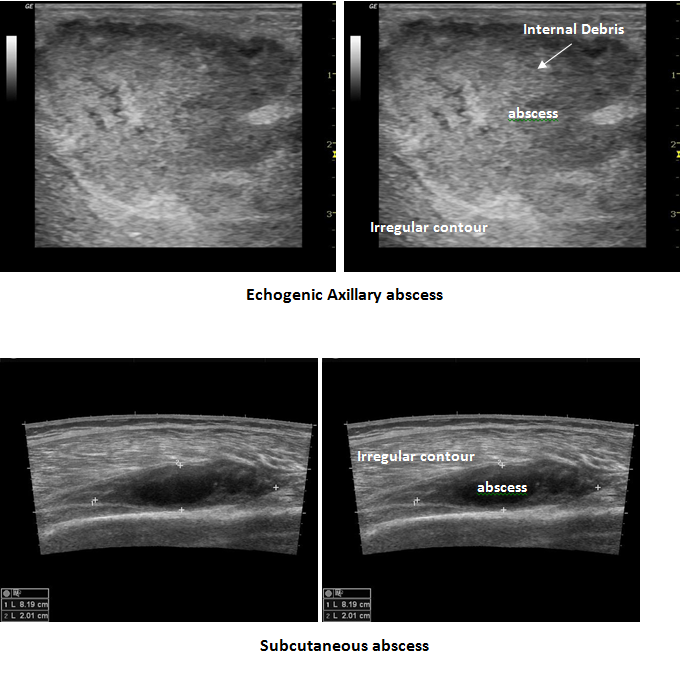
- spherical to oblong in shape ( depending on surrounding structures )
- Presence of an echogenic rim representing cellulitic soft tissue surrounding the abscess
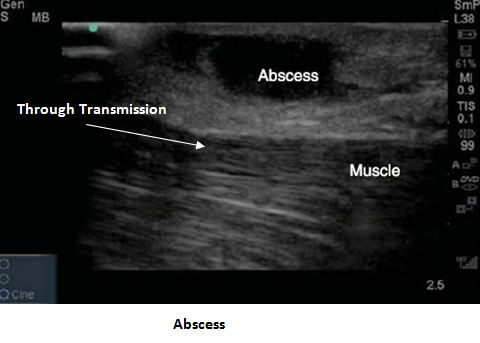
- primarily anechoic / hypoechoic
- will most often contain internal echoes corresponding to debris ( this can be used to differentiate an abscess from a simple cyst which will not have any internal echoes within it )
- posterior acoustic enhancement ( indicative of a fluid-filled structure on ultrasound )
- “Squish-Sign” with compression – if the abscess is superficial enough, you will be able to ‘agitate’ or disturb the internal debris with the application of a small amount of probe pressure.
- a solid abscess may not have posterior enhancement but will have mass-effect on surrounding structures
Setup
The US Machine is positioned so that the operator does not have to turn head away from patient:

– use linear probe on high-frequency setting for superficial structures
– If a deep abscess is suspected, the curvilinear probe ( which has a lower frequency) may be required to
penetrate and visualize the deeper structures.
Due to presence of possible infection, a probe cover is recommended prior to scanning.
If performing needle drainage, first identify the largest pocket of pus and mark the skin using a marker or needle cap.
If performing Incision & Drain, draw a line on skin over the largest collection of pus as a guide
Multiple abscesses in same relative location
ensure scanning of entire area to assess for multiple collections
If you are unsure of what the ‘normal’ area should look like, scan either a few cm away from the site, or scan the contra-lateral side of the patient
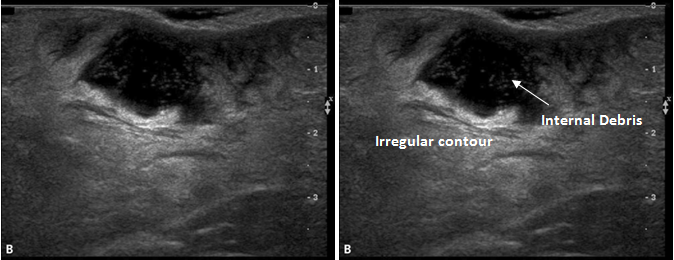
Note the internal debris within the abscess collection
Superficial Abscess
Technique
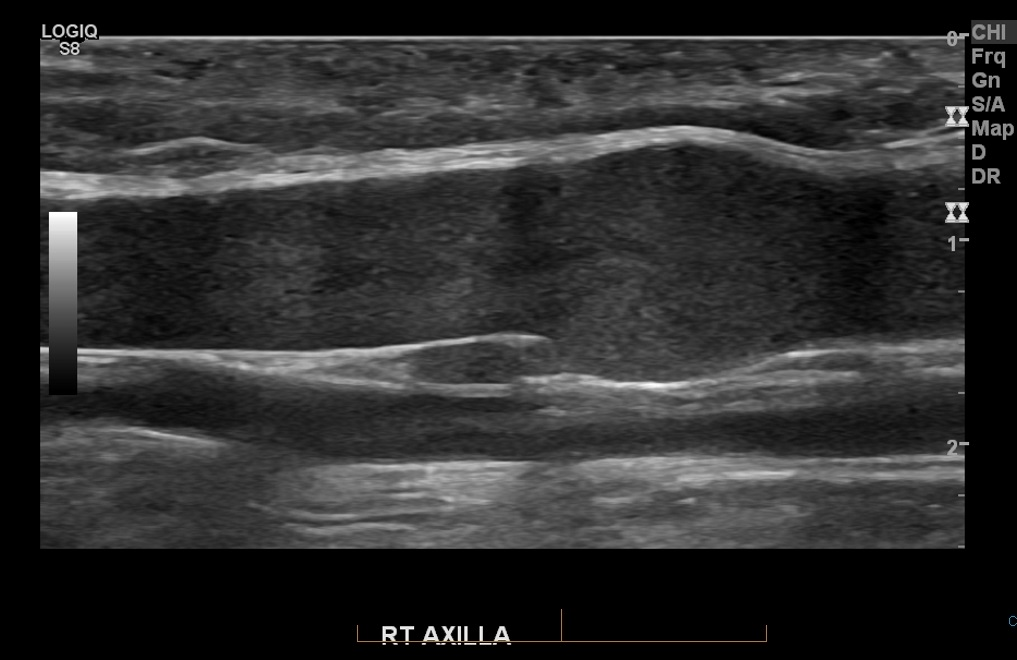
Ensure that you assess the abscess in two planes, in order to be able to confidently define the margins. This will also prevent you from attempting to drain a fluid collection that might not be an abscess
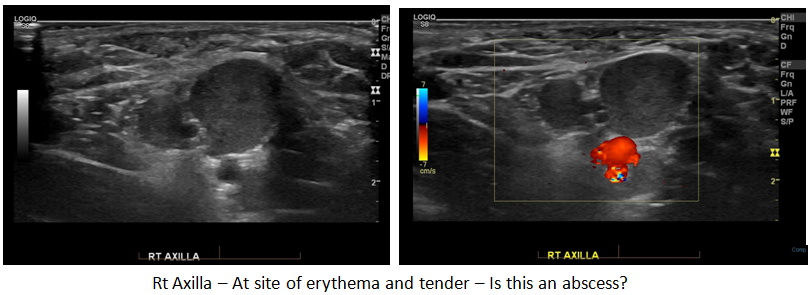
A 900 rotation of the probe reveals this possible abscess to be the axillary vein. The lack of colour response with the Doppler was due to the very sluggish flow within the vessel – There was some swirling visible within at this site, but the velocity was too slow for the machine to register the flow
Cellulitis
Ultrasound can help to determine presence of abscess versus simple cellulitis
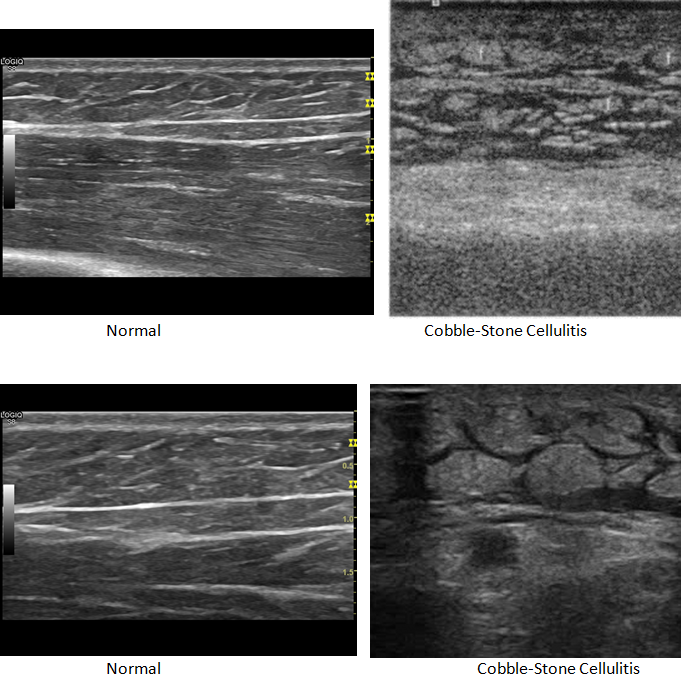
Cellulitis is defined as ‘inflammation of connective tissue with severe inflammation of dermal and subcutaneous layers of the skin’, and in most instances, is caused by staphylococcus aureus or streptococcus pyogenes. Depending on the severity, the amount of swelling ( due to edema ) may be visible on ultrasound, aiding in the diagnosis of cellulitis. If the edema is severe-enough, the ultrasound images will take on a ‘cobble-stone’ appearance.
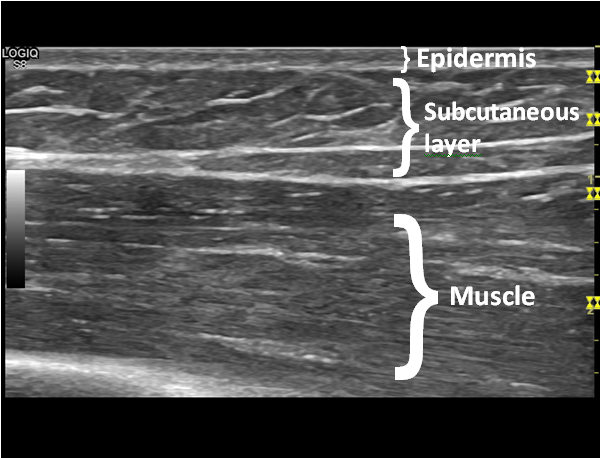
This is the normal appearance of the subcutaneous layer and underlying muscle layer.
Ultrasound can help to direct whether needle drainage or I & D should be performed
Squire et al demonstrated that ultrasound is 98%sensitve and 88% specific for diagnosis of abscess ( compared to 86% sensitive and 70% specific without imaging guidance )
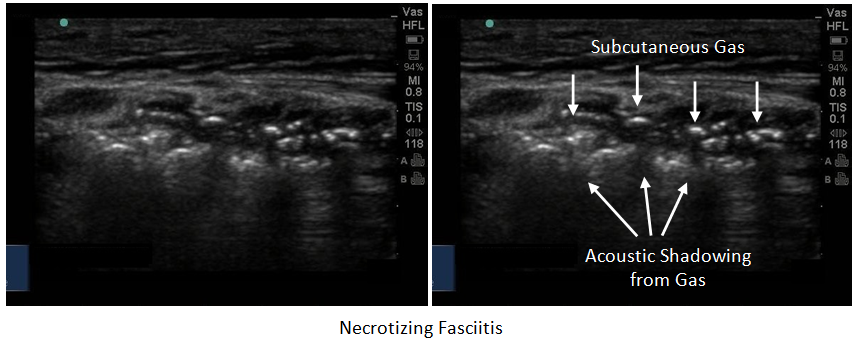
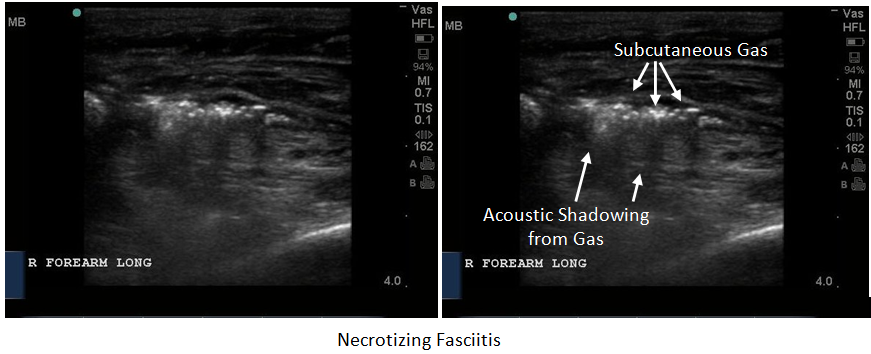
Necrotizing Fasciitis
Necrotizing Fasciitis is a rapidly progressing, life-threatening infection. It is rare and typically diagnosed by the speed of its progression. This infection will involve the subcutaneous tissues and fascia, and potentially the underlying muscle groups. Yen and colleagues found that ultrasound has high sensitivity and specificity ( 88% and 93%, respectively)1.
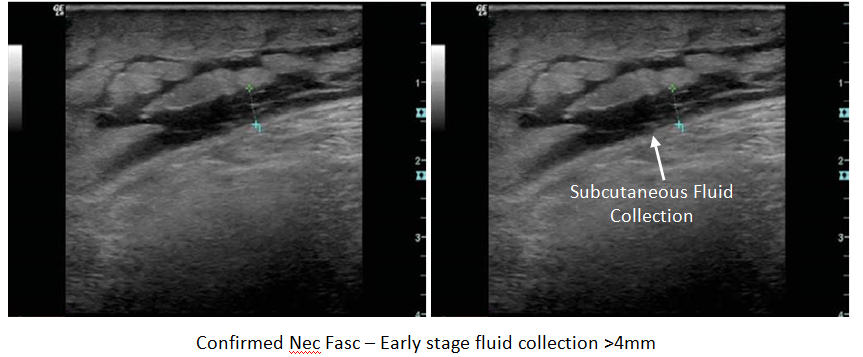
In the early stages of necrotizing fasciitis, the ultrasound images are similar to cellulitis, but a fluid layer in the deeper fascial plane which measures >4mm has been regarded has highly sensitive and specific for the diagnosis of necrotising fasciitis. As the infection progresses, gas formation ( gas gangrene) will become visible in the soft tissues. Gas will appear as bright, echogenic foci scattered throughout the soft-tissues at the infection site.
References
Yen et al. Ultrasonographic Screening of Clinically-suspected Necrotizing Fasciitis. Acad Emerg Med. Dec 2002., Vol 9, No. 12. 1448-1451
Mulcahy H, Richardson ML. Imaging of necrotizing fasciitis: self-assessment module. AJR Am J Roentgenol. 2010;195 (6): S66-9
Chao HC, Lin SJ, Huang, YC, Lin, Ty
Sonographic Evaluation of cellulitis in Children. J Ultasound Med; 2000: 29(11). P743-749
Squire, BT et al. ABSCESS: Applied Bedside Sonography for Convenient Evaluation of Superficial Soft Tissue Infection. Acad Emerg Med 2005; 12(7); p601-6
Chau, C; Griffith, J. Musculoskeleteal Infection: Ultrasound Appearance. Clin Radiol. 2005; 60(2). P149-59
Valle, M; Zamorini, M.
Skin and Subcutaneous Tissue. In: Blanchi S, Martilioni C, eds. Ultrasound of the Musculoskeletal System. Springer: Berlin 2007: 19-43
Gaspari, R, Davno, M, Briones, J, Blehar, D. Comparison of computerized tomography and ultrasound for diagnosing soft tissue abscesses. Crit Ultrasound J. 2012 Apr 17;4(1):5.
Crit Ultrasound J. 2012 Apr 17;4(1):5.
#
Reviews- Physics & Probes #
Introduction to Ultrasound Probes
The ‘art’ of ultrasound is a continuous trade-off between penetration and resolution. The probe can be good at either penetration or resolution, but not both at the same time. Some probes are good at only penetration ( can penetrate very deep into the patient, but resolution is compromised) or only resolution ( the quality of the image is vastly superior, but you are only able to look at very superficial structures ), and some probe walk the line between penetration and resolution by making some compromises to both.
The trick to remember with ultrasound is that you are using sound waves to generate an image. These ultrasound waves are measured in Mega-Hertz ( MHz), with a lower frequency ( 2-5MHz) having good penetration but less-than-ideal resolution. The higher-frequency probes (10-15MHz) have much better resolution, but due to the heightened frequency, are unable to penetrate as far into the body. A good analogy to the ultrasound probes is to think about those ‘pimped-out’ cars where you can hear the stereos from 3 blocks away.
If you think about it, you’re not hearing the full range of the stereo, you are only hearing the base ( low frequency). The lower the frequency, the farther the sound wave can travel. In order to hear the high-end of the stereo, you would actually have to be sitting in the vehicle. This is because high-frequency sound wave cannot travel as far as can lower frequency.
Low Frequency -> travel farther -> “sounds terrible” = decreased resolution
High Frequency -> shorter travel distance -> “clearer sound” = increased resolution
Curvilinear ( 2-5MHz)
This probe is the work-horse of ultrasound. It is a low frequency probe that results in a relatively good amount of penetration. Since the probe is curved, the beam ‘fans’ out through the body, to produce a wide field-of-view. As indicated, this will result in a relative loss of resolution. As the probe is quite large, it is not ideal for fitting into small areas ( such as intercostally for cardiac views )
Phased Array ( 2 – 5 MHz) ( AKA – Cardiac Probe )
This probe also uses a low frequency, but due to the smaller size of the probe-head ( read: smaller ‘foot-print”), it is more useful for fitting into tighter locations, such as intercoastal windows when assessing the heart. The name is derived from the way the computer activates the crystals in the probe – it occurs through “sequential phasing”. Due to the way the crystals are arranged in the probe head, the ‘near field’ is quite small.
Orientation Markers
Every probe in the world will have and indicator marker on them. This marker will ALWAYS be directed towards the patients HEAD (when the probe is in a longidutinal orientation) OR towards the patients RIGHT (when rotated into a transverse orientation ). This marker corresponds to the indicator marker on the screen. If the probe is every orientated the other way, the image will be ‘backwards’ to convention. The probe marker will also become of critical importance in procedures as the needle will be advanced on the same side of the marker, and will therefore always enter from the left side