Description #
This unit is designed to help the interdisciplinary team develop a better understanding of the skills involved in performing the technique of assisted cough. It will also provide an understanding of the clinical reasoning process behind the application of assisted cough. At the end of this unit the subject will have an understanding of the clinical reasoning, contraindications/restrictions, and proper application of assisted cough.
Learning Objectives #
At the completion of this unit the student will be able to:
- Know the components of a cough.
- Know the innervations of the muscles of Inspiration and expiration.
- Know the indications for an assisted cough.
- Know the contraindications and precautions for performing an assisted cough.
- Understand the concept of augmenting inspiration.
- Know how to safely apply assisted cough as a treatment technique.
Introduction to Assisted Cough #
What is a cough?
A cough involves a deep inspiratory breath followed by forced expiration–initially with a closed glottis which then opens to allow for rapid expiratory airflow (Morice, 2008).
For a physically intact adult peak expiratory flows normally reach 7 to 12 L/Sec (Bach 1993).
What is an assisted cough?
A manual assisted cough involves the manual application of abdominal pressure and/or costal lateral compression using various hand placements on expiration to augment the patient’s voluntary cough effort.
An assisted cough can increase peak expiratory flow rates by up to seven fold. (Harvey 2008)
Theory of assisted cough #
What is a deep breath?
We measure Forced Vital Capacity often referred to as the VC to determine a person’s capacity for a deep breath.
A forced vital capacity is the measure of the air forced out by the client after a maximal inspiration.
A figure of 15mls/kg is used as an indicator of when to consider ventilator support.
Consider the relationship of the level of injury to the spinal cord with respect to respiratory dysfunction as reflected in the vital capacity.
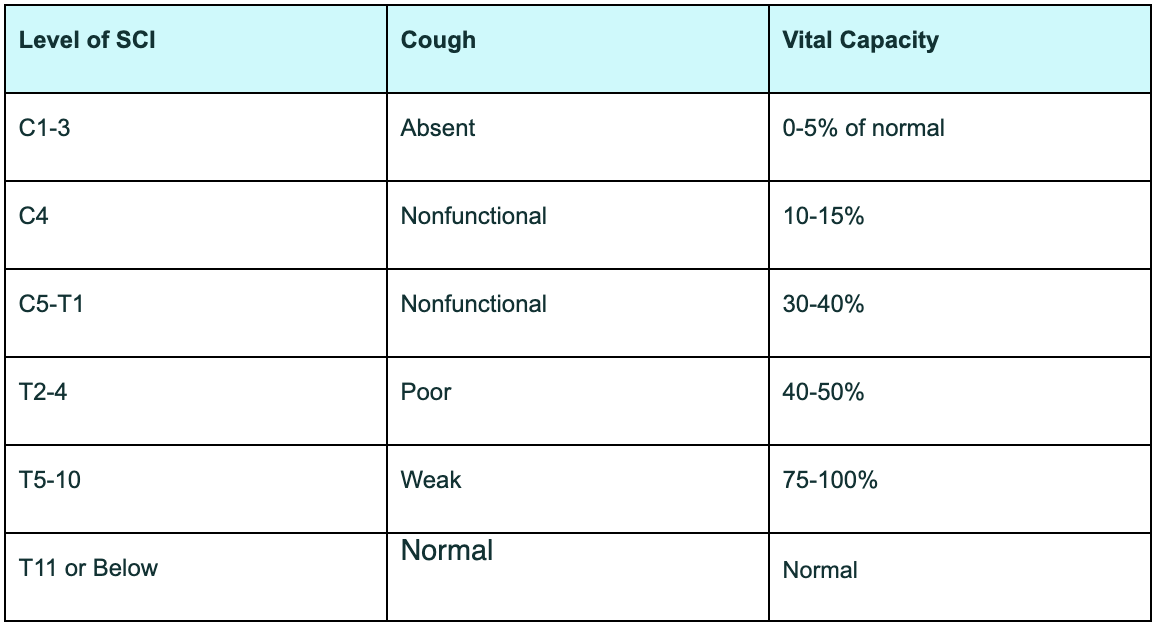
This indicates how important it is to consider supplementing the inspiration along with providing physical assistance with the expiration.
How can we supplement inspiration?
MHI: manual hyperinflation using a manual ventilation unit (MVU) or resuscitation bag.
IPPB: Intermittent positive pressure breathing.
Volume ventilator: increase the volumes during the treatment time
Breath stacking: the client takes a deep breath and holds it and then stacking another breath on top using a Resuscitation bag.
GPS: Glossopharageal breathing is a technique of breathing which consists of a stroke-like action of the tongue along with constricting action of the pharynx pumping air through the larynx into the lungs.
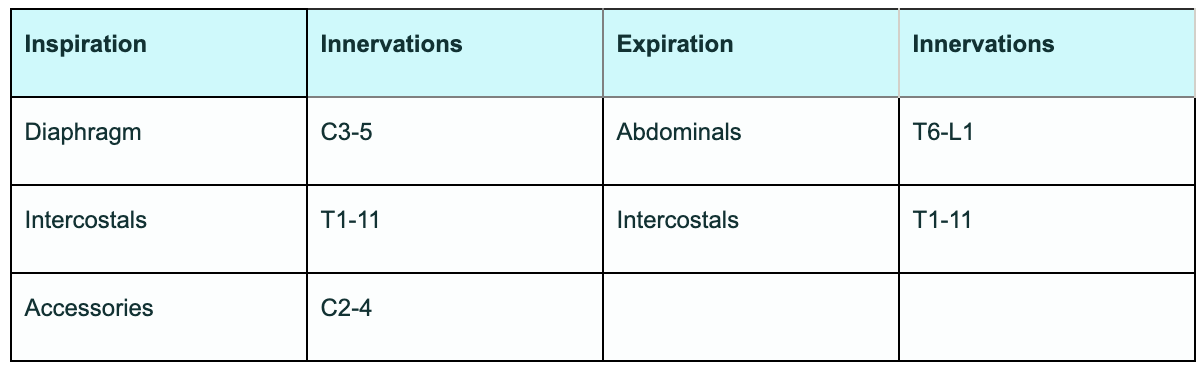
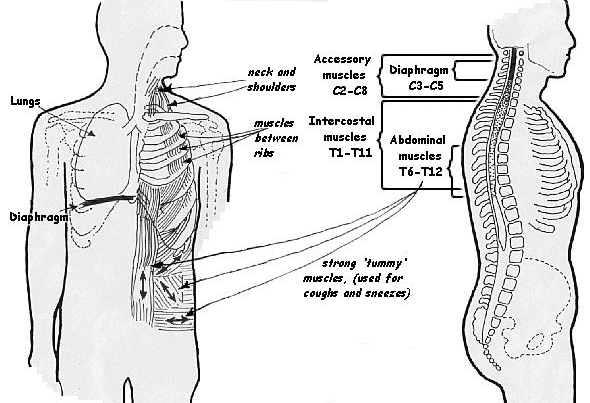
Innervation of muscles of inspiration and expiration #
What are the innervations of the muscles of Inspiration and expiration?
Indication for an assisted cough #
When is assisted cough indicated?
An assisted cough is indicated when the client is unable to effectively clear secretions through a normal cough mechanism due to neurological impairment leading to the expiratory muscles’ inability to generate sufficient expiratory flow rate. E.g. Spinal cord injury, ALS, Neuromuscular dystrophy, Post-poliomyelitis, etc.
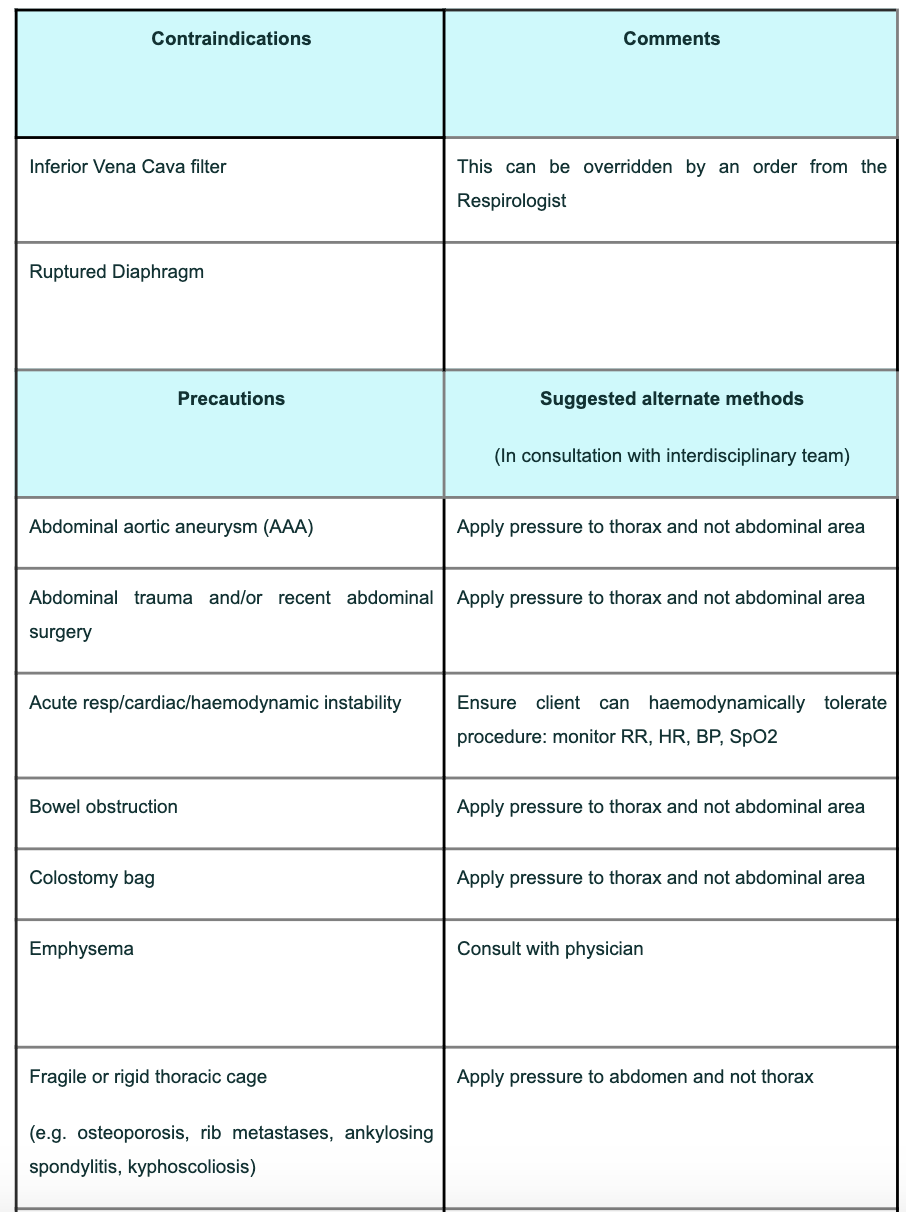
Contraindications and precautions for an assisted cough #
What are the contraindications and precautions for an assisted cough technique
Initial and ongoing assessment #
Initial and ongoing assessment
Observation
- Breathing pattern -does the client have intercostal muscles function or is there a reciprocal breathing pattern whereby the ribs draw inward during inspiration
- Work of breathing -does it look like the client is working hard to breath using their accessory muscles too fast or too slow
- Colour, amount and consistency of sputum -if it is green, yellow thick smelly and tenacious is an indication of infection
- Pallor – looking white may be an indication of hypotension
- Level of alertness – if the client is less alert is this due to medication, oxygenation or other factors
Objective findings
- Assess degree of use of intercostal muscles. Place your hand over the upper intercostal muscles and palpate during breathing you should feel tone in the muscles during a deep breath. If there is no tone and/or in-drawing noted between the ribs then there is no upper intercostal function. Palpate over the lower intercostals the degree of lateral expansion during a deep breath there may be varying levels of function and there may be asymetry noted.
- Assess degree of use of diaphragm, with the client in supine palpate under the anterior rib cage you should feel the diaphragm descend into your fingers. One side may be stronger than the other
- Assess degree of use of the accessory muscles. Palpate over the sternocleidomastoid, scalene and levator scapular muscles they should be at rest during quiet breathing.
- Determine flexibility of ribcage by applying gentle overpressure during expiration. If the client’s ribcage is rigid then consider hand placement for assisted cough would be more effective over the abdomen.
- During palpation you may also feel obvious secretions fremitus
- Auscultation may be used to determine the location of secretions and/or associated collapse. This information will help determine what position to put the client in, to obtain the best results. e.g. If you combine treatments such as postural drainage and manual hyperinflation then position the affected lung up
- Oxygen saturation (SpO2) -normal range 92-100
- Arterial blood gas (ABG) -pH 7.35-7.45/ PaCO2 35-45 / PaO2 >80 / HCO3 22-28 / BE-2 to +2
- Respiratory rate (RR) -normal 12-16
- Vital capacity (VC) 3-5 Litres or 45-65ml/kg
- Neurological motorsensory assessment to determine innervations and activation of inspiratory and expiratory muscles.
- Oxygen requirements (FiO2) to maintain SpO2 >92
- Any condition identified in contraindications and precautions
Monitoring requirements as necessary
- SpO2 – If SpO2 remain above 92 it is a good indication that the procedure is well tolerated from an oxygen requirement perspective. If the SpO2 drops below 92 it may be the airway is compromised by a plug or from prolonged suctioning
- End tidal carbon dioxide (ETCO2) is an indication of overall ventilation. Normal = 35-40mmHg typically too high indicates hypoventilation, too low indicates hyperventilation.
- Electrocardiogram (ECG) Arrhythmia indicated the client is not tolerating the procedure
- Heart rate (HR) normal 60-100bpm may be low in the quadriplegic population once out of neurogenic shock
- blood pressure (BP) normal = 100-140/50-90mmHg
How to perform an assisted cough #
How do you perform an assisted cough?
1. Preparation:
Wash hands don protective equipment
2. Consent:
Explain the procedure to the client and obtain consent
3. Position the client:
The client may be supine, side lying or sitting. This depends upon your clinical reasoning and the circumstances. Is this assisted cough needed immediately when the client is in their chair or is it a part of a respiratory treatment session? If the client is in a wheelchair can it be tilted back and up against a wall to reduce bouncing of the chair?
4. Landmark:
Abdomen: place hand above the umbilicus and at least 2 inches below the xiphoid.
Chest wall: place palm in contact with the upper and/or lower ribs.
Palpate breathing pattern and co-ordinate with client and/or secondary caregiver on timing breathing with the cough. The client will promote synchronicity with inspiration, expiration and cough.
5. Body mechanics:
Position the wrists in neutral, elbows straight but not locked, shoulders relaxed and not internally rotated, shoulders square to hips, legs in a lunge position to ensure a weight shift.
6. Hand position options:
One person –one hand on abdomen, one hand on upper or lower ribs
One clinician – both hands on chest wall only
One clinician – both hands on abdomen only
One clinician – forearm/s on Abdomen and /or Chest wall or one on each
Two clinicians – Lower hands (hand over hand or side by side) on abdomen; upper hands on ribs
Two clinicians – Any combination of the one clinician techniques
Two clinicians – May be Chest wall only or Abdomen only
7. Timing and coordination is critical to be effective:
Instruct re inspiration: Deep breath or supplemented deep breath
Coordinate timing of cough with the client’s respiratory pattern
Communicate with the client and any other clinician involved on which breath you assist the cough
8. Amount of force:
The constant manual pressure is applied as the patient starts to exhale.
Apply enough pressure to mimic muscle function for a cough to be effective without causing pain.
The duration of the pressure should be until the client starts to inhale again.
If the the pressure is too little the cough will be ineffective and there is a risk the client or caregiver will
fatigue and more attempts will be required to clear secretions.
If the pressure is too forceful, it may cause pain or trauma and the client might be reluctant to continue.
Ensure correct direction of force such that the client is not moving up toward the head of the bed.
9. Do not vibrate:
The force should be constant without vibration or shaking
You lose valuable force needed to create the expiratory flow for the cough
There is no therapeutic benefit to vibrating the abdomen
10. Dosage:
The number of assisted coughs required will be determined by several factors including:
The amount required to effectively clear the client’s secretions.
The clients fatigue level
11. Evaluation:
Ensure you evaluate the effectiveness of the procedure along with the client’s ability to tolerate it:
Using SaO2, facial expression, verbal communication, work of breathing, auscultation,
and amount cleared, along with pre versus post assessment findings.
Ensure the client is comfortable. Remove protective equipment and wash hands
Hand placement options #
Hand placement options include:-
Thorax only:-
Both hands on one side of the rib cage pushing down into chest wall one over upper intercostals one hand over lower intercostals
Hands on either side of the rib cage pushing inward and downward towards each other
Forearms in contact with upper and lower chest wall (no picture)
One hand on either side of the rib cage i.e. front and back on one side (no picture)

Abdomen only:-
One hand over the other just above the umbilicus (no picture)
Hands side by side on the abdomen one or two person technique
One hand over the abdomen the other hand being used for something else e.g. stabilise the wheelchair
One forearm in contact with abdomen (no picture)
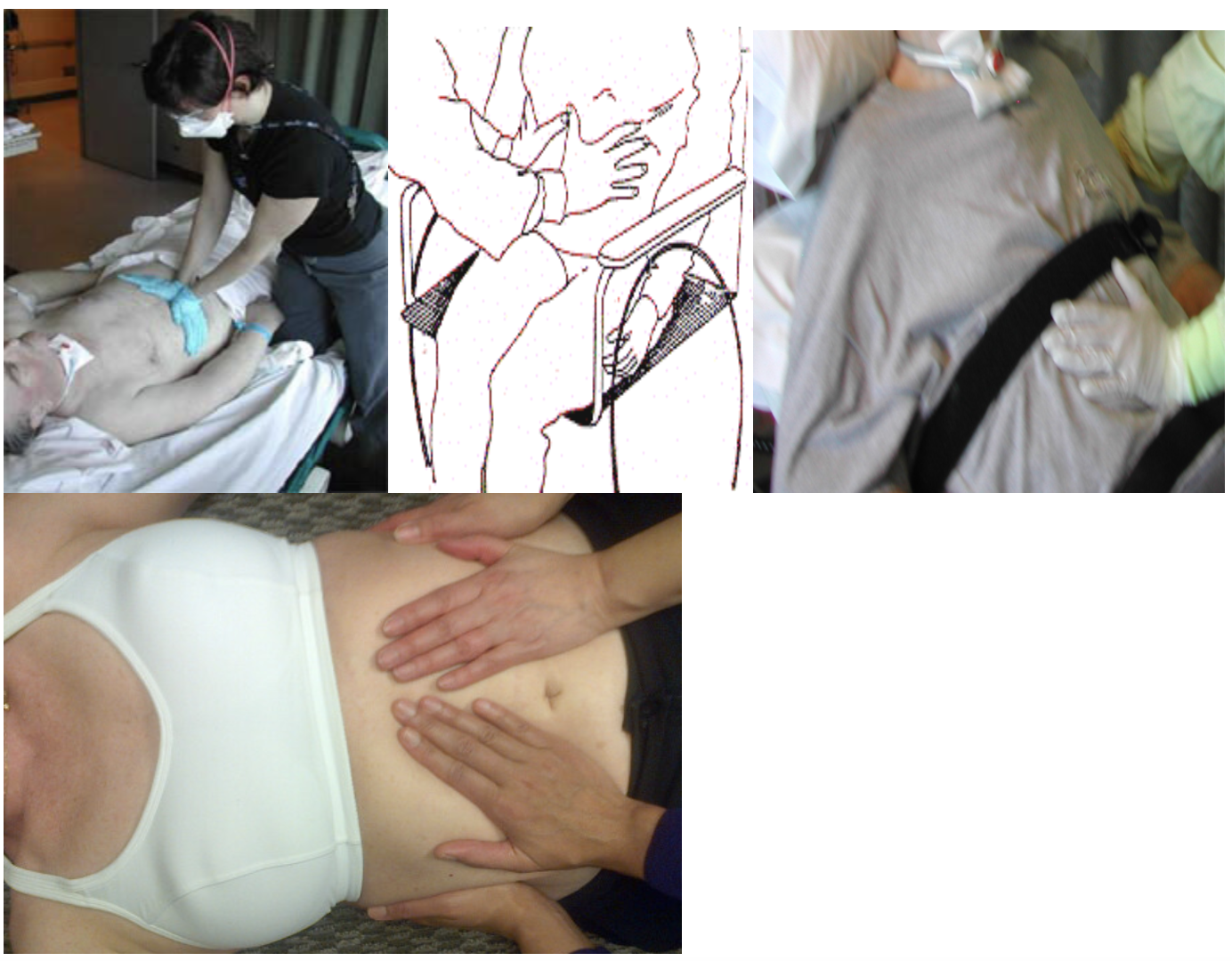
One on the thorax and one hand on the abdomen:-
Any combination can be used for both a one person and two person techniques
Remember to direction of force mimics muscle action bucket handle for chest wall and up and in for the abdomen.

photos_for_assisted_cough_hand_placement.doc
1 Person Chair #
Video demonstration of assisted cough on a client in a power wheelchair
This video demonstrates the one person technique on a client in a power wheelchair with one hand providing the assisted cough placed over the abdomen and the other hand stabilising the wheelchair.
2 Person Chair #
Video demonstration the 2 person assisted cough technique with a client in a wheelchair
2 person with client supine #
Video demonstrating a 2 person assisted cough technique with the client supine
This video demonstrates the abdominal and thoracic hand positions with a 2 person assisted cough technique
Notice the coordination between the therapists and with the client’s breathing pattern.
What NOT to do #
What not to do
Do not vibrate the abdomen during an assisted cough as shown in this video
Vibration is a separate therapy strategy that may be used prior to an assisted cough
Ventilated clients #
Ventilated Clients
Assisted cough may be performed on ventilated clients. Consider the following, as applicable:
Preoxygenation
Assess oxygen requirements and pre-oxygenate as necessary. Ensure oximetry is adequately monitored throughout procedure if the client has the potential to decompensate.
Inspiratory Volume Requirements
A deep inspiration improves the efficacy of the assisted cough maneuver. Assess the ability of the client to assist with a deep inspiration and/or provide pressure/volume assistance through the ventilator or manual ventilation unit (MVU) as required.
Humidification requirements
Ensure adequate humidification is being provided through the ventilation system in use. Meeting the client’s humidification requirements will help to thin the secretions and improve mucociliary clearance.
Alarms
If alarms are muted or silenced during the assisted cough procedure, ensure they are reactivated and appropriately set upon ventilator reconnection.
Independent Breathing Time
Assess client’s independent breathing time prior to the procedure to determine if manual ventilation is necessary if the ventilator becomes disconnected and whether the client can participate in the assisted cough maneuver.
Ventilator Disconnection
Determine if the ventilator is to be left connected during the procedure or if manual ventilation is more appropriate. This may be determined by suctioning and/or oxygenation requirements, adjunctive therapy, ventilator capability, alarm settings, or manual ventilation requirements. Consult Respiratory Therapist if unsure.
Emergency Equipment
Ensure emergency equipment is available for ventilated patients including MVU and airway equipment as needed.
Ventilator Monitoring
Ensure ventilator monitoring during and post-procedure. This includes checking alarms are active and appropriately set (alarm silence feature should be reset after assisted cough), pressures/volumes are compared to previous levels, artificial airway is in place and secure, tubing connections are secure, and all parameters have been reset to previous levels.
Interdisciplinary approach #
Interdisciplinary approach
The client is receiving optimal care when the team works together to achieve the desired outcome.
Communicate
Liaise with RT, RN, and PT to coordinate the timing of treatment when the team can be there to match when the client needs the care.
Coordinate
Treatment to be post-medication (pain, bronchodilators), at the time turns are happening staff are more available.
Combine techniques
To get the maximum outcome use your clinical reasoning to determine what combination of techniques are appropriate for your client. E.g. Postural drainage for secretions, intermittent positive pressure breathing (IPPB) or Manual ventilation unit (MVU) to increase inspiratory volume, using a 2 person assisted cough technique.
Share the Physical load
Rotate who performs the suctioning versus assisted cough versus IPPB or rotate which side of the bed you perform the technique.
Share the workload
If the client can be treated effectively by one person split the sessions up so as to not all treat one after the other but rather to meet the client’s needs over the course of the 24 hours.
Here is a 20 minute overview lecture of all the material covered. (optional)
Teaching others how to perform an assisted cough #
Assisted_Cough_Handout_for_Caregivers.doc
Please modify this document to suit your needs when education others how to perform an assisted cough
References #
References
- Morice, Alyn H (2008). Rebuttal: cough is an expiratory sound, Lung, Vol. 186, issue 1 Feb 2008, Pg 7-9
- Harvey, Lisa. Management of Spinal cord injury a guide for Physiotherapists. Churchilll Livingstone 2008
- Bach, John R. Smith, William, H. et all Airway secretion clearance by mechanical exsufflation for post poliomyelitis ventilator assisted individuals. Archives of Physical Medecine and Rehabilitation 1993:74: 170
- Pearl, J Ramirez AR (2001). Small Bowel Perforation after a Quad Cough Maneuver. J Trauma. Jul;51(1):162-3
- Assisted Cough CPD
- Home support
- PAGs