Description #
This unit provides students with small group, ‘hands on’ simulation of abdominal injuries and an opportunity to practice assessment and management skills outlined in the didactic material (see Unit I ” Trauma Evaluation and Management (TEAM)) under the direction of an instructor
Learning Objectives #
The students will be able to:
- Apply TEAM concepts in a simulated patient with abdominal injuries
- Describe the appropriate investigation of a stable patients with abdominal injury
- Describe the appropriate investigation of an unstable patients with abdominal injury
- Describe principles for operative and non-operative management of abdominal trauma.
Phase 2 #
Phase 2 – Secondary Survey
1. Parameters
- A – none
- M – marijuana + alcohol
- P – stab injury
- L – last ate 2 hours prior
- E – no information
- HEENT – normal
- C-spine – no deformity/pain
- Chest – good A/E bilaterally
- Abd – no distension / localized tenderness / no rebound tenderness / bowel sound present / NG aspiration clear / urine clear
- Pelvis – stable
- Extremities – no deformity / normal neurovascular
- Neuro – 5/5 motor / normal sensory
- Log roll – normal / rectal normal
- Skin – warm and perfused
- Blood work – Hb 161 / WBC 6.1 / PLT 344 / Na 142 / K 4 / Cl 105 / HCO3 24 / Cr 64 / Amylase 54 / Lactate 1.1
- Urine analysis – normal
Response to initial management
- Vital Signs – BP 115/60 / HR 80 sinus / RR 16 / BT 36.6 C / O2sat 98% / GCS 15
- Urine output – 80cc / 20 min
2. Required Participant Activities
- AMPLE history
- Through secondary exam(especially neurologic exam)
- Diagnostic adjuncts – CXR(rule/out free air) / ABG(for base excess) / Lab-work / NG(look for blood) / Foley catheter(monitor UO, Blood) / FAST / CT, DLP
- Frequent re-evaluation – suspect occult intra-abdominal injury / continue monitoring / look for deterioration
Review and interpret diagnostics
- no evidence of shock
- no acute abdomen
Re-evaluation
- potential occult abdominal injury
- delayed risk for tetanus
Plan/Disposition from ER
- continued monitoring
- T+S
- keep warm
- tetanus prophylaxis
- consult general surgeon
- several management options – admit and observe / local wound exploration & potential discharge / diagnostic laparoscopy / exploratory laparotomy
Communication
- Thirty-year-old male hemodynamically stable after 45 minutes
- Anterior abdominal stab wound likely needs admission for laparotomy or observation
Phase 3 #
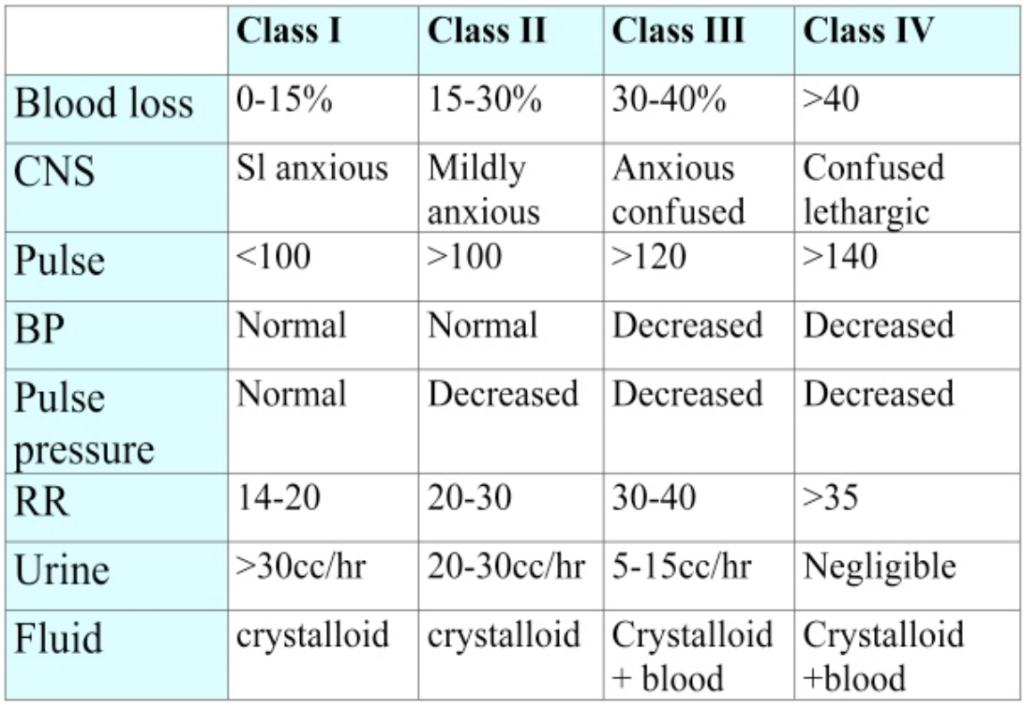
How do you classify depth of hemorrhagic shock?
Scenario Development Form #
Scenario Development Form
Please click on the link below to download the “Scenario Development Form” that can be used to prepare for the simulation sessions.