Description #
This unit will provide an overview of preoperative patient care, and will focus on patient assessment, the goals and modes of anesthesia delivery and the role of the licensed practical nurse in regards to when anesthesia is being delivery, anesthetic complications and cardiac arrest.
Learning Objectives #
At the end of the session the LPN will be able to:
- 1. Understand the important relationship between the registered nurse, the licensed practical nurse and the patient during the preoperive phase.
- 2. Understand what information is important to collect and assess during the patient check in.
- 3. Be familiar with the role of the LPN during delivery of all methods of anesthesia
- 4. Understand the role of the RN and the LPN for a patient experiencing anesthetic complications and cardiac arrest
Patient Check-in #
Nurse-Patient Relationship #
One of the most important responsibilities of the perioperative nurse is the preoperative patient check-in. To the untrained observer, this interaction could be mistaken for merely a detached verification process; however, the preoperative patient check-in. is often the only chance the nurse has to develop the rapport necessary to support the patient at possibly the most stressful time of their surgical experience. The perioperative nurse takes this opportunity to identify and understand the patient’s unique needs and to collaborate with the patient and the appropriate health care personnel in planning the care to meet those needs. This nurse-patient relationship is shaped by power, trust, respect and intimacy.
Power #
The perioperative nurse has a professional duty to regard the patient’s interests and well being as paramount. Therefore, it is essential that the perioperative nurse ascertains and upholds the patient’s wishes in regards to their surgical care and treatment. The nurse must make a conscious effort to develop a partnership role with the patient instead of an authoritative role.
Trust #
Upon entering the operating room, the patient places their absolute trust in the perioperative nurse. This element of trust is critical because the patient’s ability to make decisions and protect himself/herself is compromised by anesthesia and the surgery itself. The perioperative nurse serves as one of the patient’s advocate at this time, passing on the patient’s concerns to the surgical team and ensuring that the patient’s needs are met, safely and effectively.
Trust and confidentially go hand-in-hand. The patient assumes that the nurse can be trusted to maintain confidences. The nurse will treat patient information as confidential and will only share information on a need to know basis with others involved in the delivery of care.
Respect #
The perioperative nurse should respect the patient and their decisions about health care. Part of respect is valuing the patient as an individual and maintaining their dignity. The nurse is accountable for ensuring that they promote and protect the patient’s interests irrespective of gender, age, culture, disability, socio-economical status, sexuality or religion.
Intimacy #
Intimacy refers not to the fact that the perioperative personnel are privy to intimate details about the patient, but rather to the ability of the perioperative nurse to establish a caring connection with their patients. The patient is often anxious regarding the impending surgery, worried about the result, and stressed about their lack of control over the situation. The perioperative nurse can promote psychological and physical comfort by communicating empathetically with the patient, listening attentively to the patient, being alert to the patient’s nonverbal cues, offering gentle assurance and therapeutic touch, and providing explanations to the patient. A therapeutic relationship between the nurse and the patient, not only fulfills the patient’s physical, psychosocial, and spiritual needs, but also contributes to the autonomy, professional satisfaction, and self-actualization of the nurse.
Preoperative Patient Care #
The perioperative nurse is responsible for the assessment and admission of the patient into the operating room. During the preoperative phase, the nurse forms a therapeutic relationship with the patient and gathers data to ensure that patient care will be delivered safely and effectively. Data is gathered from the chart, laboratory and test results, consults, history, preoperative/daycare nurse, family members, and other pertinent sources. The interview is usually done in the preoperative area; either with the patient sitting in a chair or lying on a stretcher – this will depend on your institution’s method of transporting the patient to the OR theater (i.e. walking or being pushed on a stretcher) or it will depend on the patient’s physical condition.
As mentioned in PNLPN001 (Decision Making in the Perioperative Setting unit) – the patient assessment is done in collaboration with a registered nurse. Although the initial assessment is usually done by the registered nurse; a determination of patient complexity will be made and in some institutions, this level of complexity will be the determining factor as to who will do the final check-in procedure (outlined below) and/or transport the patient into the operating room theater. It is also necessary to recognize that there is no such thing as “routine surgery” – it all lies in the patient assessment (i.e. medical history, emergent situations); as this is done by a registered nurse – any participation in the check-in procedure will be an assigned duty (see the CRNBC Practice Standard: Assignment Between Nurses for further information). Any pertinent information gathered during the assessment will be relayed to the LPN and a collaborative plan of nursing care will be developed by all individuals involved with the surgical procedure.
Patient Check-In #
Often the patient assessment is done at the same time as the patient check-in; this is ideal as it allows for the patient to develop a bond with a consistent individual and is the most efficient process. However, there are times when the registered nurse will do the assessment prior to the surgical procedure start, and another nurse will do the check-in process. This is basically a verification process with the patient and a chart review to determine that all necessary information is present.
The following video is in two parts. Part one outlines the necessary information to be obtained during the patient check-in. Part two is a demonstration of a registered nurse checking in a patient prior to surgery. Watch how efficiently this check-in/interview can be done when the nurse is organized and knows exactly what questions are necessary to ask:
Anesthesia #
Learning Objectives #
At the end of the unit the student will be able to:
- Describe the three phases of a general anesthetic and relevant nursing implications
- Describe the routine monitoring equipment used on a patient undergoing an anesthetic
- Understand the effects of specific medications preoperative medications
- Recognize specific intubation equipment and their purpose
- Describe regional anesthetic, insertion technique, potential complications and nursing responsibilities: epidural & spinal
- List & describe other methods of regional anesthesia: various nerve blocks and local infiltration
- Discuss the following anesthetic complications and their negative effects on the patient: postoperative hypothermia, malignant hyperthermia, laryngospasm, pseudocholinesterase deficiency, and hypovolemia
- Describe the role of the LPN during anesthetic emergencies
Anesthetic Monitoring Equipment #
Significant advances in patient monitoring and anesthetic equipment have resulted in a decrease in risk to the surgical patient. The responsibility for this equipment lies with the anesthesiologist, however, the perioperative nurse must be familiar with the components and types of equipment, in order to assist the anesthesiologist to do their job.
A lot of mention will be made regarding the role of assisting the anesthesiologist, this infers a passive role, but it is just the opposite. The nurse who does the assisting is usually a registered nurse in the circulating role; their specialized practice includes the advanced assessment skills necessary to identify problems as they arise and the skills and scope of practice to manage routine and emergent occurrences. It may seem at times that assistance in the role of the LPN requires just standing by, but problems can arise at any moment and the anesthesiologist and registered nurse will depend on your skill set to assist in keeping the patient out of danger.
The best way to identify any change in status of the patient is through diligent monitoring of their hemodynamic state.
The different methods of monitoring a patient during surgery will be discussed (Review your textbook for further discussion). They types of monitoring devices will be divided into required (required by law for any patient undergoing an anesthetic) and specialized (used on a case or patient specific basis).
Required Monitoring Equipment #
Noninvasive Blood Pressure (NIBP)
- Preferably on arm contralateral to intravenous – BP tubing overlying brachial artery as marked on cuff, BP checked prior to induction. Avoid side with previous axillary node dissection.
- Cuff width should be 40% of circumference of extremity, bladder length encircle at least 80% of extremity. Cuffs come in a variety of sizes for the arm or thigh.
- Cuff reads falsely high if: cuff too narrow, too loose, extremity below heart level, uneven pressure
- Cuff reads falsely low if: cuff too large, extremity above heart level, quick deflation
- Artifacts caused by motion – shivering, surgeon bumping cuff, respiratory variation, kinking of tubing, loose connection or leak
- Taken every 5 minutes – may be more or less depending on patient or procedure
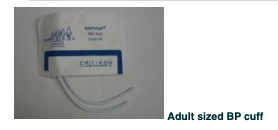
Electrocardiogram (ECG)
- Measures heart rate, rhythm, detects arrhythmias and ischemia, lead II is best for rhythm (provides the best view of the P wave).
- Three or five lead monitoring will be used – lead placement may be altered depending on the surgical incision site and patient position
- Artifacts caused by: incorrect calibration of ECG, inaccurate lead placement, poor connection, electrocautery, muscle artifact
Oxygen saturation monitor
- Pulse oximeter – measures pulse rate and oxygen saturation of hemoglobin – preferably on finger on side contralateral to BP cuff – may also use toe, ear, nasal septum, lip (different probes are available)
- Principle of measurement – uses waveform to differentiate pulsatile arterial blood from non-pulsatile venous blood, skin, muscle, bone, fingernails, and polish
- Measurement is by the absorption of light at two wavelengths, and depending on the amount of hemoglobin in oxygenated form compared to hemoglobin in reduced form (at < 90% there is less oxygenated hemoglobin readily available and SaO2 will drop quicker) – the SaO2% determined by ratio of light transmitted to photodetector
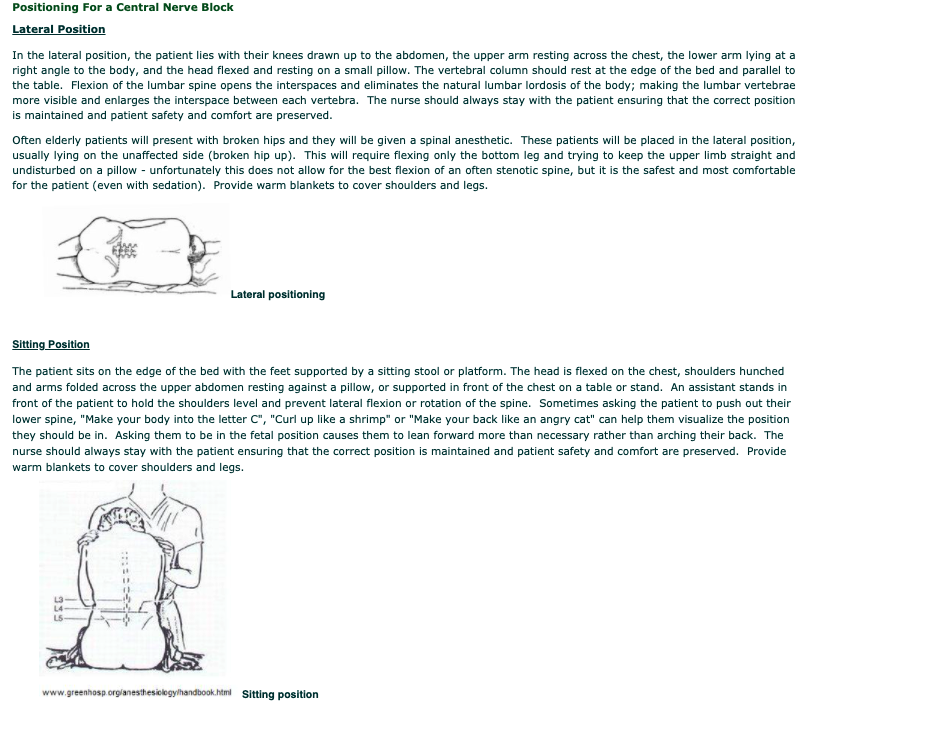
- Artifacts caused by abnormal hemoglobin, i.e. methemoglobin, carboxyhemoglobin, substance affecting absorption of light i.e. methylene blue, nail polish (blue, black, green), low flow conditions (hypothermia, vasoconstriction, hypotension), motion (shivering, agitation), ambient light
- Heart rate from electrocardiogram should be identical to heart rate from pulse oximeter to ensure oxygen saturation is accurate.
- Continuous measure of concentration of carbon dioxide, oxygen, and anesthetic gases in circuit – derives inspired and end tidal values of oxygen, CO2 (ETCO2), anesthetic gases
- Artifacts – may be obstructed by secretions or kinking of tubing
- – Water vapor may falsely elevate ETCO2
- – Nitrous oxide absorbs infrared, needs calibration
- – Lag time, the CO2 gas must travel from the patient to the monitor via long tubing
- – Air may be entrained, if there is a leak in the tubing, room air decreases the reading
- – Assume ventilation and perfusion matched to minimize gradient
- – Shallow breaths, prolongation of expiratory phase, uneven alveolar emptying
Suction
- Clean suction tubing and Yankauer tonsil suction tip present and functioning; liner requires a complete seal in suction container to fully function
Intravenous (IV)
- Adequate size intravenous (minimum size of 20 gauge is necessary for blood is to be given) that runs freely. If patient has difficult veins, a small bore IV may be started to administer the anesthetic, and then a larger bore IV will be inserted after the patient is anesthetized (veins become dilated and easier to locate under anesthetic and it is less painful for the patient).
- Depending on the procedure more than one IV may be started i.e. primary line and a larger bore IV for blood transfusion or fluid volume
- Required even if local anesthetic is given – to counteract any negative physiological effects quickly
- Warm IV fluids are administered or a fluid warmer is used
- Rapid IV transfusors can be used to give large volumes of fluid or blood products rapidly (1 unit of RBC/minute)
Stethoscope
- To check respiratory sounds after endotracheal intubation
- To assess heart function – automatic monitors can never replace physical assessment
Recommended to be Readily Available #
Temperature Probe
- Required to be readily available (in the OR theater) if the patient’s condition should change
- Oral or temperature probes
- Temperature above 35°C
- Use of forced air warming blankets (i.e. BairHugger, WarmTouch) – upper body, full body and lower body blankets available
- Preferable to warm upper body (and head) over lower body for more effective overall core temperature warming
- Do not place warming hose next to skin or under a flannel blanket, as skin burns may occur (especially on highest setting) – there must always be a layer between the patient’s skin and the warming hose – use of manufacturer blanket is recommended.

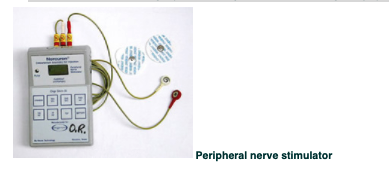
Peripheral Nerve Stimulator
- Not required but must be readily available, in order to assess the level of muscle relaxant still present in the body and therefore should be available, as muscle relaxation is used at some point for most surgeries. ECG patches are placed on the patient over muscle (temple or arm), stimulator cable attached to patches → small electrical current delivered to nerve, and degree or absence of twitch is measured
- If twitch prominent and surgery is still underway then more muscle relaxant will be given
- If twitch absent and surgery is finishing then a reversal agent (if possible) will be given
Specialized Monitoring #
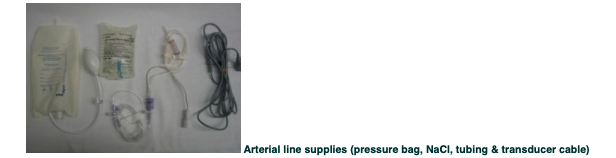
Invasive blood pressure (Arterial line)
- Purpose: allows beat to beat measurement of blood pressure and frequent arterial blood sampling. Arterial lines are used not only for patients with cardiovascular issues or for cases with suspected blood loss, but are also used in obese patients (BMI > 40) in which accurate BP readings with even a large BP cuff are less than optimal.
- Supplies required: single line transducer kit, heparinized saline (not at all institutions – some use plain saline), connector cable for anesthetic machine monitor, pressure bag, IV pole clamp
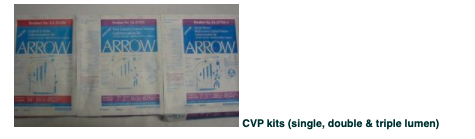
Central Venous Pressure (CVP) Line
- Purpose: accurate evaluation of hypovolemia or fluid overload, large bore IV access, ability to infuse inotropic and vasopressor drugs in larger doses
- Supplies required: saline, triple transducer kit, connector cable for anesthetic machine, IV pole clamp, central venous catheter kit (comes in single, double and triple lumen – be sure to clarify which one)
- Inserted in the trendelenburg position (head down) to increase visibility of veins (venous congestion) and reduce the risk of air emboli
Pulmonary Artery Catheter (Swan Ganz)
- Purpose: monitors pulmonary artery pressure and gives indication of intravascular hemodynamics
- It is used infrequently, usually only in ICU patients coming to the operating room and or cardiac surgery or liver transplant patients
- Supplies required: as for CVP, Swan Ganz catheter, larger bore introducer kit
Urinary Catheter
- Used for accurate fluid balance
- Urine output should be monitored for lengthy procedures (>2-3hrs) or for specific patient populations
- Urometer collection bags are best for accurate monitoring
Sequential Compression Device (SCD)
- Although not a piece of monitoring equipment, it is a useful means of preventing venous stasis → DVT formation and pulmonary emboli
- Risk factors: surgeries > 2 hours; age over 40; obesity; malignancy; prior history of varicose veins or pulmonary emboli; thrombophylic states; type of anesthesia; pre and postoperative mobility; level of hydration; presence of sepsis
- Contraindications: severe arterial disease of the lower extremities; dermatitis; gangrene; recent skin graft
- Thigh or knee length compression sleeves – even more effective when used in conjunction with compression stockings (TED)
- Used in procedures > 1hr (may be hospital specific, as a form of anticoagulant therapy may be used instead or in conjunction with SCD use)
Other
- Fetal monitor for obstetrical patients
- BIS® monitoring – a specially designed machine that monitors the depth of anesthesia; allows for accurate predication or timing of return to consciousness
- Doppler ultrasound – to check for air embolus – also used during vascular surgery to check patency of vessels
- Transesophageal echocardiogram (TEE probe) – used to check heart valve function during trauma or open heart surgery
- Ultrasound machine – used to accurately locate difficult veins for IV or CVP placement, arteries for arterial puncture and for nerve blocks – avoid multiple punctures
Nursing Responsibilities Regarding Patient Monitoring #
Preparation of the Patient for Anesthesia #
The word anesthesia is derived from a Greek word meaning “no sensation”. Today anesthesia can be described as a state in which the feelings of pain and other sensations are blocked. It can also be described as a ‘reversible lack of awareness’ this can be a total lack of awareness (as in a general anesthetic) or a lack of awareness of a part of the body (as in a spinal anesthetic or nerve block).
Every patient about to receive an anesthetic, in whatever form that may be, will undergo a preoperative assessment – this assessment is done by the anesthesiologist, and it reveals the patient’s history and risk factors regarding their airway management and surgical morbidity.
As most patients are now admitted the same day of surgery, preoperative clinic visits are an ideal way for the patient to have all appropriate tests completed and medications prescribed prior to showing up for surgery (ideally as close to the date of surgery as possible), so that they are in optimal condition to undergo the stress of a surgical procedure. These assessments or interviews are carried out in one of four ways:
- In a Pre-admission Clinic where lab tests, x-rays, physical exams and interviews are carried out by the anesthesiologist and a registered nurse.
- A telephone interview is carried out by a registered nurse to assess healthy, uncomplicated patients. If anything significant is determined from the interview the patient may be asked to visit the clinic.
- Often the anesthesiologist will receive a request for a consult and visit the patient on the ward or emergency department. This may occur one day before the case or as a consult ordered by the surgeon asking for an anesthesiologist’s opinion about the patient’s suitability for receiving an anesthetic. Most hospital inpatients scheduled for elective surgery are consulted on the ward the evening prior to surgery.
- A patient may receive their preoperative assessment just prior to entering the operating room, in the preoperative waiting area – it is important not to transport the patient until the assessment has been made. . This is not ideal, but common for emergent surgeries (if a prior consult cannot be obtained). For these emergent type procedures – it is essential that the registered nurse do the entire patient check-in process.
The information provided by the patient’s history and physical examination and the patient’s wishes will determine what type of anesthetic the patient will receive, how they will be monitored during the surgical procedure, how difficult their airway will be to establish and maintain, any other special risk factors, and any special needs/challenges the patient will present with.
Based on the patient information gathered in the preoperative visit, the anesthesiologist assigns the patient an American Society of Anesthesiologist’s (ASA) Physical Status Classification score between 1-5. These scores are defined as:
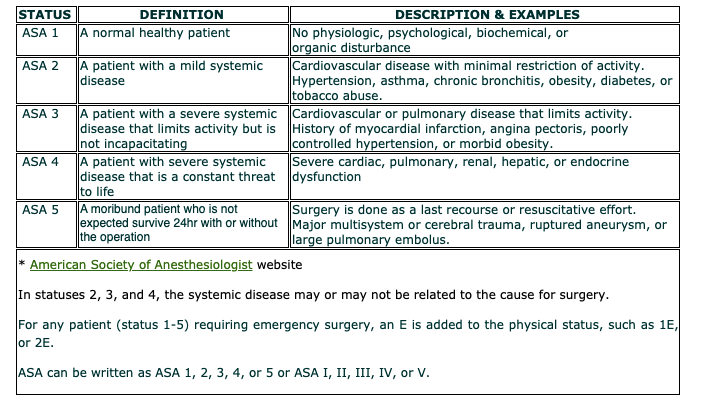
The Role of the LPN during General Anesthesia #
Role of the LPN during General Anesthesia #
As professionals, LPNs adhere to the Professional Standards of Practice. Your role during the administration of general anesthesia will depend on your profession’s scope of practice (the range of activities that your profession is authorized to perform based on educational preparation and certification).
General Anesthesia #
General anesthesia can be described as:
A reversible state of unconsciousness produced by drugs with sufficient depression of reflexes to allow a surgical procedure to be performed.
The anesthesiologist makes a decision about what kind of anesthetic and even what type of general anesthetic to give a patient based on:
- The goal of anesthesia
- The stage of anesthesia
- Requirement of surgery – length of surgery; need for muscle relaxation; significant blood loss expected; does the patient need to be aroused quickly after surgery (i.e. neurosurgery) to be assessed, etc.
- Unique requirements and characteristics of the patient – pre-existing medical conditions, trauma, age, personal preference etc.
Let us look at the first two more closely.
Goals of General Anesthesia #
The overall goals of anesthesia are:
- Unconsciousness, hypnosis and amnesia
- Patient will be unaware of environment during surgery and have no recall of intraoperative events
- Rapid onset, short duration drugs are used such as benzodiazepines (i.e. Midazolam), Propofol and barbiturates (rarely)
- Anesthetic gases such as Isoflurane, Sevoflurane and Desflurane
- Drugs used to produce unconsciousness have minimal if any analgesic properties
2. Analgesia – absence of painful perceptions
- Intraoperative pain control inhibits the stress response associated with the surgical procedure and will aid in postoperative recovery
- Potent short duration synthetic opioid agonists are used pre- and intraoperatively – i.e. Fentanyl, Sufentanil, Remifentanil
- Longer acting drugs such as Morphine, Hydromorphone and Fentanyl may be used towards the end of the procedure and in recovery for acute pain management
3. Muscle relaxation
- Used to facilitate airway intubation – use rapid onset muscle relaxants such as Succinylcholine and Rocuronium. The administration of Succinylcholine causes a few moments of generalized muscle fasciculations (patient will appear to be twitching) prior to the onset of muscle relaxation.
- Used to relax muscle tension around the operative site – depending on surgical procedure and site, they may not be needed – use longer acting drugs such as Vecuronium for the surgical procedures
4. Autonomic and endocrine reflex control
- Control of fight or flight response to the stress of surgery and to some of the secondary effects of the drugs used to induce anesthesia
- Control of autonomic and endocrine activity leads to an uneventful postoperative course
Stages of General Anesthesia #
The stages of general anesthesia should not be confused with the level of anesthesia. The level of anesthesia is outlined in your textbook as four stages in the level of consciousness (physiologic and reflex response) once anesthetic drugs are given. The stages of anesthesia refer to the whole anesthetic experience – the process by which a patient is prepared, given and awakened from an anesthetic. Although preoperative preparation is an important step, the stages of general anesthesia are considered to be:
- Induction
- Maintenance
- Emergence
Preoperative Preparation #
Preoperative preparation by the anesthesiologist was discussed previously. This discussion involves what happens to the patient just before and just after they enter the operating room theater. This preparation enables the patient to undergo the stress of surgery, decreases the risk of aspiration, controls any reflex activity prior to induction, provides analgesia and anxiety control.
With a registered nurse present at all times, the role of the LPN during preoperative preparation includes:
Induction #
Induction is the start of the general anesthetic to the fully anesthetized state (unconsciousness with sufficient depression of reflexes).
This phase of anesthesia places the patient in a potentially unstable condition and everyone attending to the patient must focus on the patient and be prepared for any untoward event.
It is desirable to reach unconsciousness as quickly as possible and so rapid onset short duration drugs (i.e. Propofol) are given to induce anesthesia in combination with a short acting opioid (i.e. Fentanyl or Sufentanil) to counteract any discomfort and related nervous system reflex activity.
Once the patient is unconscious it is necessary to manually assist with ventilation – the patient has an unprotected airway – once the patient is sufficiently preoxygenated and muscle relaxation is adequate, intubation occurs. If the procedure is of a short duration and the patient will be in the supine position, intubation may not be necessary and a laryngeal mask may be used. For longer procedures, a short to intermediate acting muscle relaxant (i.e. Rocuronium) is given to facilitate endotracheal intubation. Intubation should occur within 90 seconds of unconsciousness.
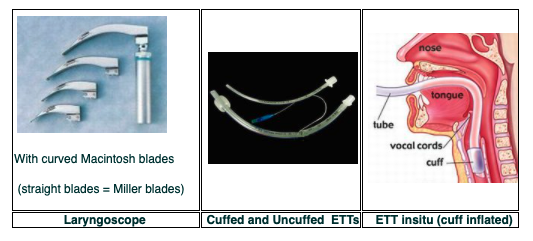
A laryngoscope is used to visualize the vocal cords. A topical local anesthetic (i.e. Lidocaine spray) may be applied to suppress any residual airway reflexes. The endotracheal tube is placed and attached to a mechanical ventilator and secured into place. Breath sounds are assessed with a stethoscope to ensure proper placement of the endotracheal tube (bilateral and equal breath sounds).
Emergence
Recovery from anesthesia is the second most important time for the patient. The overall goal is restoration of all vital functions to normal, including ventilation, airway reflexes and hemodynamic status. The patient progresses through four phases:
- Recovery of sensory and motor function as anesthesia depth is reduced – anesthetic gases and drugs are stopped or tapered off 30-40 minutes prior to the end of the surgical procedure (or before depending on their clearance time from the body) – which includes closure of the patient’s surgical wound. In the case of muscle relaxants, depending on which type was used, a reversal agent is given. To ensure ongoing analgesia postoperatively further opioids may be given, but adequate respiratory and hemodynamic function must be considered
- Resumption of spontaneous ventilatory control – reversal agents for opioids (Naloxone) or benzodiazepines (Flumazenil) may need to be given if awakening is prolonged
- Return of airway reflexes – sufficient muscle control is restored and attempts to breathe are made
- Awakening – patient opens their eyes and becomes increasingly aware of their surroundings
Tracheal extubation is the single most important event the patient will experience. If the patient does not have adequate control of their own airway or is not sufficiently awake to maintain their own airway prior to extubation, this can lead to emergency reintubation. Coughing should be avoided for certain procedures (i.e. ophthalmic) and so the patient may be kept in a deeper state to avoid reflex irritation – extubation will be attempted once the patient is more fully awake.
With a registered nurse present at all times, the role of the LPN during the emergence phase of anesthesia includes:

Intubation Techniques and Supplies #
Intubation refers to the placement of a tube into an orifice of the body, however, it is a term commonly used to refer to tracheal intubation. Tracheal intubation is the placement of a flexible plastic tube into the trachea. Reasons for tracheal intubation include:
- Apnea
- Respiratory failure
- Inability to protect airway (i.e. trauma, altered gag reflex)
- Altered level of consciousness
- Maintenance of patent airway
All of these reasons are applicable after the administration of a general anesthetic and muscle relaxants and therefore require some means of securing the patient’s airway.
Airway Anatomy #
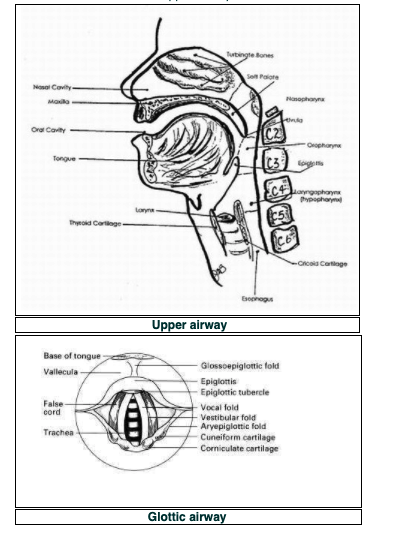
The upper airway is designed to deliver gases (O2 and CO2) to and from the lower airway (thoracic trachea, carina, mainstem bronchi and bronchioles) and onto the respiratory airway (respiratory bronchioles and alveoli of the lungs) for gas exchange. The upper airway can be divided into three sections:
- Supraglottic airway: nasal and oral pharynxes and the laryngeal pharynx. The soft palate separates the naso- and oropharynx (which includes the tongue, tonsils and pharyngeal muscles). The pharynx also includes the entrance to the esophagus.
- Glottic airway: laryngeal structures. The epiglottis is located at the top of the laryngeal cavity and during swallowing seals off the laryngeal inlet. The vocal cords (or ligaments) are within the laryngeal cavity and the opening between is the glottis. The glottis is the narrowest section of the adult upper airway. The larynx is protected by the thyroid and cricoid cartilages. The cricoid cartilage is the only complete circle of cartilage in the trachea; all the others are U-shaped.
- Subglottic Airway: cervical trachea. The larynx attaches to the cervical trachea (at the level of the 6th cervical vertebra). The subglottic area is about 10-15 cm to the carina (where the trachea bifurcates into the left and right mainstem bronchus). The subglottic trachea is the narrowest section of the upper airway in children.
The anesthesiologist can opt for a supraglottic airway (for short, simple procedures) or endotracheal intubation for procedures that are longer, more complex, or involve the patient to be in certain positions.
The most common supraglottic airway is the laryngeal mask airway (LMA) and the most common tracheal intubation is with an endotracheal tube (ETT).
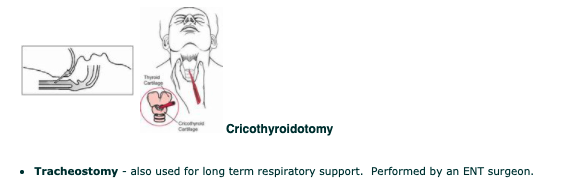
For emergency purposes, such as laryngotracheal injury, maxillofacial trauma, inability to open the mouth or unclench the teeth, or deformities that prevent orotracheal intubation, the following might be performed:
- Cricothyroidotomy – an opening is made between the cricoid and thyroid cartilages into the trachea. Some anesthesiologist always carry a large bore IV cannula and adapter “just in case”
Intubation #
The patient who is to undergo a general anesthetic has their airway assessed preoperatively by the anesthesiologist to determine how difficult it will be to see the glottic airway. To determine the degree of difficulty, the anesthesiologist will perform a number of assessment techniques (i.e. observation, asking the patient to open their mouth, etc).
Based on their findings and on the type of surgery the patient is to have, the anesthesiologist determines which method of airway control is required and by what means the airway can be placed quickly and accurately. The best determinant of airway access is by visual inspection via direct laryngoscopy, however this is not something one can do until the patient has been sedated (and a airway control has potentially be lost) and so the method by which airway control is gained can change rapidly.
The different methods used will be discussed below, in terms of how they are used and what the items used are, so as mentioned in the previous section (Role during General Anesthesia) you may be asked to retrieve these items while the anesthesiologist and registered nurse attend/monitor the patient.
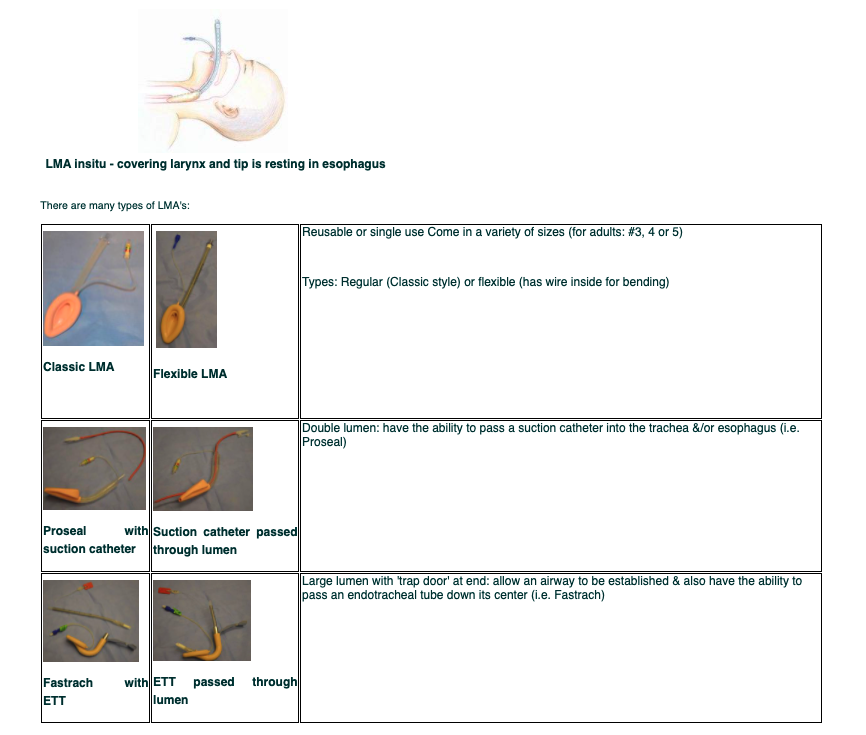
Supraglottic Airway #
The Laryngeal Mask Airway (LMA) is usually used for relatively short procedures and only for patients in the supine position and who are at a low risk for aspiration. LMA’s can be used for spontaneous (patient is sedated but breathing on their own) or mechanical ventilation.
It may also be used as a temporary measure to secure the airway until an ETT can be placed. LMA’s do not require a laryngoscope to put in place and they fit over top of the larynx. Since they are resting in the supraglottic area, behind the glottis (covering the larynx), they do not provide a sufficient seal against the regurgitation of stomach contents; therefore an LMA is not considered a secure airway (only a patent airway) and it’s use cannot be considered routine for shorter procedures (i.e. not for use in patients with reflux disease). It has a cuff and so a syringe is required as well to inflate it.
Direct Laryngoscopy #
This is achieved with the use of a laryngoscope (for visualization) and an endotracheal tube (ETT). The ETT comes in a variety of diameters, measured in French (Fr.) units.
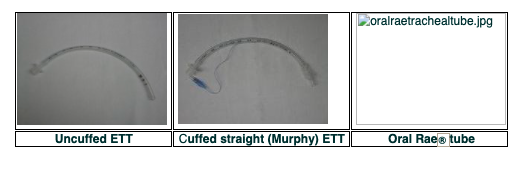
The tubes can be cuffed (with a balloon) or uncuffed. Cuffed tubes are used to seal off the airway from any aspirate – they provide a secure airway. Uncuffed tubes are only used in small children (the age is debatable, but usually 6 years old and under, depending on the size of the child) as their airway is so narrow it cannot accommodate the tube and a cuff and its resultant pressure.
Oral Tubes
The ETT is passed through the mouth, larynx, and vocal cords and into the trachea. A balloon, attached to the tube, is then inflated near the distal tip of the tube to help secure it in place and protect the airway from aspiration into the lungs of blood, vomit, and secretions (from esophageal regurgitation). The tube may be straight or angled downwards. Angled tubes are called oral Rae® tubes and are used for surgeries in the facial area (i.e. nose or ophthalmic procedures) – the angle keeps the ETT out of the way of the surgical area.
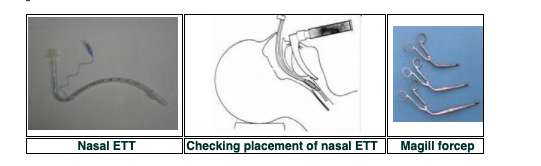
Nasal Tubes
Another means of tracheal intubation is passing a tube through the nose, into the oropharynx, larynx, vocal cords and then into the trachea. This method is used for surgeries in and around the mouth. They are often warmed to soften them and then passed through one of the nares (i.e. in a bottle of warm water/saline). The laryngoscope is placed orally and as the tube is passed and viewed in the oropharynx, a forcep (called a Magill) is used to advance the tube downward through the glottis.
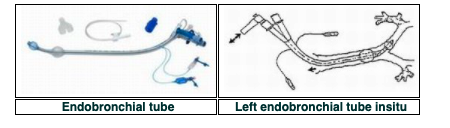
Endobronchial tubes
Endobronchial tubes are used for surgery of the lungs. They have two lumens – one sits in the trachea, above the carina, and the other sits in the right or left main stem bronchus. The tubes are designed for either the left main bronchus or the right main bronchus. Tubes come in sizes 26 to 41 French gauge (37-39 Fr. is the usual size for a female and 39-41 Fr. for a male).
After placement of an endobronchial tube, the anesthesiologist will place a flexible fiberoptic bronchoscope down the center of the tube to ensure it is sitting in the correct position in the bronchus.
Indirect Laryngoscopy #
Indirect laryngoscopy is achieved by the use of a lighted stylette. Lighted stylettes rely upon transillumination of the anterior neck tissues to demonstrate laryngeal placement. A well circumscribed glow indicates tracheal intubation, whereas a diffuse glow is seen with esophageal placement. A lighted stylette is used for:
- Patients with limited mouth opening or reduced neck movement
- Difficult intubations or failed intubation
- Bloodied airway
Contraindicated in patients with anatomic abnormalities of the upper airway or pharyngeal masses.
Advantages are that it is less stimulating than direct laryngoscopy, it does not require visualization of the larynx, can be done nasally and it is a portable and inexpensive device.
Disadvantages are that it is a blind technique, it is difficult to view the light in patients with dark skin or scarring, and it requires a darkened environment.
The ETT is placed over a stylette that has a light source attached. This stylette is placed into the mouth and advanced down into the oropharynx. The OR room lights are dimmed, as this will allow for the light to illuminate a pathway that can be seen through the patient’s skin. The anesthesiologist will go by feel and the location of the light (central on the neck over the trachea) to advance the stylette through the glottis and into the trachea. Once it feels like the stylette is in the right location, the ETT tube will be slide downwards off the stylette into position – the stylette is removed, leaving the ETT behind. The ETT cuff is inflated.

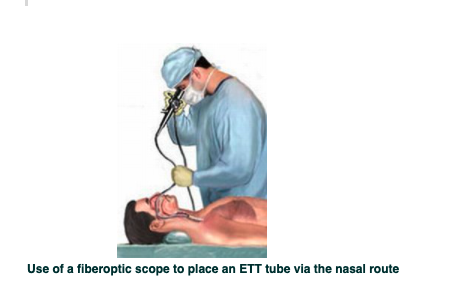
Fiberoptic Intubation #
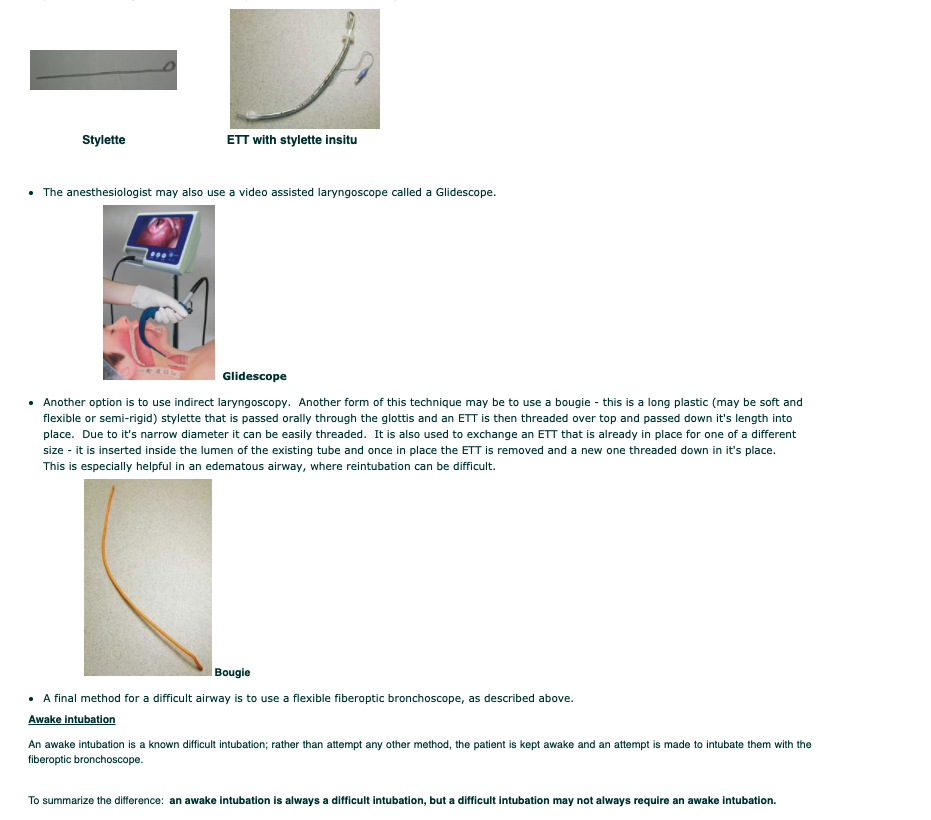
A flexible endoscope (bronchoscope) is used to visualize the vocal cords when unable to do so with a regular laryngoscope. The “scope” is placed inside the ETT and then the scope is inserted via the nose or mouth and passed through the vocal cords into the trachea, the tube is threaded down over the scope and into the trachea. A flexible bronchoscope may also be used to check ET tube placement.
When a fiberoptic intubation is used, it is either an emergency situation where other attempts at laryngoscopy have failed. It is used in a known difficult airway patient and done when the patient is awake – this is called an awake intubation.
An awake intubation is done for patient’s that have:
- A known difficult airway/ intubation i.e. Ankylosing spondylitis, previous cervical fusion surgery
- Failed intubation
- Potentially unstable cervical spine i.e. cervical trauma, rheumatoid arthritis
It is achieved by using a variety of types of topical anesthetics (Lidocaine) – mouthwash, sprays, tracheal injection – to freeze the vocal cords and diminish the gag reflex. The patient is also given a mild sedative, as it is necessary to obtain the patient’s cooperation and maintain a spontaneous airway, but at the same time it is necessary to relieve anxiety and discomfort. This process may take some time (~15 minutes).
Once a sufficient level of topical anesthesia is achieved, a flexible endoscope (with an ETT threaded over the end) is used to visualize the vocal cords. The scope is inserted into the mouth (more common than the nasal route) and passed through the vocal cords into the trachea, and then the tube is directed down over the scope and into the trachea. The scope allows for suctioning of secretions and a definitive placement of the ETT. Once the ETT is placed, the scope is removed, the cuff is inflated and secured. Anesthetic drugs can now be administered once the airway is secured.
Other Intubation Supplies #
Other necessary supplies (beside the laryngoscope and ETT tubes) are assistive supplies like Magill forceps, bougies and stylettes; and the following:
Oral airway: used to keep the patient’s tongue from obstructing airway during preoxygenation prior to intubation (sized by # i.e. #3).
To choose the proper size oral airway, hold the airway against the side of the patient’s face – it should extend from the corner of the patient’s mouth to the angle of the jaw (below the ear lobe).
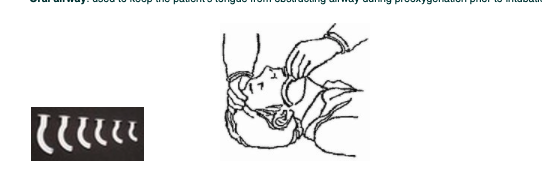
Nasal airway: a nasal airway may be used instead of an oral airway (sized in French). It is often used more often postoperatively.

Breathing Circuit: used to manually ventilate the patient and to preoxygenate prior to intubation. The intubating mask is attached to anesthetic tubing, which attaches to the anesthetic machine. A filter is placed at the expiratory end of the tubing to prevent any infectious matter from entering the anesthetic circuit. The rebreathing bag is a reservoir filled with oxygen that the anesthesiologist will use to “bag” the patient during manual ventilation – squeezing the bag forces oxygen through the inspiratory end of the anesthetic tubing and into the patient’s lungs. After intubation, the anesthetic tubing is connected to the ETT.
Lidocaine spray: given to prevent larygospasm and numb vocal cords as the ETT passes. It comes in a prefilled syringe (Laryngojet) or as an aerosol spray with disposable nozzle.
Syringe: a 10-20 cc syringe is necessary to inflate the cuff of the ETT tube or LMA.
Tape or ties: used to secure the ETT
Lubricating jelly: used to ensure easy removal of the stylette from the lumen of the ETT or for inserting the LMA (less mucosal trauma)
Difficult Intubation vs. Awake Intubation #
Difficult Intubation
A patient may have a variety of reasons why they are difficult to intubate (i.e. short neck, large tongue, anterior larynx, cervical arthritis, etc) and may require different techniques to intubate. The anesthesiologist may start with direct laryngoscopy.
- A stylette is a bendable metal guide coated with plastic that is inserted inside the ETT and allows the ETT to be shaped; and allow for placement through the vocal cords in patients with an anterior larynx.
The Role of the LPN During Regional Anesthesia #
Role of the LPN during Regional Anesthesia #
As professional, LPNs adhere to the Professional Standards of Practice. Your role during the administration of regional anesthesia will depend on your profession’s scope of practice (the range of activities that your profession is authorized to perform based on educational preparation and certification).
Regional Anesthesia #
Regional anesthesia is achieved by the temporary interruption of the transmission of motor and sensory nerve impulses to and from a specific area or region of the body. Regional anesthesia produces analgesia and muscle relaxation – two of the goals of anesthesia – without altering the patient’s level of consciousness. General anesthesia requires total body anesthesia, whereas regional anesthesia produces anesthesia that is selective to the surgical site.
Local anesthetic drugs are injected into close proximity to selected nerves and produce anesthesia in the region of injection. Depending on the dose, the drug provides absence of sensation (anesthesia) and absence of pain without disruption of other sensory modalities (analgesia). The patient will also receive an anxiolytic drug (i.e. Midazolam or Propofol) in sub-anesthetic doses to relieve anxiety. Opioid analgesics may also be administered to supplement pain management.
Regional anesthesia involves a number of techniques and is classified according to the site where the local anesthetic is injected. The types of regional anesthesia to be discussed are:
- Topical and Infiltration
- Peripheral nerve blocks
- Intravenous Bier block
- Neuroaxial (Central) blocks: spinal and epidural anesthesia
Topical and Infiltration Anesthesia #
Topical and infiltration anesthesia are often referred to as local anesthesia. The patient will be awake or slightly sedated during this type of anesthetic, so it is important to keep noise to a minimum and conversation appropriate and confidential.
Topical Anesthesia #
A local anesthetic may be applied directly to the surface of an area requiring desensitization for a short period of time. Examples of this are:
- Lidocaine spray or gel applied to the mucous membranes of the respiratory tract prior to intubation (i.e. awake intubation)
- Tetracaine drops used for short examinations of the eye
- Emla cream applied to the skin for painful intravenous insertions
 #
#
Infiltration Anesthesia #
Infiltration of local anesthetic involves injection of the drug directly into the surgical area (local block) or into the tissue surrounding the surgical area (field block). This technique may be used to suture a superficial wound or injected around or into the surgical site at the beginning of the procedure or at the end in order to provide postoperative analgesia. The addition of a vasoconstrictor agent is often used to reduce bleeding in and around the surgical site (i.e. Marcaine 0.25% with 1:200,000 Epinephrine). The vasoconstrictor also aids in decreasing blood flow around the area, causing a slower redistribution of the drug away from the area – drugs with Epinephrine added double their duration of action.
Monitored Anesthetic Care (MAC) #
Monitored anesthetic care or MAC is where the anesthesiologist monitors the patient’s vital signs and level of comfort, but is not the one administering the anesthetic – this is done by the surgeon in the form of topical or infiltration anesthesia. The anesthesiologist is present in case the local anesthetic drugs might not be enough for the patient and in which case they may administer a light sedative or convert to a general anesthetic if required. An anesthesiologist will also monitor for side effects of local infiltration (i.e. total anesthesia after a retrobulbar block is administered).
When MAC is not required, for example in a simple wound suturing, there will be a registered nurse who will be responsible for monitoring the patient. Usually pulse oximetry and blood pressure monitoring are sufficient, but in some institutions ECG monitoring will also be done. Even if a scrub nurse is not required, two nurses – one a registered nurse to monitor the patient and another perioperative nurse to assist the surgeon.
Peripheral Nerve Blocks (PNB) #
In a peripheral nerve block the local anesthetic is injected around a peripheral nerve or nerve plexus that innervates a particular area of the body (encompassing the surgical site). Peripheral nerve blocks provide anesthesia as well as some akinesia (lack of movement), as sensory and motor impulses are blocked to and from the injected nerves. They can be performed for surgical anesthesia or for postoperative pain control. For longer term pain control, a catheter may also be inserted, which will allow for repeated injections of local anesthetic. Examples of peripheral nerve blocks are brachial plexus (for the shoulder), axillary block (for the hand and medial side of the forearm), ulnar/median/radial nerve blocks (for the hand), femoral nerve (for the leg), popliteal (for the lower leg) and peribulbar and retrobulbar blocks (for the eye).
To administer a peripheral nerve block, the anesthesiologist will follow these steps:
- Cleanse the area with antiseptic solution around the nerve location
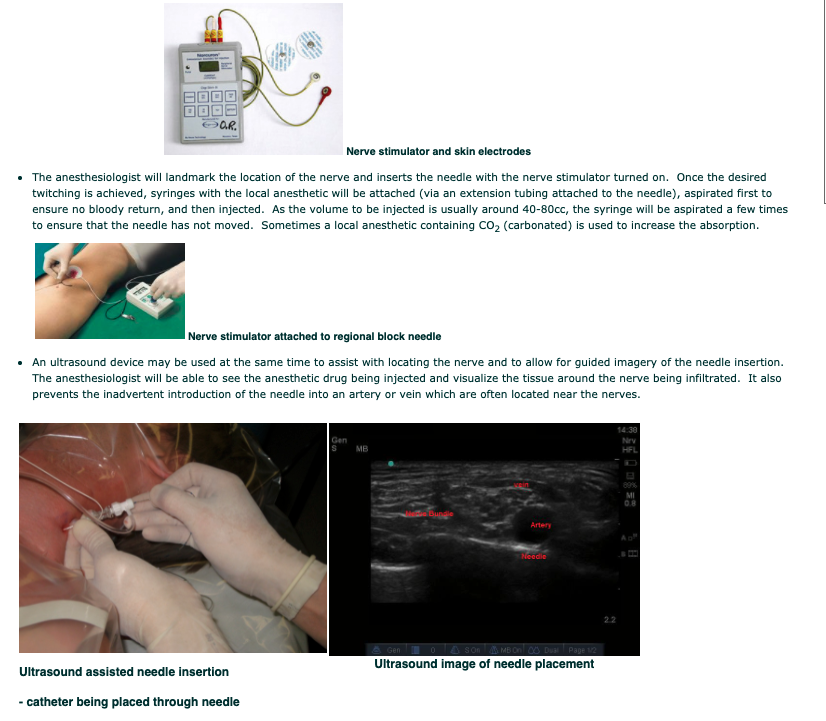
- Locate the nerve or nerve plexus with the use of a special insulated needle (regional block needle). This needle has wires attached that will connect to a nerve stimulator – one conducting wire and one ground wire. The nerve stimulator will send impulses down the needle shaft which will help to locate the nerve (motor branch), by stimulating the nerve and producing twitching of the muscles around it.
- A tourniquet is often used for surgery of the extremities so it is important that the block extend far enough up the limb to allow for the discomfort of the tourniquet site as well as the surgical site.
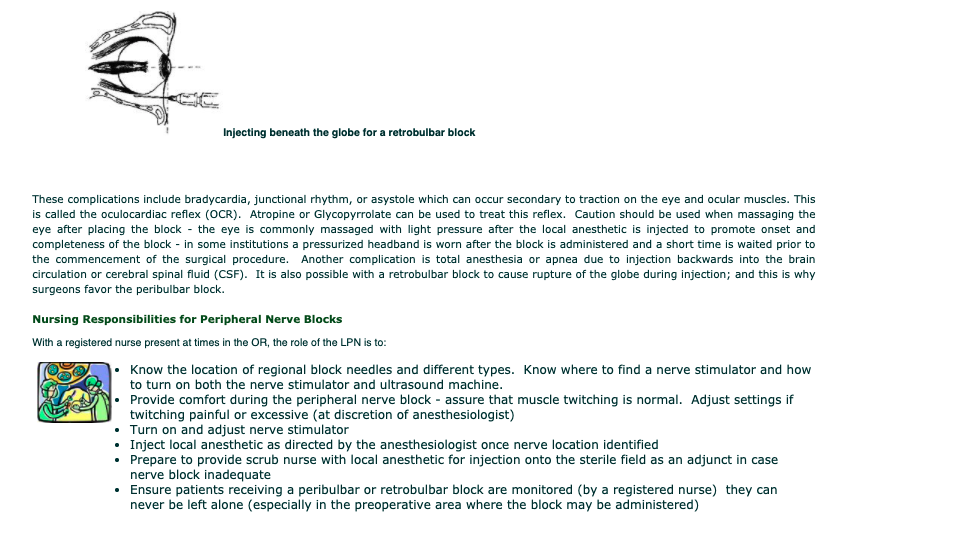
Peribulbar and Retrobulbar Blocks #
Ophthalmic blocks are administered by the ophthalmologist with the anesthesiologist providing MAC, as these blocks have potentially serious side effects.
The peribulbar block involves injections above and below the orbit, with local anesthetic deposited in the orbicularis oculi muscle and beneath, above and behind the globe. The potential for intraocular or intradural injection is limited because the anesthetic is deposited outside the muscle cone. The risk of intraconal hemorrhage and direct optic nerve injury is also less than with a retrobulbar block.
A retrobulbar block is a regional anesthetic nerve block into the retrobulbar space, the area located behind the globe of the eye. Local anesthetic is injected into this space. This injection provides akinesia of the extraocular muscles by blocking cranial nerves III, IV, and VI, thereby preventing movement of the globe. It also provides sensory anesthesia of the conjunctiva, cornea and uvea by blocking the ciliary nerves. This block can be used for cataract surgery but may be used for other intraocular surgeries; although it’s risk of complications are making the peribulbar block more common.
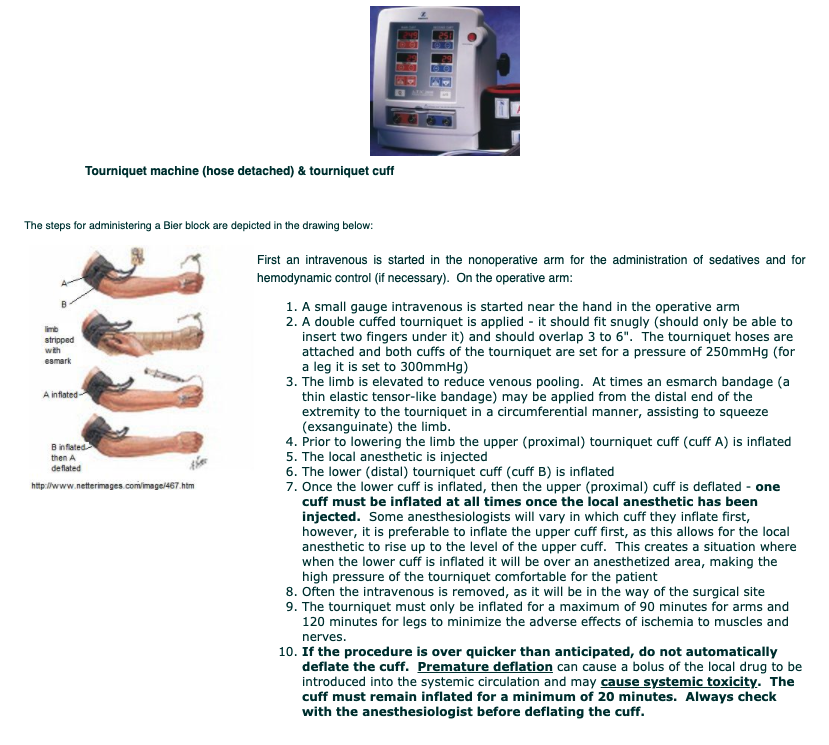
Intravenous Block (Bier Block) #
An intravenous block, commonly referred to as a Bier block, is the type of anesthesia used on an extremity – typically the arm (rarely the leg) for procedures of about an hour duration (i.e. hand procedures such as tendon repair). The Bier block works by injecting the local anesthetic via an intravenous while circulation to the limb is occluded by a pneumatic tourniquet. The tourniquet ensures that the local anesthetic remains within the extremity, until the pressure is released. The dosage of the drug must be determined for the length of the procedure, as very little drug should be left unmetabolized prior to the deflation of the tourniquet and to prevent the release of a bolus of the local anesthetic drug systemically (potential for systemic toxicity).

Central Nerve Blocks #
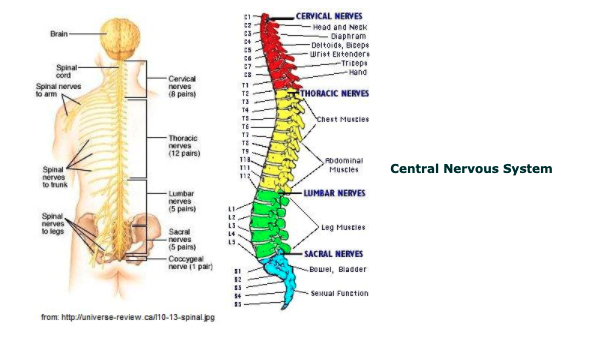
Neuroaxial (central) blocks are accomplished by depositing the local anesthetic in proximity to the spinal cord and it’s nerve roots. There are two types of central nerve blocks that will be discussed – spinal and epidural.
Anatomy and Physiology #
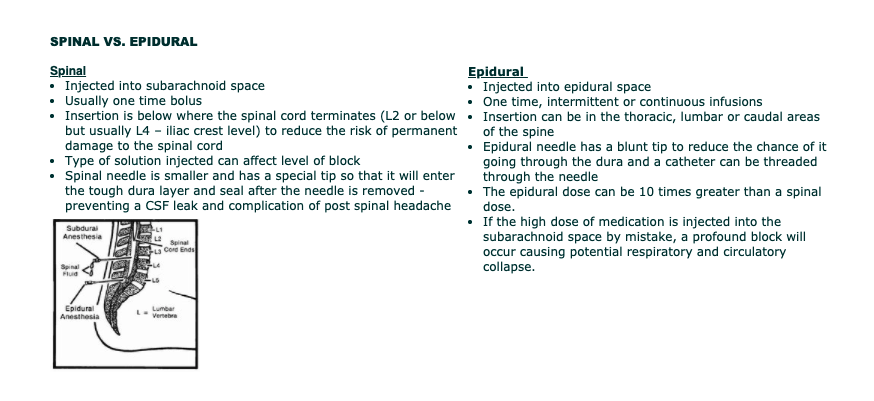
Epidural or spinal analgesia/anesthesia involves the injection of an opioid, local anesthetic or a combination of both into the epidural or subarachnoid space. The spinal cord occupies the upper two thirds of the vertebral canal. It is approximately 42 cm long and usually ends at the level of the first lumbar vertebra (L1).
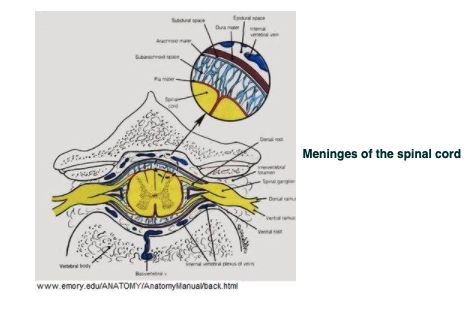
The brain and spinal cord are continuous and are encased by 3 membranes:
- the dura mater (the tough outermost layer),
- the arachnoid, and
- the pia mater (thin innermost layer adherent to the brain and spinal cord).
Between the pia mater and the arachnoid is the subarachnoid space which is filled with cerebral spinal fluid (CSF). The total volume of CSF is about 150ml and 20-30ml of this is found in the spinal canal. The spinal cord gives off 31 pairs of spinal roots and nerves. The autonomic parasympathetic fibers have craniosacral origins, and the sympathetic fibers arise from the thoracolumbar area of the spinal cord. After leaving the spinal cord, the spinal roots and autonomic nerves pass through the subarachnoid and epidural spaces, forming peripheral nerves and nerve plexuses leaving the spinal cord.
Spinal Anesthesia #
Spinal anesthesia is accomplished by injection of the local anesthetic drug into the subarachnoid (intrathecal) space of the spinal column.
The subarachnoid space is an actual space between the arachnoid and the pia mater. Medication injected into this space mixes with the CSF around the spinal cord and spinal cord nerve roots. When inserting a needle into this space it is important to enter the space below the level of the spinal cord termination to reduce the risk of permanent damage to the cord. Anesthesiologists will use the iliac crest, which is approximately the level of L4, as a landmark. The subarachnoid space lies between the pia mater and the arachnoid and is filled with cerebral spinal fluid (CSF) – see diagram below. Local anesthetic is injected into this space and mixes with the CSF around the spinal cord and spinal cord nerve roots.
Blockade Sequence #
Progression of the blockade is based on the size, anatomy and location of the nerve fibers in the subarachnoid space. In spinal anesthesia the progression usually begins in the feed (caudally) and progresses upward (cephalad), in the following way:
- Vasodilation: increased in cutaneous perfusion – patient will experience a warmth in the affected area
- Cold Discrimination: patient will report advancing sensation of warmth – toes to head. Will report sensation of warmth to cold stimulus (i.e. when touched with ice or alcohol swab)
- Fast and dull pain: patient will report dull pain in affected areas (i.e. when touched by a pin) and sharp pain in unaffected areas. Surgeon will always test prior to making incision by pinching the patient’s skin with forceps.
- Light vs. deep touch: unable to feel light touch, but deeper touch may still be present
- Proprioception: patient is unable to discriminate position or location of blocked extremities
- Motor: patient will be unable to move affected area/limbs
Once this last stage of blockade has been reached, it can be assumed that the block is successful and it can be determined how far cephalad the block has taken effect.
As the blockade wears off, it will occur in the opposite order. That is to say, motor function will return first; this is what makes central nerve blocks appropriate for postoperative pain control – the lack of sensory perception (pain control) for some time after motor function has returned.
Spinal Anesthesia: Hyperbaric vs. Hypobaric Solutions #
Depending on the type of local anesthetic solution used the patient may be asking to remain in the sitting or lateral position, so that the solution can “descend” – this can make the block descend to levels lower than where it was injected or make the block unilateral (i.e. if lying on the left side it can stay only on the left side and the right side unaffected). It can also make the solution “rise” if the patient is moved out of position too soon – it can take up to 10 minutes for the solution to “settle”. This is achieved through the weight or baricity of the solution relative to CSF. There are three types of solutions:
- Isobaric: solution has the same weight as CSF. This type of solution will remain in the area that it was injected – resist spread. Therefore, the patient can be repositioned immediately after injection without altering the level of anesthesia.
- Hyperbaric: solution is heavier than CSF. This is achieved by mixing the local anesthetic with a glucose (D5W) solution. Being heavier than CSF hyperbaric solutions tend to settle to the most dependent area of the subarachnoid space. The most dependent area was determined by the position the patient is in when the drug was injected. In the sitting position if injected at the L2-3 interspace will cause the solution to sink to the sacral segments of the spinal cord. If the patient is lateral, an injection at the L2-3 interspace will cause the dependent hip and leg to be affected. If the patient is supine, the drug will gravitate up into the thoracic region, creating unnecessary or unwanted thoracic involvement.
- Hypobaric: solution is lighter than CSF. This is achieved by the addition of sterile water to the solution. This type of solution is not commonly used, as it’s level of spread to the nondependent area can be unpredictable in the sitting position.
Epidural Anesthesia #
Epidural anesthesia is accomplished by injection of the local anesthetic drug into the epidural space.
The epidural space is a potential space containing blood vessels, lymphatics, fatty tissue and spinal nerve roots. It is located outside the 3 membranes covering the spinal cord, between the dura mater and the ligamentum flavum. Venous plexus are prominent, but no free fluid exists in the epidural space. The ligamentum flavum is an extremely tough ligament binding the spinal vertebra together, and it must be punctured in order to access the epidural space found just beyond it.
The local anesthetic solution eventually diffuses across the dura and arachnoid membranes into the subarachnoid space. There is no free fluid in the epidural space so epidural bolus can be given hours apart via a catheter without the catheter clotting.
Anesthetic Complications #
There are many complications of different surgical procedures themselves, but what are the emergency situations that can occur while a patient is undergoing an anesthetic? Some are unique to anesthetics themselves, while others are linked not only to the stress of undergoing an anesthetic, but to the surgical procedure itself. Let us discuss six such complications.
Malignant Hyperthermia #
Malignant hyperthermia (MH) is a fulminating hypermetabolic state occurring in genetically predisposed individuals when exposed to triggering agents. Potential triggering agents include commonly used gaseous inhalation anesthetics (i.e. Isoflurane, Desflurane, Sevoflurane, and Methoxyflurane); the muscle relaxant Succinylcholine and some local anesthetics (Lidocaine).
The triggering agent increases the intracellular calcium ion concentration. The elevated calcium level produces a chain of reactions whose signs include a greatly increased body metabolism, muscle rigidity and high fever which may exceed 42° C (thus the name hyperthermia). Death or brain damage may result from cardiac arrest, internal hemorrhaging or failure of other body systems. Episodes of malignant hyperthermia are rare and most often occur in children and young adults. The exact incidence is unknown but may be as frequent as 1 in 5,000 or as rare as 1 in 65,000. MH susceptibility is an inherited gene, and males are more likely to develop MH than females. A mortality rate of nearly 80% in 1960, when MH was first identified, has been dramatically reduced by the introduction in 1979 of the drug Dantrolene sodium (drug for reversing the exacerbated release of calcium).
MH is suspected if a person has a family history of severe reactions during anesthesia. The diagnosis can be confirmed or ruled out by skeletal muscle biopsy. This involves surgical removal under MH-safe anesthesia of a piece of muscle and usually subjecting the removed muscle to standardized laboratory testing.
Signs and symptoms of MH:
- Early signs of an MH reaction are increased CO2 in blood or exhaled gas, rapid irregular heart rate, excessively rapid deep breathing, and blueness of the skin .
- Followed by muscle rigidity – masseter muscle of jaw common indicator – (MH causes an intense release of calcium into the muscle cells causing contraction), acidity of the blood and muscle cell damage
- This is followed by the body temperature rapidly rising to extremely high values (> 42°C)
- If the reaction is unchecked the muscle cell membrane is disrupted causing leakage of myoglobin (→ kidney failure), leakage of K+ and Ca++ (→ heart failure and cardiac arrest), failure of coagulation, and eventually brain death may result
- Not every MH reaction will exhibit all the features of an MH reaction, thereby making the diagnosis difficult sometimes.
Treatment:
- Strict preoperative screening (ask re: family history) and in some high risk cases administration of preventive dose of Dantrolene
- Removal of all triggering agents from the operating room preoperatively for known cases
- Early diagnosis of symptoms and prompt treatment: stop triggering agent, flush with 100% O2 to clear anesthetic machine of all inhalational gases and hyperventilate patient with 100% O2 (may have to manually ventilate patient at this time)
- Administration of IV Dantrolene – this drug needs to be reconstituted and given in large quantities
- Cool patient with cooling blanket, sterile ice (slush) in operative wound, ice lavage (gastric, urinary and rectal), ice packs in armpits and groin
- Treat other hemodynamic symptoms (i.e. acidosis → administer Sodium bicarbonate), observe end tidal CO2 and arrhythmias
- Provide with isolation room in PAR, as the expiration of gases from other patients, can also trigger a reaction. Patient is at risk for up to 48 hours after receiving an anesthetic
Laryngospasm #
Laryngospasm is a forceful involuntary spasm of the laryngeal musculature caused by sensory stimulation of the superior laryngeal nerve. Triggering stimuli include pharyngeal secretions, the presence of blood, food, vomitus or a foreign body in the larynx or passing of the endotracheal tube (ET) through the larynx during extubation.
This glottis closure reflex can continue even after the irritation to the mucosa ceases. Varying degrees of laryngospasm produce sounds that range from a high-pitched squeaky crowing to total absence of sound. The latter indicates complete closure of the cords and there is no airflow. Laryngospasm occurs most commonly upon extubation of the patient, the anesthesiologist will be the individual directing the treatment of this condition, suctioning to remove secretions, blood etc, repositioning of the mandible in combination with oxygen by mask under positive pressure is often all that is needed to treat this condition. However, if the condition persists a short acting muscle relaxant such as Succinylcholine may be administered. As a last resort, the patient may have to be reintubated.

Airway Obstruction #
Airway obstruction can be described by:
- Location – upper or lower. Upper airway obstruction, glottic and supraglottic, can have the greatest impact on the postoperative patient as the lack of any air exchange.
- Degree – partial or complete. Laryngospasm is a form of complete airway obstruction. Partial airway obstruction can develop into a complete obstruction if not treated.
Anesthesia related causes can be:
- Inadequate reversal of muscle relaxation
- General anesthesia depresses the airway reflexes of coughing and swallowing resulting in the inability to clear secretions
- Glottic edema from tracheal intubation
- Peripheral nerve blocks to the head and neck area can potentially injure blood vessels and the resultant bleeding can compress the airway directly or through mucosal edema from obstructed venous drainage.
Surgery related causes result from procedures around the head and neck and can cause obstruction by causing displacement or compression of the airway by:
- Soft tissue edema around the head and neck – steroids may be administered preoperatively if this is anticipated
- Dislodgement of surgical packing or clots
- Bleeding into or adjacent to the airway
- Accidental transection of nerves involved in reflexes (gag, swallowing, coughing) i.e. recurrent laryngeal nerve
- Surgical positions that require the patient to be head down or prone can cause facial and neck edema
Patient related causes can be from:
- Medical conditions resulting in neuromuscular weakness, especially of pharyngeal and laryngeal muscles (prevent spontaneous airway clearance by weakened cough) i.e. Myasthenia Gravis or ALS
- Pre-existing airway diseases such as asthma, bronchitis or smoking
- Excessive soft tissue surrounding the airway increases the risk for edema
- Excess soft tissue of head, neck and trunk impair mandibular and cervical mobility and ability to position airway for maximal patency
- High risk for gastric aspiration secondary to increased intragastric pressure (i.e. pregnancy), increased gastric volume (i.e. recent meal) and decreased tone at the lower esophageal sphincter (i.e. GERD)
- Elderly patients: potential to dislodge teeth; diminished laryngeal reflex reactivity; limited cervical (neck) mobility
- Pediatric patients (under 8 years old): large head causes flexion of short neck; larger soft tissue structures (tongue and epiglottis); larynx is more cephalad than an adult which results in greater airway closure when neck is extended; shorter trachea; and narrower subglottic airway
- Trauma to the head and neck

Hypothermia #
Hypothermia is a common problem for perioperative patients in that it has a negative impact intraoperatively and in postoperative recovery. The effects of hypothermia are manifested in such areas as:
- Increased incidence of wound infection
- Altered cardiac performance
- Altered coagulopathy
- Altered action of common anesthetic drugs
- Delayed emergence from anesthesia
Why are perioperative patients prone to hypothermia? The main reason is anesthetic agents cause vasodilation between the warm central circulation and the cool peripheral circulation; leading to heat loss through radiation, convection, conduction or evaporation. Examples of this are:
- The room itself is kept cool, due to air exchange for infection control and OR personnel are scrubbed under warm operative lights
- IV fluids may be room temperature
- Irrigation fluids may be room temperature
- Body surface is exposed to the cool room air during positioning and skin preparation
- Some skin prep solutions are alcohol based
- Body cavities are open to room air during surgery
- Unwarmed, unhumidified gases
Take a moment to reflect on what happens to your body when you are cold.
What is hypothermia and why is it so bad for the patient?
- Postoperative hypothermia is defined as temperature < 36°C
- The elderly and children are the most vulnerable
- Postoperative shivering increases the need for oxygen by 300-400% and increases the risk of myocardial ischemia and angina
- During general anesthesia the body cannot compensate for hypothermia – anesthetics inhibit central thermoregulation by interfering with hypothalamic function
- There is a shift in the oxyhemoglobin dissociation curve – Hemoglobin has a greater affinity for oxygen and does not readily release it for cell and tissue use
- There is a loss of intravascular volume due to vasoconstriction
- When the body re-warms and vasodilation occurs, the patient becomes hypovolemic
Negative effects of hypothermia:
- CNS depression → increased level of anesthesia
- Drugs, especially muscle relaxants, are metabolized more slowly
- Clotting abnormalities (↑ platelet activity, ↓ fibrinolysis)
- Increases the incidence of wound infection (due to vasoconstriction)
What can the LPN do to reduce the chances of the patient becoming hypothermic?

Inadvertent hypothermia is a preventable complication of surgery. Understanding the causes and effects of hypothermia is essential in recognizing and implementing the most effective nursing interventions.
Hypovolemia #
The patient may present to the patient in a hypovolemic and/ or hypotensive state or may become so during the surgical procedure. If there is not frank bleeding, signs of symptoms of hypovolemia are ↑ heart rate and/ or arrhythmias, ↓ or unstable BP, and if larger volumes have been lost, coagulopathies develop. Some reasons for hypovolemia are:
- Trauma – severing of blood vessels, blunt trauma (intrabdominal)
- Highly vascularized tissue or tumors – some patients may have tumor vessels embolized prior to surgery to cut down on bleeding
- Surgical trauma – inadvertent nicking of an artery
- Medical conditions – patients on anticoagulants that have not been stopped preoperatively, ↑ INR, coagulopathic diseases (i.e. Hemophilia)
- Some patients are NPO for long periods of time and may be fluid (and electrolyte) depleted – the elderly and children are especially prone
Emergency Situations in the Operating Room #
Learning Objectives #
At the end of the unit the student will be able to:
- Understand how to respond to a respiratory and a cardiac arrest.
- Recognize the role of the LPN in a cardiac arrest and emergency situations.
Definitions #
Patients undergoing surgical intervention have an inherent risk of cardiac arrest due to the hazards of surgery. The perioperative nurse has a professional responsibility to understand the complexities of a cardiac arrest and its treatment. The following definitions distinguish the difference between a cardiac arrest, respiratory arrest, and code blue.
Cardiac Arrest #
A Cardiac Arrest is the sudden, abrupt loss of normal blood circulation due to the failure of the heart to function. Sudden death may occur within minutes after symptoms appear. Ventricular Fibrillation (VF) constitutes the most common electrical mechanism in cardiac arrest, and is responsible for 65 to 80% of occurrences. Another 20-30% is caused by severe bradyarrhythmias, pulseless electrical activity (PEA) and asystole. Other conditions are associated with impaired circulation due to a state of shock.
Respiratory Arrest #
Respiratory Arrest is the cessation of the normal tidal flow of the lungs due to any number of respiratory failures. It is a medical emergency and is usually related to or coincides with a cardiac arrest. If respiratory arrest is prolonged, cardiac arrest quickly follows because progressive hypoxemia impairs cardiac function. Respiratory arrests are less prevalent in the operating room because most patients are usually intubated and mechanically ventilated.
Code Blue #
One of many standardized hospital emergency codes, a Code Blue is called to alert staff that an emergency situation has occurred. A Code Blue is often called due to cardiac or respiratory arrest, but may also be used to represent a real or suspected imminent loss of life and can be called if any immediate and urgent treatment and/or back-up are required.
Causes of Cardiac Arrest in the Operating Room #
Causes of Cardiac Arrest #
Many factors can attribute solely or in combination to a cardiac arrest in the operating room. These factors include:
- Surgical management
Surgical management may involve uncontrollable hemorrhage, error in technique (surgeon accidentally nicks an artery), air embolism, and cerebral vascular accident.
- Anesthetic management
Anesthetic management may involve improper premedication, improper management of anesthetic, inadequate ventilation, myocardial depression, complication of regional techniques, aspiration, technical failure, failure to secure an airway, administration of the wrong anesthetic gas, and improper management of the immediate postoperative period (ventilation).
- Intraoperative pathological events
Intraoperative pathological events may consist of coronary ischemia mainly due to coronary vasospasm, arrhythmias, pulmonary embolism, and other conditions.
- Preoperative complications
Preoperative complications may be due to pre-existing conditions such as allergies, coronary artery disease, cardiomyopathy, hypokalemia, digitalis toxicity, severe myocardial depression, peritonitis, severe trauma, ruptured aortic aneurysm, abdominal hemorrhage, inhalation of blood and/or gastric contents (preoperative), pulmonary embolus during induction, intracerebral hemorrhage, cerebral edema, and meningitis.
Events Leading to a Cardiac Arrest #
There are certain events that may lead to a cardiac arrest in the operating room because they trigger the patient’s vasovagal responses during surgery. A vasovagal reaction activates the body’s parasympathetic nervous system and inhibits the body’s sympathetic nervous system leading to vasodilation and bradycardia. This response may occur during:
- Intubation and extubation of the endotracheal tube
- Tracheal suctioning
- Downward traction of the stomach or manipulation of the abdominal viscera
- Manipulation of the abdominal organs, common bile duct, and gallbladder
- Postural changes
- Pressure from positioning equipment or turning the patient under anesthesia
- When traction is placed on the peritoneum during closure
- Eye procedures where the eye muscles are stimulated (strabismus, scleral buckle, pressure on the eye)
- Patient with undue fear or apprehension
- Anaphylaxis
- Injection of contrast dye during an angiography (i.e. reaction to dye)
- Removal of aortic clamps during a surgery
- Placement of a Cardiac catheter (Pulmonary Aortic) in the right ventricle.
Treatment includes the restoration of venous return and correction of blood volume deficits.
Resuscitation Procedure #
Cardiac or respiratory arrest may occur in patients undergoing surgery because of the hazards of surgery due to hemorrhage, shock, or unfavorable reactions to anesthesia. Cardiopulmonary resuscitation (CPR) is the immediate restoration of circulatory and respiratory functions by mechanical or manual methods and the administration of drugs to stimulate ventilation and cardioconversion to a normal sinus rhythm. In a cardiac arrest CPR is vital to the patient’s survival, therefore, all perioperative nurses should have current CPR certification.
Resuscitation Procedure for a Cardiac Arrest in the Operating Room #
The resuscitation protocol for a cardiac arrest in the operating room should be understood by all operating room staff. The primary priorities in a cardiac arrest are AIRWAY management, CHEST COMPRESSIONS, defibrillation if required, and treatment of any dysrhythmias.
The hospital’s code team may be used in the perioperative areas and in others it may be the staff in the operating room that becomes the code team. When a cardiac arrest occurs in the operating theater, the anesthesiologist takes charge of the resuscitation.
Role of the Circulating Nurse (must be a RN) #
The importance of having two registered nurses during a cardiac arrest situation cannot be stressed enough – the need for specialized duties (IV medication, defibrillation, etc) and the ability to have the appropriate staff to respond at a moments notice.
One of the registered nurses will be designated as the in charge” nurse in a CODE BLUE situation. The circulating nurse should always stay with the patient and control traffic in the room ensuring that there is essential staff only. When a code blue is initiated (usually by the anesthesiologist) the designated registered nurse is responsible for:
- Calling for help with the emergency call system within the OR or perioperative area (CODE BLUE)
- Ensuring CPR is initiated and provide assistance if needed.
- Assisting the surgeon and anesthesiologist with resuscitation and defibrillation.
- Assigning a registered nurse to be the ‘recording nurse’ and delegating duties to other responders
Role of the Scrub Nurse #
The scrub nurse is responsible for:
- Remaining sterile, moving sterile items out of the way, and maintaining the sterility of the sterile items unless additional assistance is required (then unscrub and assist).
- Noting the start time of the CODE BLUE.
- Quickly covering the incision site with a sterile drape or towel.
Role of the Recording Nurse #
The Recording nurse (RN) is responsible for:
- Recording the times and events on the Resuscitation Record using the same clock or watch throughout the code. Confirm the start time with the anesthesiologist and the scrub nurse.
- Noting the procedures, drugs, and defibrillation and the patient’s response to the resuscitation.
- Ensure that the Resuscitation Record is completed, signed, and copies filed correctly. Documentation should be logical and concise.
The role of the LPN not in the scrub role or responding to a Code Blue #
The LPN responding to the code blue is responsible for:
- Bringing the cardiac arrest cart to the operating room or code blue location. Plugging in the defibrillator.
- Assisting and sending blood specimens to the lab.
- Acting as a runner to obtain supplies.
- Relieving rescuer performing chest compressions as required.
- Removing excess furniture and or equipment from area to allow more room.
- Be available and assist/respond to delegated activities to the best of your ability.
Death in the Operating Room #
The nursing responsibilities for a death in the operating room are hospital specific. It is important that the perioperative nurse understands the institution’s policy and procedure for handling death in the operating room. Here are some common points to note:
- The surgeon or anesthesiologist is responsible for pronouncing the death of the patient.
- All O.R. deaths are cases for the coroner because it is an unexpected outcome. It is the surgeon’s responsibility to notify and speak to the coroner.
- Do not remove any tubes or lines from the patient until cleared by the coroner.
- Do not remove any drugs, supplies or equipment from the room until cleared by the coroner.
- It is the surgeon’s responsibility to notify the patient’s relative(s) or significant other(s).
- The family may wish to view the patient prior to sending the patient to the morgue. Prior to bringing the family in (and after clearance from the coroner), clean the OR and make patient as presentable as possible for viewing. Support the family in their grief – call in a social worker if necessary.
- Debrief as a group after the fact. A death can be traumatic to all involved.
Spinal Anesthetic Block #
The step by step sequence to administering a spinal anesthetic block is as follows:
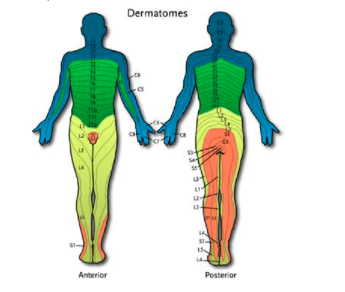
1.The anesthesiologist will cleanse the patient’s skin with antiseptic solution. They will then landmark the iliac crest and spinous processes of the spine – the iliac crest is level with the L4 spinous process. They will then count up or down to determine which level they wish to inject the local anesthetic. Having a knowledge of which nerve roots innervate which dermatomes of the body will determine at which level the spinal will need to be placed.
2.A nerve block that is too high (above the level of the T4 vertebra) can interfere with the intercostal muscles and spontaneous breathing. As the patient is often receiving a spinal anesthetic to avoid a general anesthetic, this can be a dangerous situation and require emergency intubation.
3.Once the right level is determined (i.e. L4 vertebra), the anesthesiologist will feel for the interspace between the vertebra above or below the selected vertebra (i.e. the L3-4 or the L4-5 interspace). A 30 gauge (G) 5/8″ needle is used to inject local anesthetic intradermally and then a 25 G 1 1/2″ needle is used for a deeper injection – this is to locally infiltrate the area, so the patient does not feel pain during the insertion of the spinal needle. However, they will feel pressure.
4. The spinal needle is a fine needle (22, 25 or 27 Gauge) with a sharp tip (Quinicke or Whitacre) and is about 3 1/2″ long. The spinal needle is inserted via a midline or paramedian approach to the chosen interspace, and advanced through the skin, spinous ligaments (supraspinal, interspinal and ligamentum flavum), the epidural space and finally through the dura mater into the subarachnoid space. This may take some time, as some patients have stenotic (narrowed) vertebrae making it difficult to find and enter the interspace. Once the needle has traversed the dura, a distinct “pop” is felt in the anesthesiologist’s fingers and confirmed by the presence of CSF dripping out of the needle hub (see picture below). In elderly patients the CSF pressure may be low, so it may take a moment to see the CSF appear.
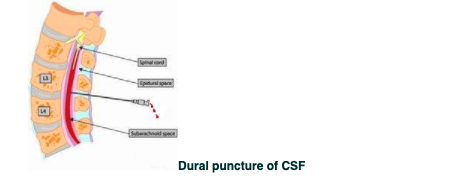
5.The syringe containing the local anesthetic is checked to make sure it is free of air bubbles and then attached to the hub of the spinal needle. Prior to injection, the anesthesiologist will aspirate about 0.2 ml of CSF to ensure proper placement, the drug is injected, CSF is aspirated once more, and then the needle and syringe are removed.
Epidural Anesthesia Block Sequence #
The sequence to administering an epidural anesthetic block is as follows:
Epidural Anesthesia #
The sequence to administering an epidural anesthetic (block) is as follows:
1. Position the patient as for a spinal. Follow the sequence for administering a spinal – steps 1-3.
2.The needle used for an epidural differs from a spinal needle in that it has a blunt tip, is of a wider bore (to introduce the epidural catheter through it, and it is approximately 3 1/2″ long. The needle is placed through a midline or paramedian approach to the chosen interspace, and advanced through the skin and spinous ligaments (supraspinal, interspinal and ligamentum flavum. A syringe of saline is attached to the hub of the needle, and then the needle is advanced further into the epidural space. Continuous pressure is placed on the barrel of the syringe as the needle is advanced. The epidural space is a potential space, therefore when the needle advances into the epidural space there will be a sudden loss of resistance and the syringe barrel will be easily depressed. This is called the loss of resistance technique – pictured below.

3. Once the needle is in place, the epidural catheter will be threaded through the needle. If it advances easily, then the needle placement is assumed to be in the correct location. The catheter is inserted to a depth of 7″. The catheter is taped to the patient’s skin according to the anesthesiologist’s preference – it is taped in such a way that kinking of the catheter is avoided.
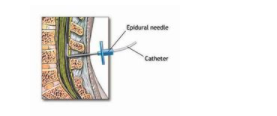
4. A filter is placed onto the end of the catheter, to ensure no bubbles or debris enter the catheter. The catheter is aspirated to ensure that there is no CSF return. A test dose is given via the catheter to ensure that the appropriate level of blockade is achieved and that the catheter is in the correct position. The sequence of blockade is similar to a spinal anesthetic. A higher dose of anesthetic drug must be administered, as it must traverse through the spinal meninges to affect the spinal nerves. It is a dangerous situation to have the catheter tip advance past the dura mater and have the large dose of local anesthetic injected into the CSF.
5.Further injections will be given via the catheter during the surgical procedure, depending on the length of the procedure. Alternatively, a dose will be given at the beginning and the end of the procedure for postoperative pain control. In the PAR, a continuous infusion will commence to provide postoperative analgesia. The catheter is usually kept in place for up to 5 days postoperatively and will be monitored by an anesthesiologist on the surgical ward.