Description #
To follow
Learning Objectives #
At the end of this module the student must be able to:
a) Demonstrate how bronchodilators are properly administered (MDI and nebulizer)
b) Understand the etiology and pathophysiology of acute bronchospasm.
c) Understand the risk factors contributing to the development of acute bronchospasm.
d) * Understand and identify the physical signs and symptoms of increased work of breathing.
e) * Demonstrate the immediate nursing interventions for a patient in acute bronchospasm.
(* – HPS only)
Asthma and Acute Bronchospasm #
Etiology:
Bronchospasm is an acute deterioration in the signs and symptoms of asthma. Asthma is defined as a chronic inflammatory disorder of the airways associated with increased airway responsiveness to a variety of stimuli. The inflammation causes recurrent episodes of shortness of breath (dyspnea), wheezing, and cough. Episodes are associated with airflow obstruction that occurs predominantly in the small-to-medium airways and reverses partially or completely, either spontaneously or with treatment.
The speed with which acute bronchospasm develops during an asthma exacerbation depends on the cause. Sudden attacks can be triggered by an allergen (pet dander, pollen, peanuts), irritant exposure (industrial chemicals, general air pollution, chlorine, crack cocaine), exercise, or by the use of some medications (non-steroidal anti-inflammatory agents, ß-adrenergic blockers) in susceptible patients. Slower onset attacks may be triggered by a viral infection, chronic exposure to low doses of allergens, and non-specific irritants. Slow onset attacks may also be triggered by gastro esophageal reflux disease (GERD). Status asthmaticus is an acute exacerbation of asthma characterized by severe acute bronchospasm, which is unresponsive to initial treatment. Status asthmaticus may lead to arterial carbon dioxide retention (hypercarbia), depletion of arterial oxygen (hypoxemia), respiratory failure and death.
Pathophysiology #
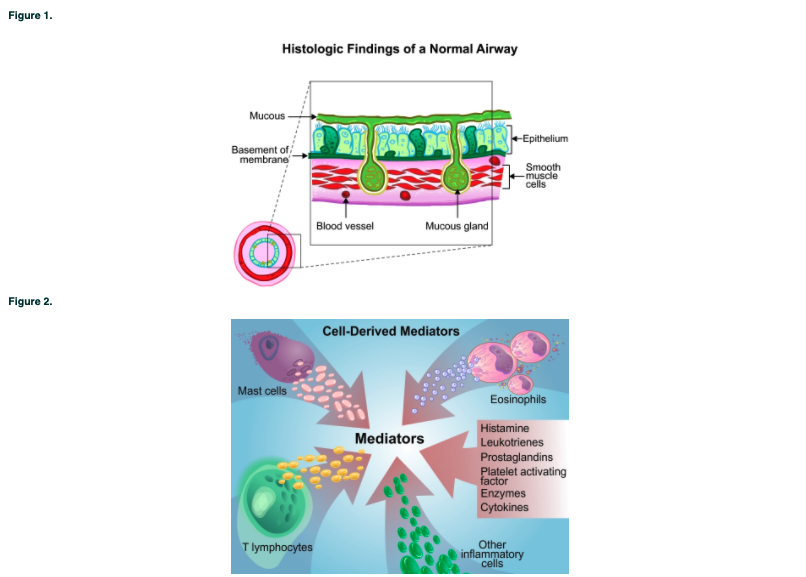
Airway inflammation in asthma is a direct response of the immune system to a trigger. Physiologically, an asthma exacerbation has two components: an early acute bronchospastic phase, marked by smooth muscle constriction causing narrowing of the airway. The later phase, which begins several minutes to hours after the early phase, results in mast cell degranulation, infiltration of T-lymphocytes and eosinophils, and the release of inflammatory mediators, including histamine, prostaglandins, and leukotrienes. These substances cause further airway smooth muscle contraction, increased capillary permeability, vascular fluid leakage, mucus secretion, desquamation of the airway epithelium, and activation of neuronal reflexes. These processes contribute to continued airway hyper responsiveness, bronchoconstriction, and sustained inflammation.
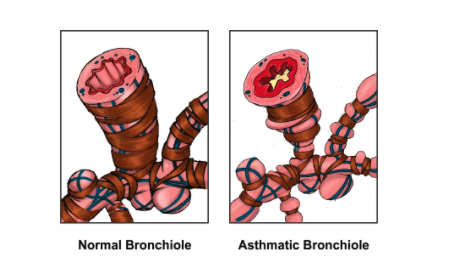
A cross-section of a normal airway is shown in the Figure 1. The single layer of ciliated epithelial cells lines and protects the bronchial wall. The mucous glands provide a protective layer of mucus above the epithelial cells. The smooth muscle cells are relaxed. Figure 2. depicts the inflammatory cascade in the second phase of acute bronchospasm.
Clinical Features #
During acute bronchospasm the asthmatic patient will complain of chest tightness, shortness of breath, wheezing, and coughing. Common findings include tachypnea, use of accessory muscles, a prolonged expiration, expiratory polyphonic wheezing, diaphoresis, and intercostals retractions. The patient will often be anxious, diaphoretic, and tachycardic.
Accessory muscles of breathing are used due to pulmonary hyperinflation. Hyperinflation causes the diaphragm to assume a flat position, which is less capable of effective ventilation. Increased anteroposterior diameter occurs when air trapping and pulmonary hyperinflation are present. In severe cases of bronchospasm, the patient’s expiratory flow may last for 60 seconds to try and expel trapped gas – a normal expiratory time is only 1 to 5 seconds. It is not uncommon to see a patient leaning forward and bracing their hands or elbows on a table during acute bronchospasm. This position may provide a better mechanical advantage for the accessory muscles (especially the sternocloidomastoid and scalene muscles) to assist breathing. The patient will assume the reclining position only when severely exhausted. Also, patient’s may instinctively breath with ‘pursed lips’, which creates a backpressure to splint open the airways.
Wheezing is caused by air rushing through a decreased airway diameter. The wheezes are often musical in nature, which is called polyphonic wheezing. Wheezing requires relatively rapid airflow through the airways, and silent chest indicates that there is insufficient airflow for noise generation, and is a sign of fatigue and respiratory failure. Localized wheezing or crackles may represent mucus plugging and atelectasis.
Intercostal retractions are seen as intermittent depressions of the skin around the rib cage with each inspiratory effort – they result when a significant drop in intrapleural pressure causes the skin overlying the chest wall to sink inward. Retractions are a clear indication that the patient’s work of breathing is severely increased, and respiratory fatigue may be imminent. Abdominal paradox is a sign of diaphragmatic fatigue. It is recognized by the inward movement of the abdomen during inspiration. Normal diaphragm contraction pushes the abdominal contents downward and outward during inspiration. Fatigue of the diaphragm allows it to be ‘sucked’ upwards into the chest when the accessory muscles create a negative intrathoracic pressure during inspiration.
Diagnosis:
Asthma should be considered in anyone who wheezes. The clinician should ask the patient about an asthmatic history, recent exacerbations, their severity, medications, their response to therapy, and any history of intubation. The patient should also be asked about any recent trigger exposure and respiratory tract infections. Differential diagnosis may include congestive heart failure, chronic bronchitis, pulmonary embolism, and upper airway obstruction. Diagnostic tools include pulse oximetry, simple bedside spirometry, arterial blood gases, chest X-ray, ECG, and blood work. Attacks may be mild (stage I), moderate (stage II), severe (III), or respiratory failure (IV).
Simple bedside spirometry is useful in objectively determining the severity of airflow obstruction and the response to therapy. Most people, unless in respiratory failure, are able to perform a simple spirometry measurement. Normal values vary considerably according to a person’s age, sex, and size. The peak expiratory flow rate (PEFR) measures airflow during forced expirations. The forced expiratory volume in one second (FEV1) measures the amount of air that can be exhaled in one second. PEFR or FEV1 less than 50% of predicted or the patients’ personal best can define moderate to severe acute bronchospasm (stage I to II). Simple spirometry will usually be done pre and post bronchodilator administration, to assess the response to medications. If a FEV1 is less than 1 liter, the PEFR is less than 200 l/min, or less than 30% of predicted values, and then an ABG will usually be done to determine the extent of any hypoxemia and acid-base status.
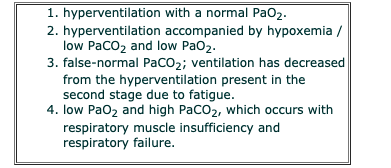
Arterial blood gases, specifically levels of hypoxemia and hypercapnia, are very useful in determining the severity of acute bronchospasm. Typically, the PaCO2 is decreased during the onset of bronchospasm, due to tachypnea. A normal or increased PaCO2 indicates that a more severe stage of airway obstruction has occurred. This is an extremely serious sign of respiratory muscle fatigue that signals the need for more intensive medical care, such as admission to the ICU and, probably, intubation with mechanical ventilation. A markedly increased PaCO2 indicates that the patient has started to become fatigued and has enough air trapping to retain CO2.
Table 1. The 4 stages of blood gas progression in acute bronchospasm:
The CXR may show hyperinflation of the lungs, and widened areas between the ribs. There may be signs of infection if this is the underlying cause. In the later stages of bronchospasm, there may also be atelectasis and areas of collapse due to mucus plugging. An ECG may reveal a sinus tachycardia with PAC’s and/or PVC’s. Bradycardia is an ominous sign of respiratory arrest, and is likely to occur during respiratory fatigue and failure. Lab data may reveal an elevated white blood cell count if infection is present, and a high lactate level due to the high work of breathing and high oxygen consumption.
Treatment:
The clinician should direct first-line treatment at maintaining adequate oxygenation, providing fast-acting bronchodilators, and reducing airway inflammation.
Oxygen therapy is always indicated, because patients having severe acute bronchospasm are invariably hypoxemic. Oxygen should be given at a level to maintain arterial oxygen saturations greater than 92%. This improves oxygen delivery to the peripheral tissues (including the respiratory muscles), reverses hypoxic pulmonary vasoconstriction, and may stimulate bronchodilation. Oxygen administration will also help ease a patient’s anxiety and improve their level of sensorium. Oxygen may dry airway mucosa, so it should always be humidified in an acute attack.
Along with oxygen, the first line of treatment for acute bronchospasm is fast-acting bronchodilators. Reversing or decreasing bronchospasm will allow the patient to exhale trapped air more effectively, which will help decrease the PaCO2. The most common bronchodilators used are short acting ß-agonists (salbutamol or Ventolin) and anticholinergics (ipratropium bromide or Atrovent). ß-agonist drugs stimulate ß-adrenergic receptors in the smooth muscle to dilate the airways and modulate inflammatory mediator release. They also inhibit pulmonary vascular leakage and enhance mucociliary clearance. side effects of ß-agonists are tremors, tachycardia, and nausea. Anticholinergic drugs block acetylcholine from causing smooth muscle contraction and from producing excess mucus in the bronchi. There are no known side effects to anticholinergics, but the onset is slower, 15 minutes to one hour, whereas the onset for ß-agonists is 1 to 15 minutes. Long acting ß-agonists (salmeterol, or Serevent) may be added to therapy once the patient is stable, to provide a more consistent control of symptoms.
Bronchodilators can be given by a metered dose inhaler (MDI) and spacer device, or by aerosolized small volume nebulizer (SVN). The MDI and spacer is the most popular route of administering bronchodilators to a stable patient. An MDI and spacer carry the advantage low cost and faster drug delivery time, but require hand to mouth coordination to perform proper technique. With severe bronchospasm, a small volume nebulizer is a more effective route, as the patient does not have to hold their breath to receive the full dose of the medications, and there is no technique to learn. Typically, bronchodilators are given every four to six hours, but during an acute attack, they may be given continuously until some resolution of symptoms occurs. (See Appendix 1. for proper use of MDI and spacer).
Corticosteroids are potent anti-inflammatory agents used in the management of asthma. IV administration of corticosteroids (methylprednisolone, prednisolone) cause a reduction in airway inflammation, a decrease in mucus secretion and airway edema, and a reduction in airway hyperresponsiveness of the airways. The mechanisms of action include the reduction of migration and inhibition of inflammatory cells, an increase in the number of ß-adrenergic receptors, and enhancement of the responsiveness of ß-agonist receptors (which will enhance the effectiveness of ß-agonist drugs). Corticosteroids also act on mast cells by slowing the synthesis of histamines. The benefits of inhaled corticosteroids are the same as by IV, but the onset is slower. The potential side effects of high-dose steroid medications include osteoporosis, immunosuppression, increased fat cell production, and hypertension. Patients who take inhaled oral steroids may also suffer from recurrent candidiasis (oral yeast infection/thrush).
IV methylxanthines (theophylline and aminophylline) are sometimes considered if bronchodilation cannot be achieved with ß-agonists, anticholinergics, or IV corticosteroids. Theophylline relaxes smooth muscle, and has some anti-inflammatory properties. Some studies have shown that theophylline also enhances mucociliary clearance by increasing cilia beat frequency.
Impending respiratory arrest (stage IV attack) requires sedation, oral intubation, and mechanical ventilation. Sedatives help to gain control of the airway, and decrease the work of breathing, decrease oxygen consumption, and help the patient feel comfortable on the ventilator. The largest diameter endotracheal tube should be used to decrease airway resistance and to remove mucus plugs with suctioning. Once on a ventilator, the patient who is refractory to treatment may receive inhaled anesthetic gases or IV anesthetics shown to produce bronchodilation, such as isoflurane and ketamine. Other goals of management include treatment of bacterial lung infections with antibiotics, mucolysis, and maintenance of adequate hydration. Because of the severity of the inflammatory response, the patient may have significant fluid loss, and should have a constant infusion of fluid to produce enough urine output for the patient’s age and size. Potassium balance should be carefully monitored due to the changes in arterial pH and by treatment with IV corticosteroids can cause urinary potassium loss.
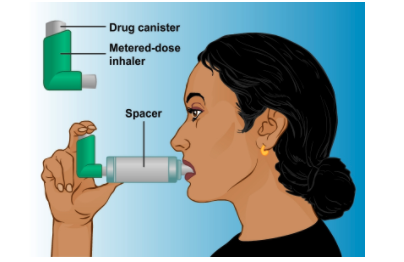
To Use a Spacer:
- Shake the inhaler well before use (3-4 shakes)
- Remove the cap from your inhaler
- Put the inhaler into the spacer as above
- Breathe out, away from the spacer
- Bring the spacer to your mouth, put the mouthpiece between your teeth and close your lips
- Press the top of your inhaler once
- Breathe in very slowly until you have taken a full breath. If you hear a whistle sound, you are breathing in too fast. Slowly breath in.
- Hold your breath for about ten seconds, then breath out.
- Repeat if necessary based on prescribed dosage.
References #
Beers, Mark H. (MD); Berkow, R. (MD), editors. The Merck Manual of Diagnosis and Therapy (seventeenth edition), 1999. Merck Research Laboratories, Whitehouse Station, New Jersey.
Canadian Thoracic Society, © 2000-2003 Canadian Asthma Consensus Guidelines
Fink, M., Abraham, E., Vincent, JL., Kochanek, P. Textbook of Critical Care (5th edition) 2005. Elselvier Suanders, Philadelphia, Pennsylvania.
Oh, T., Bernsten, A., and Soni, N., Oh’s Intensive Care Manual (5th Edition) 2003. N. Elsevier Ltd., London, England.