Description #
This module will provide an overview of preoperative patient care and will focus on patient assessment, the goals and modes of anesthesia delivery, the role of the perioperative nurse in assisting with anesthesia delivery, anesthetic complications and cardiac arrest.
Learning Objectives #
At the end of the session the nurse will be able to:
- Understand the important relationship between the nurse and the patient during the preoperative phase.
- Understand what information is important to collect and assess during the patient check in.
- Be familiar with delivery methods of anesthesia
- Understand the role of the RN for a patient experiencing anesthetic complications and cardiac arrest
Introduction #
To get you started…..
Think of a time in your own life when you felt vulnerable or out of your depth. Have you experienced a situation where you or a family member were treated in a health care setting and given little knowledge or control over the treatment?
- How did you feel?
- How did you perceive the people who were in control of the situation?
- What communication skills were used?
Patient Assessment #
Learning Objectives #
At the end of the session the nurse will be able to:
- Analyze a patient’s chart for pertinent information that will affect their operative course
- Utilize proper interview techniques to check in a patient & interact with family members
- Interpret and respond appropriately to pertinent lab values and tests as they pertain to a patient
- Provide psychosocial support to the patient undergoing an operative procedure
- Recognize the importance of and comply with surgical site marking
Nurse-Patient Relationship #
One of the most important responsibilities of the perioperative nurse is the preoperative patient “check in”. To the untrained observer, this interaction could be mistaken for a simple verification process; however, the preoperative patient assessment is often the only opportunity for the nurse to develop the rapport necessary to support the patient through what may be the most stressful time of their surgical experience. The perioperative nurse can take this opportunity to identify and understand the patient’s unique needs. It is also a time to collaborate with the patient in planning the care to meet those needs. This nurse-patient relationship is shaped by power, trust, respect and intimacy.
Power #
The perioperative nurse has a professional duty to regard the patient’s interests and well-being as paramount. Therefore, it is essential that the perioperative nurse ascertains and upholds the patient’s wishes in regards to their surgical care and treatment. The nurse must make a conscious effort to develop a partnership with the patient rather than assuming an authoritative role.
Trust #
Upon entering the operating room, the patient places their absolute trust in the perioperative nurse. This element of trust is critical because the patient’s ability to make decisions and exercise self-protection is compromised by anesthesia and the surgery itself. The perioperative nurse advocates for the patient at this time, passing on the patient’s concerns to the surgical team and ensuring that the patient’s needs are met, safely and effectively.
Trust and confidentiality go hand-in-hand. The patient assumes that the nurse can be trusted to maintain confidences. The nurse will respect the patient’s confidentiality and will only share information on a need-to-know basis with others involved in the delivery of care.
Respect #
The perioperative nurse should respect the patient and their decisions about health care. Part of respect is valuing the patient as an individual and maintaining their dignity. The nurse is accountable for promoting and protecting the patient’s interests irrespective of gender, age, culture, disability, socio-economic status, sexuality or religion.
Intimacy #
Intimacy refers to the ability of the perioperative nurse to establish a caring connection with patients. The patient is often anxious and stressed regarding the impending surgery, the possible outcome and their lack of control over the situation. The perioperative nurse can promote psychological and physical comfort by communicating empathetically with the patient, listening attentively, being alert to the patient’s nonverbal cues, offering gentle assurance and therapeutic touch, and providing explanations. A therapeutic relationship between the nurse and the patient not only fulfills the patient’s physical, psychosocial, and spiritual needs, but also contributes to the autonomy, professional satisfaction, and self-actualization of the nurse.
Preoperative Patient Assessment #
The Perioperative nurse is responsible for the assessment and admission of the patient into the operating room. During the preoperative phase, the nurse forms a therapeutic relationship with the patient and gathers data to ensure that patient care will be delivered safely and effectively. The interview is usually done in the preoperative area; either with the patient sitting in a chair or lying on a stretcher – this will depend on your institution’s method of transporting the patient to the OR theater (i.e. walking or being pushed on a stretcher) or it will depend on the patient’s physical condition.
The following video on patient assessment is in two parts. Part one outlines the procedure for conducting a preoperative assessment and the necessary information to be obtained. Part two is a demonstration of a nurse checking in a patient prior to surgery. Watch how efficiently this check-in/interview can be done when the nurse is organized and knows exactly what questions are necessary to ask:
Anesthesia #
Learning Objectives #
At the end of the module the nurse will be able to:
- Describe the three phases of a general anesthetic and identify relevant nursing implications
- Describe the routine monitoring equipment and more invasive monitoring techniques
- Understand the effects of all anesthetic medications used throughout the perioperative period
- Identify specific intubation equipment and know the purpose of the equipment
- Describe and demonstrate rapid sequence induction (cricoid pressure) and when it would be used
- Describe awake intubation, when it would be used and what equipment is required
- Describe regional anesthetic, insertion technique, potential complications and nursing responsibilities: epidural and spinal
- Describe other methods of anesthesia: monitored anesthetic care, various nerve blocks and local infiltration and when they are used
- Discuss the following anesthetic complications and their negative effects: postoperative hypothermia, malignant hyperthermia, laryngospasm, pseudocholinesterase deficiency, and hypovolemia
- Describe the role of the Registered Nurse during anesthetic emergencies.
History of Anesthesia #
The word anesthesia (sometimes spelled anaesthesia) is derived from a Greek word meaning “no sensation”. Today anesthesia can be described as a state in which the feelings of pain and other sensations are blocked. It can also be described as a “reversible lack of awareness”, this can be a total lack of awareness (as in a general anaesthestic) or a lack of awareness of a part of the body (as in a spinal anesthetic or nerve block).
The science of anesthesia has undergone many changes over the years. A brief synopsis of it’s history can be found in the Supplemental Information – Anesthesia: History of Anesthesia
Preparation of the Patient for Anesthesia #
Every patient who receives a form of anesthetic will be assessed perioperatively by an anesthesiologist.
The preoperative assessment notes the patient’s diagnosis, history, airway management and risk factors (surgical morbidity).
Many patients attend preoperative clinic visits to have all the appropriate tests completed and medication prescribed prior to surgery (ideally as close to date of surgery as possible). These visits ensure that the patients are in optimal condition to undergo the stress of a surgical procedure. Preoperative assessments are carried out in the following ways:
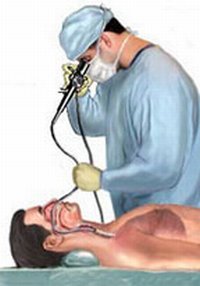
1.In a Pre-admission Clinic where lab tests, x-rays, physical exams and interviews are carried out by the anesthesiologist and a registered nurse. Watch the following video of an anesthesiologist in the Pre-admission clinic interviewing a patient for surgery:
Anesthetic Monitoring Equipment #
Significant advances in patient monitoring and anesthetic equipment have resulted in a decrease in risk to the surgical patient. The final responsibility for this equipment lies with the anesthesiologist, however, the Perioperative nurse must be familiar with the components, basic assembly and operation in order to assist the anesthesiologist.
A lot of mention will be made regarding the role of assisting the anesthesiologist, this infers a passive role, but it is just the opposite. It is the registered nurse in the perioperative role who has the assessment skills necessary to identify problems as they arise and has the skills with which to manage routine and emergent occurrences. It may seem at times that assistance requires just standing by, but problems can arise at any moment and the anesthesiologist will depend on your skill set to assist in moving the patient out of danger.
The different methods of monitoring a patient during surgery will be discussed (Review your textbook for further discussion). They will be divided into required monitors (required by law for any patient undergoing an anesthetic) and specialized monitors (used on a case or patient specific basis).
Required Monitoring Equipment #
Nonivasive Blood Pressure (NIBP)
- Preferably on arm contralateral to intravenous – BP tubing overlying brachial artery as marked on cuff, BP checked prior to induction. Avoid side with previous axillary node dissection.
- Cuff width should be 40% of circumference of extremity, bladder length encircle at least 80% of extremity. Cuffs come in a variety of sizes for the arm or thigh.
- Cuff reads falsely high if: cuff too narrow, too loose, extremity below heart level, uneven pressure
- Cuff reads falsely low if: cuff too large, extremity above heart level, quick deflation
- Artifacts caused by motion – shivering, surgeon bumping cuff, respiratory variation, kinking of tubing, loose connection or leak
- Taken every 5 minutes – may be more or less depending on patient or procedure

Electrocardiogram (ECG)
- Measures heart rate, rhythm, detects arrhythmias and ischemia, lead II is best for rhythm (provides the best view of the P wave).
- Three or five lead monitoring will be used – lead placement may be altered depending on the surgical incision site and patient position
- Artifacts caused by: incorrect calibration of ECG, inaccurate lead placement, poor connection, electrocautery, muscle artifact

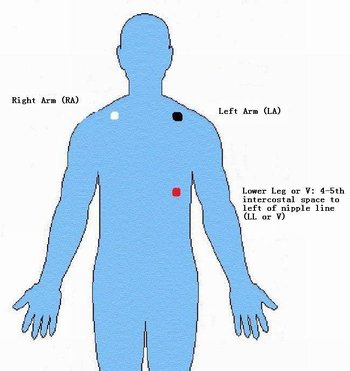
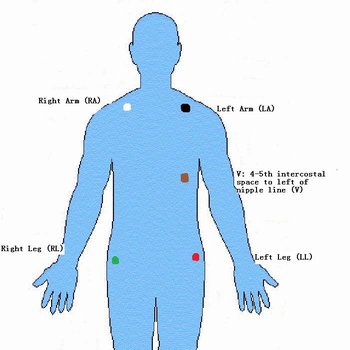
3 lead placement 5 lead placement
Oxygen saturation monitor
- Pulse oximeter – measures pulse rate and oxygen saturation of hemoglobin – preferably on finger on side contralateral to BP cuff – may also use toe, ear, nasal septum, lip (different probes are available)
- Principle of measurement – uses waveform to differentiate pulsatile arterial blood from non-pulsatile venous blood, skin, muscle, bone, fingernails, and polish
- absorption of light at two wavelengths, 660 nm and 940 nm, depending on amount of hemoglobin in oxygenated form compared to hemoglobin in reduced form (at < 90% there is less oxygenated hemoglobin readily available and SaO2 will drop quicker)
- SaO2% determined by ratio of light transmitted to photodetector
- Artifacts caused by abnormal hemoglobin, i.e. methemoglobin, carboxyhemoglobin, substance affecting absorption of light i.e. methylene blue, nail polish (blue, black, green), low flow conditions (hypothermia, vasoconstriction, hypotension), motion (shivering, agitation), ambient light
- Heart rate from electrocardiogram should be identical to heart rate from pulse oximeter to ensure oxygen saturation is accurate.
Oxygen saturation probe on index finger
Capnography – measurement of CO2
- Continuous measure of concentration of carbon dioxide, oxygen, and anesthetic gases in circuit – derives inspired and end tidal values of oxygen, CO2 (ETCO2), anesthetic gases
- Principles of measurement – infrared absorption proportional to concentration of gases present – highest value of CO2 called end tidal CO2 (ETCO2) – reflects alveolar and blood CO2 tension. End tidal anesthetic gases best reflect concentration of anesthetic in brain (target organ)
- Artifacts – may be obstructed by secretions or kinking of tubing
- – Water vapor may falsely elevate ETCO2
- – Nitrous oxide absorbs infrared, needs calibration
- – Lag time, the CO2 gas must travel from the patient to the monitor via long tubing
- – Air may be entrained, if there is a leak in the tubing, room air decreases the reading
- – Assume ventilation and perfusion matched to minimize gradient
- – Shallow breaths, prolongation of expiratory phase, uneven alveolar emptying
Suction
- Clean suction tubing and Yankauer tonsil suction tip present and functioning; liner requires a complete seal in suction container to fully function
Intravenous (IV)
- Adequate size intravenous (minimum 20 gauge) that runs freely. If patient has difficult veins, a small bore IV may be started to administer the anesthetic, and then a larger bore IV will be inserted after the patient is anesthetized (veins become dilated and easier to locate under anesthetic and it is less painful for the patient).
- Depending on the procedure more than one IV may be started i.e. primary line and a larger bore IV for blood transfusion or fluid volume
- Required even if local anesthetic is given – to counteract any negative physiological effects quickly
- Warm IV fluids are administered or a fluid warmer is used
- Rapid IV transfusors can be used to give large volumes of fluid or blood products rapidly (1 unit of RBC/minute)
Stethoscope
- To check respiratory sounds after endotracheal intubation
- To assess heart function – automatic monitors can never replace physical assessment
Temperature
- Not necessarily required, but required to be readily available (in the OR theater) if the patient’s condition should change
- Oral or temperature probes
- Temperature above 35°C
- Use of forced air warming blankets (BairHugger, WarmTouch) – upper body, full body and lower body blankets available
- Preferable to warm upper body (and head) over lower body for more effective overall core temperature warming
- Do not place warming hose next to skin or under a flannel blanket, as skin burns may occur (especially on highest setting) – there must always be a layer between the patient’s skin and the warming hose – use of manufacturer blanket is recommended.

Peripheral Nerve Stimulator
- Not required but must be readily available. It is required in order to assess the level of muscle relaxant still present in the body and therefore should be available, as muscle relaxation is used at some point for most surgeries. ECG patches are placed on the patient over muscle (temple or arm), stimulator cable attached to patches → small electrical current delivered to nerve, and degree or absence of twitch is measured
- If twitch prominent and surgery is still underway then more muscle relaxant will be given
- If twitch absent and surgery is finishing then a reversal agent (if possible) will be given

Specialized Monitoring #
Invasive blood pressure (Arterial line)
- Purpose: allows beat-to-beat measurement of blood pressure and frequent arterial blood sampling. Arterial lines are used for patient’s with cardiovascular issues, patients with anticipated large blood loss, and for obese patients (BMI > 40) in which accurate BP readings with even a large BP cuff are less than optimal.
- Supplies required: single line transducer kit, heparinized saline (as per hospital policy), connector cable for anesthetic machine monitor, pressure bag, IV pole clamp
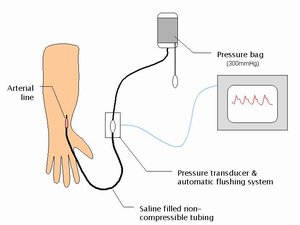
Arterial catheter insitu (radial artery) connected to transducer with resultant waveform
Arterial line supplies (pressure bag, NaCl, tubing & transducer cable)
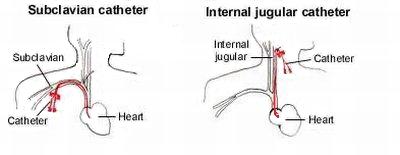
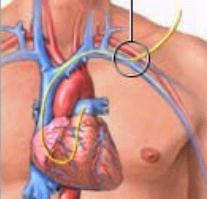
Central Venous Pressure (CVP)
- Purpose: accurate evaluation of hypovolemia or fluid overload, large bore IV access, ability to infuse inotropic and vasopressor drugs in larger doses
- Supplies required: saline, triple transducer kit, connector cable for anesthetic machine, IV pole clamp, central venous catheter kit (clarify the need for single, double and triple lumen)
- Inserted in the trendelenburg position (head down) to increase visibility of veins (venous congestion) and reduce the risk of air emboli
Pulmonary Artery Catheter (Swan Ganz)
- Purpose: monitors pulmonary artery pressure and gives indication of intra-vascular hemodynamics
- Used primarily for ICU, cardiac surgery and liver transplant patients
- Supplies required: same as CVP, Swan Ganz catheter, larger bore introducer kit
Urinary Catheter
- Fluid balance monitoring
- Urine output monitoring indicated for lengthy procedures (>2-3hrs) or for specific patient populations
- Urometer collection bags provide accurate output monitoring
Sequential Compression Device (SCD)
- Although not a piece of monitoring equipment, SCD’s are used to prevent venous stasis (DVT formation and pulmonary emboli)
- Risk factors for venous stasis: surgeries > 2 hours, over 40 years old, obesity, malignancy, prior history of varicose veins or pulmonary emboli, thrombophylic states, type of anesthesia, pre and postoperative mobility, level of hydration, presence of sepsis
- Contraindications: severe arterial disease of the lower extremities, dermatitis, gangrene, recent skin graft
- Thigh or knee-length compression sleeves are more effective when used in conjunction with compression stockings (TED)
- Indicated in procedures > 1hr (may be hospital-specific; a form of anticoagulant therapy may be used instead or in conjunction with SCD use)
Other
- Fetal monitor for obstetrical patients
- BIS® monitoring – a specially designed machine that monitors the depth of anesthesia; allows for accurate prediction or timing of return to consciousness
- Doppler ultrasound: to check for air embolus; also used during vascular surgery to check patency of vessels
- Trans-esophageal echocardiogram (TEE probe); used to check heart valve function during trauma or open heart surgery
- Ultrasound machine; used to accurately locate veins for IV or CVP placement, arteries for arterial puncture and for nerve blocks (avoid multiple punctures)
Nursing Responsibilities Regarding Patient Monitoring #
- Apply all required monitors (BP, ECG and pulse oximeter) onto the patient after the patient has been comfortably transferred to the operating room table and obtain the patient’s BP first.
- Obtain supplies for specialized monitoring and assist with insertion( learn location of supplies; identify resource people). The program will provide labs on how to set up for and assist with arterial and CVP lines.
- When transferring and positioning the patient, ensure that any invasive lines, tubings, or catheters are not kinked or pulled.
- For invasive monitoring lines, ensure that they are attached to the correct transducer cables, zero out and ensure that wavelength is adequately displayed on monitor (may need to reposition limb so that tubing or catheter is not kinked)
- Learn how to troubleshoot monitors/machines that are not working properly and/or identify who to contact for assistance
- Insert urinary catheter, using aseptic technique. Learn the options available (coude tip urinary catheters, notify specialist) for difficult urinary catheter insertions.
- Administer oxygen if patient experiencing low oxygen saturation levels; (may be due to suppressed respiration from preoperative narcotic or sedation administration)
- Always observe at the patient as well as the monitors (i.e. alarms may indicate that probes or leads have been dislodged).
- Apply SCD compression sleeves(attach to machine and turn the machine on)
- Provide warm IV fluids as necessary. Learn how to set up fluid warming devices (i.e. Gaymar fluid warmer).
- Use warmed flannel blankets as soon as patient enters the OR theater and upon emergence of anesthetic. Cover the patient with forced air warming blanket and adjust temperature as necessary during the surgical procedure.
- Provide support and comfort to the patient while patient is awake. Constantly monitor patient while under anesthesia.
- Some patients will be transferred to the ICU or PAR when intubated and will require monitoring during the transfer to these units. Portable monitors are used to assess arterial pressure, ECG and oxygen saturation (pulse oximeter). An ambu-bag and oxygen tank will also be required to provide bagged ventilation (if necessary) during transport. Duties include: providing and hooking up monitor, assisting with bagging the patient (turn oxygen up to 15 L/min), obtaining enough people to transport the patient safely (i.e. often have heavy bed, IV infusion pumps, ambu-bag etc). Depending on the hospital where you will be working, you may have Anesthetic Assistants (specially trained respiratory therapists) to assist with these transports.
Pharmacological Principles of Anesthesia #
Pharmodynamics and Pharmokinetics #
The drugs used during anesthesia involve many drugs that you are familiar with and a few that you may not have dealt with before. To understand the effects regarding the drugs used to induce anesthesia; it is necessary to review a few basics of pharmacology.
- What do drugs do to the body (Pharmacodynamics)?
- Any given drug has a Desired (or Primary) Effect and a Secondary (or Side) Effect to specific receptors in the body. The drug can bind with the receptors and elicit the typical mediated response and therefore be termed an agonist.
- On the other hand the drug can bind with the receptor and inhibit or prevent the expected response and be termed an antagonist. For example, the drug Morphine is targeted at specific opiate receptors in the brain that mediate the recognition of and response to pain – the primary effect is analgesia. However, opioid receptors are also located in the respiratory and vomiting centers of the brain so the secondary effect of morphine is respiratory depression, nausea and vomiting.
- What does the body do to drugs (Pharmacokinetics)?
Drugs are absorbed into the bloodstream (i.e. via IV injection or in the case of anesthetic gases forced into the respiratory tract and absorbed from the lungs) into circulation – the drug is distributed to various parts of the body. The highly perfused tissues such as the brain, heart and liver receive, in proportion, a larger amount of the total dose. They are then distributed to the receptor sites (causing desired and side effects).
Clearance or recovery from a drug is via metabolism through the liver, kidneys (excretion) or lungs (expiration).
Clearance or recovery can happen in three ways:
a) Redistribution:
- Drug is removed from the receptor, but not the body
- Drug is redistributed to other tissue and may be stored and released again at another time (many drugs are fat soluble)
- Drug is released from a storage site and can potentially be reactivated into the blood stream
b) Drug is removed from the body and metabolized:
- Drug is inactivated and removed by making it water soluble (this is called the biotransformation process)
- Metabolism occurs in the liver but to some extent can happen in the kidneys, lungs and GI tract
- Slow process and can be prolonged in a patient with liver, cardiac or renal disease
- Also affected by hypoventilation (delays excretion through the lungs), hypotension (slows circulation to clearance organs), lengthy surgery (involves the giving of more drugs – which increases clearance time), obesity (drugs that are lipid soluble are stored in the fat cells and can be redistributed) and hypothermia (slows down metabolic processes)
c) The drugs are then excreted by:
- Eliminating the drug from the body altogether
- The kidneys are the major organ of excretion although some drugs are excreted from other sites such as the lungs (gases) and the biliary tract
3. By administering a second drug that counters the effects of the first one. This drug is called an (antagonist). This works by:
- Binding to receptors without causing receptor activation
- Prevents the activating drug from stimulating the receptor (i.e. Narcan antagonizes the effects of narcotics)
Pharmacology of the Peripheral Nervous System #
Knowledge of the Peripheral Nervous System will assist you during your clinical practice in understanding:
- when a certain drug is given
- what drug (or type of drug) may be needed to maintain the patient’s homeostasis (whether you are asked to administer it or just obtain it)
- how the drugs work
or supplemental information on the pharmacology of the Peripheral Nervous System, please click on the following: SI – Review of the Peripheral Nervous System and its Effects on Pharmacology
A multi-pharmaceutical approach is used in anesthesia. By using a number of drugs with similar desired effects, a lower dose of each drug can be given. As a result, side effects associated with high doses of only one or two drugs can be avoided and the desired effects of each drug can be maximized. Each drug is selected based on the goals and sequence of anesthesia.
General Anesthesia #
General anesthesia can be described as:
“A reversible state of unconsciousness produced by drugs with sufficient depression of reflexes to allow a surgical procedure to be performed.” – Hardman & Limbird, 1996
The anesthesiologist determines the type and administration route of the anesthetic for a patient based on:
- The goal of anesthesia
- The stage of anesthesia
- Specific surgery requirements: length of surgery, need for muscle relaxation, significant blood loss expected, need for quick post-operative arousal (i.e. neurosurgery), etc.
- Unique requirements and characteristics of the patient; preexisting medical conditions, trauma, age, personal preference etc.
Let us look at the first two more closely.
Goals of General Anesthesia #
The overall goals of anesthesia are:
1.Unconsciousness, hypnosis and amnesia
- The patient will be unaware of environment during surgery and have no recall of intraoperative events
- Rapid onset, short duration drugs such as benzodiazepines (i.e. Midazolam), Propofol and barbiturates (rarely)
- Anesthetic gases such as Isoflurane, Sevoflurane and Desflurane
- Drugs used to produce unconsciousness have minimal, if any, analgesic properties
2. Analgesia – absence of painful perceptions
- Intraoperative pain control inhibits the stress response associated with the surgical procedure and will aid in postoperative recovery
- Potent short duration synthetic opioid agonists are used preoperatively and intraoperatively (i.e. Fentanyl, Sufentanil, Remifentanil)
- Longer acting drugs such as Morphine, Hydromorphone and Fentanyl may be used toward the end of the procedure and in recovery for acute pain management
3. Muscle relaxation
- Used to facilitate airway intubation; use rapid onset muscle relaxants such as Succinylcholine and Rocuronium Bromide
- Used to relax muscle tension around the operative site when indicated; may require longer-acting drugs such as Vecuronium for the surgical procedures
4. Autonomic and endocrine reflex control
- Control of fight or flight response to the stress of surgery and to some of the secondary effects of the drugs used to induce anesthesia
- Control of autonomic and endocrine activity leads to an uneventful postoperative course
Stages of General Anesthesia #
The stages of general anesthesia should not be confused with the level of anesthesia. The level of anesthesia is outlined in the Alexander’s textbook as four stages in the level of consciousness (physiologic and reflex response), once anesthetic drugs are given. The stages of anesthesia refer to the whole anesthetic experience; the process by which a patient is prepared, given anesthesia and awakened from an anesthetic. Although preoperative preparation is an important step, the stages of general anesthesia are considered to be:
- Induction
- Maintenance
- Emergence
Preoperative Preparation
Preoperative preparation by the anesthesiologist was previously discussed. This discussion involves what happens to the patient immediately before and after they enter the operating room. Preoperative preparation assists the patient in enduring the stress of surgery, decreases the risk of aspiration, controls any reflex activity prior to induction, provides analgesia and anxiety control.
- Review module on Patient Assessment
- Always project a calm, confident and respectful manner in the presence of the patient
- Ensure the patient is comfortable
- Be aware of preoperative medication administration; sedated patients cannot be unattended
- Introduce yourself to the patient and the patient to all personnel present in the OR theater
- Provide warm blankets for the patient
- Explain all nursing care to the patient
- Provide therapeutic touch and reassurance
- Keep noise to a minimum
- Many patients have a fear of needles; provide patient support during IV insertion
- Apply or assist with applying monitoring devices on patient
- Be attentive to the patient
Induction
Induction is the start of the general anesthetic to the fully anesthetized state (unconsciousness with sufficient depression of reflexes).
This phase of anesthesia places the patient in a potentially unstable condition and all health care professionals attending to the patient must pay close attention on the patient and be prepared for any untoward event.
It is desirable to reach unconsciousness as quickly as possible. Rapid onset short duration drugs (i.e. Propofol) are given to induce anesthesia in combination with a short acting opioid (i.e. Fentanyl or Sufentanil) to counteract any discomfort and related nervous system reflex activity.
Once the patient is unconscious (anesthesiologist will test for absence of eyelash reflex), the anesthesiologist will manually assist with ventilation as the patient has an unprotected airway. When the patient is sufficiently preoxygenated and muscle relaxation is adequate, intubation occurs. If the procedure is of a short duration and the patient will be in the supine position, intubation may not be necessary and a laryngeal mask may be used. For longer procedures, a short-acting or intermediate-acting muscle relaxant (i.e. Rocuronium) is given to facilitate endotracheal intubation. Intubation should occur within ninety seconds of unconsciousness.
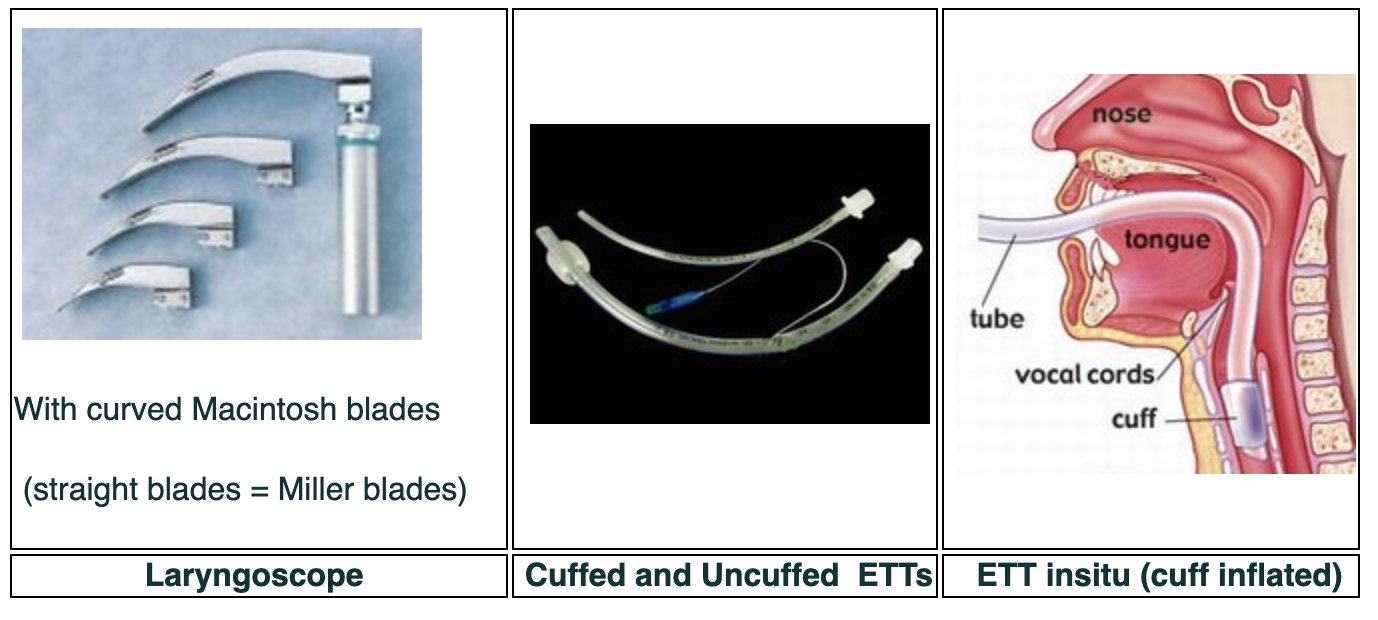
A laryngoscope is used to visualize the vocal cords. A topical local anesthetic (i.e. Lidocaine spray) may be applied to suppress any residual airway reflexes. The endotracheal tube is placed in the patient, attached to a mechanical ventilator and secured into place. Breath sounds are assessed with a stethoscope to ensure proper placement of the endotracheal tube (bilateral and equal breath sounds).
Maintenance
Maintenance occurs after intubation (airway established) then the patient is prepared for the surgical procedure. Activities that occur at this time are: urinary catheter insertion, invasive line insertion, patient positioning, surgical skin preparation and the actual surgical procedure itself.
The anesthesiologist will administer longer acting drugs are administered in the form of:
- Volatile inhalation agents (anesthetic gases) such as Isoflurane, Desflurane and Sevoflurane. These drugs come in a volatile liquid form that is placed into vaporizers attached to the anesthetic machine (vaporizes the liquid to gas) and introduces the gas into the breathing circuit where the patient inhales it. Another inhalational agent is Nitrous Oxide (a non-volatile inhalation agent). This gas is rarely used today, but can be given in adjunct with the volatile gases as it has few side effects and allows for smaller doses of the volatile agents to be given (which can have hypotensive effects).
- Long acting opioids and Propofol – given in intermittent or continuous infusions
- Long acting muscle relaxants – i.e. Pancuronium
- Drugs to counteract the side effects of surgical stimulation – such things as bleeding, visceral manipulation and vessel clamping can lead to undesirable physiological responses such as BP and HR changes.
- Be aware of the patient’s physiological status throughout the surgery
- Assist with or obtain glucometer readings for diabetic patients
- Monitor blood loss by assessing sponges and suction containers and report to anesthesiologist if excessive. Prepare for and assist with blood transfusions, if required
- Monitor temperature control settings on forced-air warming devices. Patients are vulnerable to temperature changes especially during exposure of body cavities
- Provide warm IV fluids for irrigation fluids
Emergence
Recovery from anesthesia is the also a critical time for the patient. The overall goal is restoration of all vital functions to normal parameters (ventilation, airway reflexes and hemodynamic status). The patient progresses through the following four phases of emergence from the anesthetic:
- Recovery of sensory and motor function as anesthesia depth is reduced. Anesthetic gases and drugs are stopped or tapered off thirty to forty minutes prior to the end of the surgical procedure (or sooner depending on their clearance time from the body) prior to the end of the surgical procedure (which means closure of the patient’s surgical wound). When indicated, a reversal agent is given when muscle relaxants are used. Opioids may be given to provide ongoing post-operative analgesia with adequate respiratory and hemodynamic monitoring.
- Resumption of spontaneous ventilatory control; reversal agents for opioids (Naloxone) or benzodiazepines (Flumazenil) may necessary if awakening is prolonged
- Return of airway reflexes; sufficient muscle control is restored and patient attempts to breathe
- Patient awakening: spontaneous eye opening and increasing awareness of their surroundings
Tracheal extubation is the single most critical event that the patient will experience in this phase. Emergency reintubation may be necessary if the patient is unable to maintain or control of their own airway or is not sufficiently awake to maintain their own airway prior to extubation. Some patients may be kept in a deeper state of anesthesia to avoid reflex irritation. Coughing should be avoided for these procedures (i.e. ophthalmic) and extubation will be attempted once the patient is more fully awake.
- STAY BESIDE THE PATIENT HAS BEEN EXTUBATION (extremely important) and the patient’s airway is secure (patient is able to breath on their own) and oxygen saturation is reading normal
- Keep the patient warm: hypothermia can lead to undue postoperative complications
- Reorientate the patient; they may not know where they are or what happened to them until they are fully awake
- Some patients, especially children and teenagers, can wake up suddenly (progress through the four phases rapidly) and become combative. Ensure that they do not hurt themselves on the side rails, help to reorientate them and reassure them as they waking up.
- Be prepared if there is a need to reintubate the patient; be knowledgeable of where the necessary supplies are kept
- Transport patient to the postoperative anesthetic recovery room (PAR) and give a hand-over report to PAR nurse
Types of General Anesthesia #
There are different types of general anesthesia, all result in the same end result; the patient is given anesthetic drugs (rendered unconscious) and intubated. The type of general anesthetic given is dependent on the individual patient’s needs and the duration and type of surgery. The types of general anesthesia are:
- Inhalation Technique
- Propofol is given to facilitate a rapid induction (if IV present) or patient may breathe themselves under with a volatile inhalational agent such as Sevoflurane or Desflurane, in a mixture of Nitrous oxide, Air and/or Oxygen. This is often used for children (or patient’s with needle phobias) to avoid insertion of an IV while the patient is awake. Once unconscious, one of the other types of anesthesia will be used.
- Total IV Anesthesia (TIVA)
Once was used for short cases, remote locations, radiology, where no gas scavenging system is available and office-based surgical procedures; but is now a generally used technique. Again the usual intubation drugs are given, but then short-acting drugs such as Propofol, Ketamine and Remifentanil are administered by continuous infusion. Due to the short acting nature of the drugs, when surgery is almost done the infusion is titrated off and emergence occurs quickly. Volatile inhalational gases are not used – Oxygen is always used.
- Combination
In this technique, after intubation (Propofol, muscle relaxant, and Fentanyl have been given), longer acting drugs are given in a one time dose. Drugs such as Midazolam and Fentanyl. This is usually done for shorter procedures, where the drugs are not quite worn off by the time the procedure is over, providing some postoperative pain relief. Inhalational gases may or may not be used.
Intubation Techniques and Supplies #
Intubation refers to the placement of a tube into an orifice of the body and, most commonly refers to tracheal intubation. Tracheal intubation is the placement of a flexible plastic tube into the trachea. Reasons for tracheal intubation include:
- Apnea
- Respiratory failure
- Inability to protect airway (i.e. trauma, altered gag reflex)
- Altered level of consciousness
- Maintenance of patent airway
Tracheal intubation of a patient is required following the administration of a general anesthetic and muscle relaxants. Securing the patient’s airway is paramount.
Airway Anatomy #
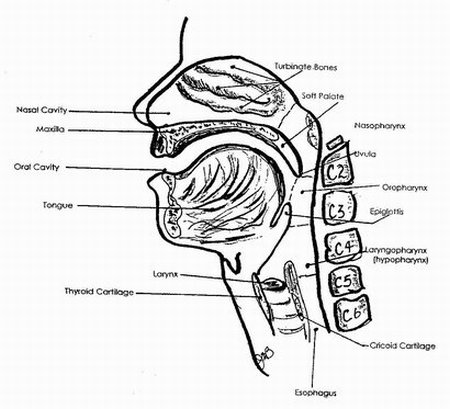
The upper airway is designed to deliver gases (O2 and CO2) to and from the lower airway (thoracic trachea, carina, mainstem bronchi and bronchioles) and into the respiratory airway (respiratory bronchioles and alveoli of the lungs) for gas exchange. The upper airway can be divided into three sections:
- Supraglottic airway: nasal and oral pharynxes and the laryngeal pharynx. The soft palate separates the nasopharynx and oropharynx (which includes the tongue, tonsils and pharyngeal muscles). The pharynx also includes the entrance to the esophagus.
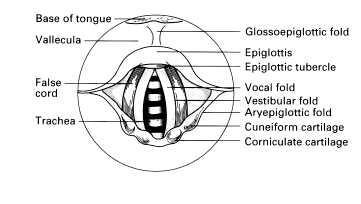
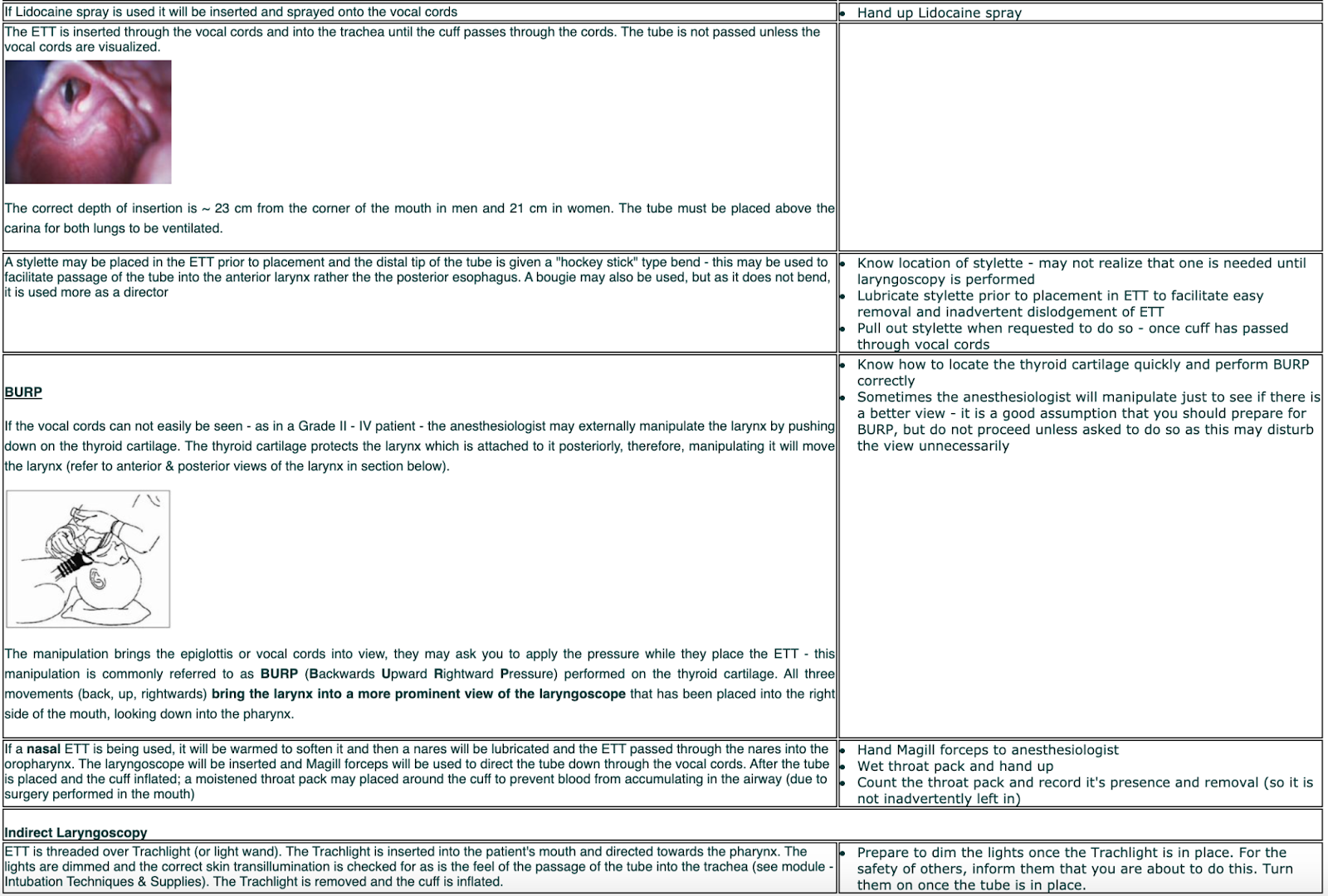
- Glottic airway: laryngeal structures. The epiglottis is located at the top of the laryngeal cavity and seals off the laryngeal inlet during swallowing. The vocal cords (or ligaments) are within the laryngeal cavity and the opening between is the glottis. The glottis is the narrowest section of the adult upper airway. The larynx is protected by the thyroid and cricoid cartilages. The cricoid cartilage is the only complete circle of cartilage in the trachea; all other cartilages are U-shaped.
- Subglottic Airway: cervical trachea. The larynx attaches to the cervical trachea (at the level of the sixth cervical vertebra). The subglottic area is about 10-15 cm to the carina (where the trachea bifurcates into the left and right mainstem bronchus). The subglottic trachea is the narrowest section of the upper airway in children.
The anesthesiologist can choose a supraglottic airway for short, simple procedures or endotracheal intubation for complex procedures that are longer or require the patient to be in certain positions.
The laryngeal mask airway (LMA) is the most common supraglottic airway.
The endotracheal tube (ETT) is the most common tracheal intubation.
For emergency situations such as laryngotracheal injury, maxillofacial trauma, inability to open the mouth or unclench the teeth, or deformities that prevent orotracheal intubation, a procedure known as cricothyroidotomy may be indicated.
- Cricothyroidotomy – an opening is made between the cricoid and thyroid cartilages into the trachea. An anesthesiologist may carry a large bore IV cannula and adapter in preparation for this emergency procedure.

- Tracheostomy – also used for long term respiratory support. Performed by an ENT surgeon.
The patient who is to undergo a general anesthetic has their airway assessed preoperatively by the anesthesiologist. Based on their findings and on the type of surgery the patient is to have, the anesthesiologist determines which method of airway control is required and by what means the airway can be placed quickly and accurately.
Airway Assessment #
When a patient requires a general anesthetic, the anesthesiologist will perform a number of assessment techniques to determine how difficult it will be to see the patient’s glottic airway (i.e. observation, asking the patient to open their mouth, etc.).
The anesthesiologist determines which method of airway control is required for the patient based on a physical asessment and the specific surgery that is planned. The best way to assess an airway is by visual inspection via direct laryngoscopy after the patient is sedated. The anesthesiologist and perioperative team must be prepared to re-gain airway control if the airway of the sedated patient is compromised during the laryngoscopy.
Supraglottic Airway #
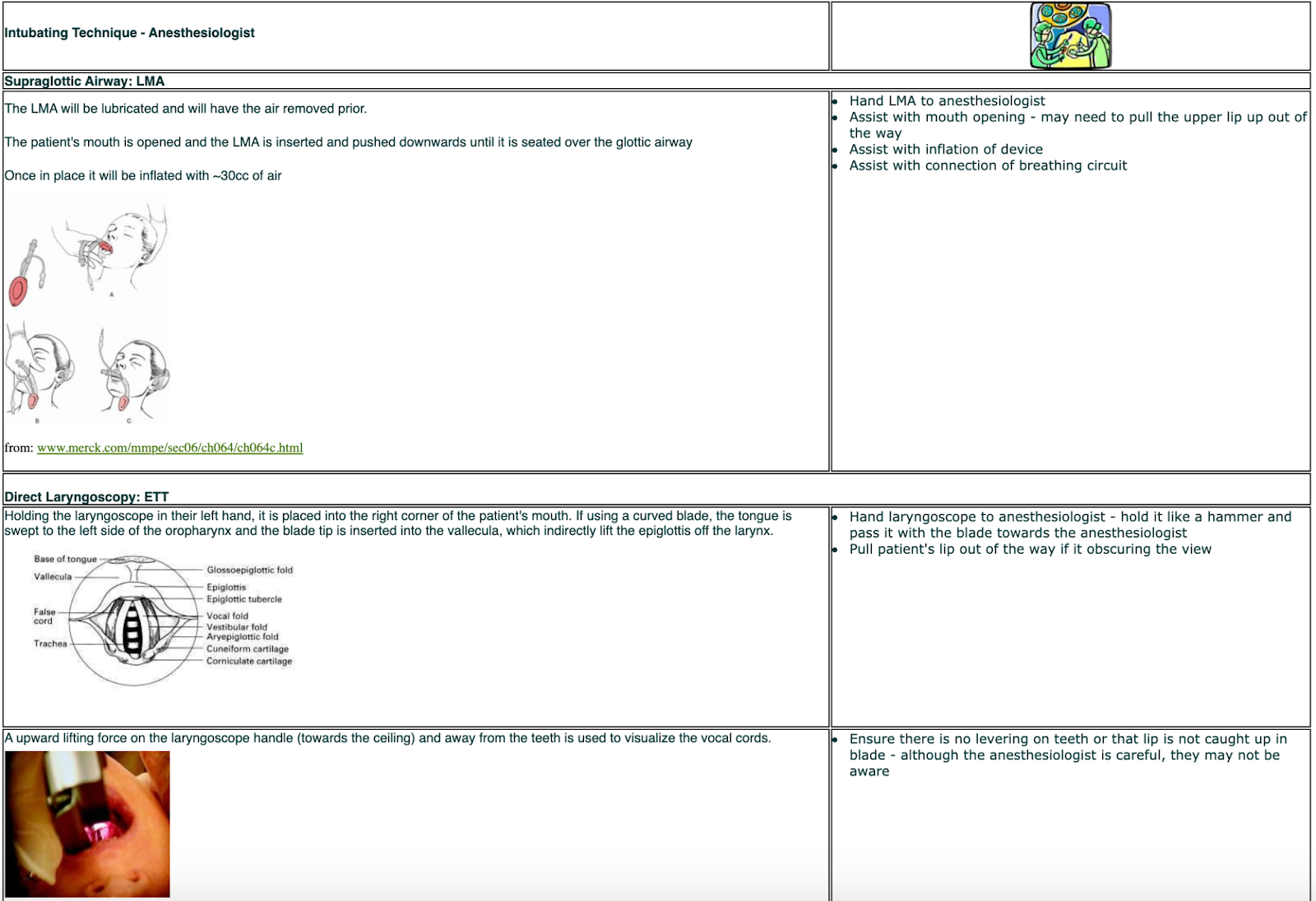
The Laryngeal Mask Airway (LMA) is usually used for relatively short procedures, for patients in the supine position only and who are at a low risk for aspiration. LMA’s can be used for spontaneous (patient is sedated but breathing on their own) or mechanical ventilation.
The LMA may also be used as a temporary measure to secure the airway until an ETT can be placed. A laryngoscope is not required to insert an LMA as they fit over top of the larynx. Since an LMA rests in the supraglottic area, behind the glottis (covering the larynx), they do not provide a sufficient seal against the regurgitation of stomach contents (i.e. not used for patient’s with reflux disease). For this reason, an LMA is considered a patent airway as opposed to a secure airway. The LMA is routinely used for shorter procedures. The LMA has a cuff that is partially deflated before insertion and fully inflated once in place. LMA’s require a syringe with approximately 30cc of air to inflate.
Types of LMAs:
1 . Classic LMA – either come with wire rings (making it more flexible and sturdier) in lumen or without.
Reusable or Single use
Come in a variety of sizes (for adults: #3, 4 or 5)
Types: Regular (Classic Style) or flexible (has wire inside for bending)


Classic Classic-flexible
2. Proseal LMA – Double lumen: Back lumen go directly down to the trachea and front lumen use to pass a suction catheter or NG tube into the esophagus.


3. Fastrach LMA – used in difficult intubation cases. The Fasttrach LMA has a “trap door” at the end which allows an airway to be established and also allows an endotracheal tube to pass down its center lumen.

Direct Laryngoscopy #
Direct Laryngoscopy is achieved with the use of a laryngoscope (for visualization) and an endotracheal tube (ETT). The ETT comes in a variety of diameters, measured in French (Fr.) units.
The ETT will often be cut to a length of ~ 28 cm as this is a sufficient length for the tube to sit above the carina and have a few inches sticking out of the mouth to attach to the ventilation tubing. The ideal ETT placement length (~2 cm above the carina to teeth) is roughly 21 cm in women and 23 cm in men. The diameter of the tube (internal diameter) should be a 7.0 to 7.5 Fr. tube for women and a 7.5 to 8.0 Fr. tube for men and for children it should be roughly the diameter of their little finger or nostril.
The ETT can be cuffed (with a balloon) or uncuffed. Cuffed ETT are used to seal off the airway from any aspirate and they provide a secure airway. Uncuffed tubes are only used in small children (usually 6 years old and under, depending on the size of the child) as a child’s airway is narrow it may not be able to accommodate the pressure of a cuffed ETT.
Oral Tubes
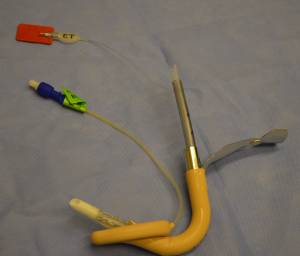
The ETT is passed through the mouth, larynx, and vocal cords and into the trachea. The ETT balloon is then inflated near the distal tip of the tube. The balloon helps to secure the ETT in place and protects the airway and lungs from aspiration of blood, vomit, and secretions (from esophageal regurgitation). The ETT may be straight or angled downwards. Angled tubes are called oral Rae tubes and are used for surgeries in the facial area (i.e. nose or ophthalmic procedures). The angle keeps the ETT from encroaching into the surgical area.



Uncuffed ETT —————————-Cuffed straight (Murphy)——————ETT Oral Rae tube
Nasal Tubes
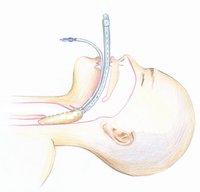
Another method of tracheal intubation is intranasal. The ETT is passed through the nose into the oropharynx, larynx, vocal cords and into the trachea. This intubation method is used for surgical interventions that take place in and around the mouth. These ETT are often warmed (in a bottle of warm water or saline) to soften them prior to nasal insertion. The laryngoscope is placed orally and as the ETT is passed and viewed in the oropharynx. A forcep (called a Magill) is used to advance the tube downward through the glottis.



Nasal ETT————————–Checking placement of nasal ETT——Magill forcep
Endobronchial tubes
Endobronchial tubes (EBT) are used for surgery of the lungs. EBT have two lumens; one sits in the trachea, above the carina, and the other sits in the right or left main stem bronchus.
One lung ventilation (OLV) is the term used in thoracic anesthesia to describe the ability to ventilate one of a patient’s lungs, allowing the other one to collapse. Most lung resections and esophageal surgeries can be done without collapsing a lung by ventilating the patient with smaller tidal volumes and the surgeon using a retractor. However, if the surgeon is not able to operate with the lung inflated, or if the tumor is technically difficult to resect, OLV will be required.
The EBT are designed to sit in either the left main bronchus or the right main bronchus. Either EBT can be used to ventilate either lung depending on which lumen is clamped; however, a left-sided EBT is usually used as it is easier to position. The right-sided EBT is more difficult to position because the right upper lobe comes off the right main bronchus at variable distances from the carina (each person is different). If the end of the tube is not properly aligned with the entrance to the right upper lobe, the lobe will not be ventilated.
By clamping one lumen of an endobronchial tube, it will occlude ventilation to the lung on that side and the lung will deflate. If one lumen is clamped, ventilation can be continued through the other lumen (to the other lung). EBT come in sizes 26 to 41 French gauge (37-39 Fr. is the usual size for a female and 39-41 Fr. for a male).
After placement of an endobronchial tube, the anesthesiologist will place a fiberoptic bronchoscope down the center of the EBT to visually confirm correct placement of the tube in the bronchus.


Endobronchial tube———————————-Left endobronchial tube insitu
Indirect Laryngoscopy #
Indirect laryngoscopy is achieved by the use of a lighted stylette. Lighted stylettes rely upon transillumination of the anterior neck tissues to guide laryngeal placement. A well-circumscribed glow indicates tracheal intubation, whereas a diffuse glow is seen with esophageal placement. A lighted stylette is used for a patient:
- With limited capacity to open their mouth or reduced neck movement
- who are difficult to intubate (Grade 3-4) or had previous failed intubation
- who have a bloody airway
The lighted stylette is contraindicated in patients with anatomic abnormalities of the upper airway or pharyngeal masses.
The advantages of a lighted stylette are:
- It is less stimulating than direct laryngoscopy
- It does not require visualization of the larynx
- It can be used intra-nasally
- It is a portable and inexpensive device.
The disadvantages of a lighted stylette are:
- It is a blind technique
- It is more difficult to view the light in patient’s with dark skin or scarring
- It requires a darkened environment.
The ETT is placed over a stylette that has a light source attached. This stylette is placed into the patient’s mouth and advanced down into the oropharynx. The OR room lights are dimmed, as this increases the contrast allowing the light to be seen through the patient’s skin. The anesthesiologist will proceed “by feel” and the location of the light (central on the neck over the trachea) to advance the stylette through the glottis and into the trachea. Once the anesthesiologist feels the stylette is in the right location, the ETT will be slid downwards off the stylette into position; the stylet is removed, leaving the ETT behind. The ETT cuff is inflated.



Light wand——-Trachlight® – upper one has stylette attached & ETT threaded on —-Trachlight® insertion (will sequence through stages of illumination)
Fiberoptic Intubation #
A flexible endoscope (bronchoscope) is used to visualize the vocal cords when the anesthesiologist is unable to do so with a regular laryngoscope. The “scope” is thread through the inside of the ETT and then both are inserted via the nose or mouth and passed through the vocal cords into the trachea. Once the ETT is in place and secured, the bronchoscope is carefully removed. A flexible bronchoscope may also be used to check ET tube placement.
A fiberoptic intubation is indicated in emergency situations or when other attempts at laryngoscopy have failed. It may also be used when a patient is known to have a difficult airway. In this situation, the fiberoptic intubation is done when the patient is awake. This procedure is called an “awake intubation”.
An awake intubation is indicated in the following situations:
- The patient is known to have a difficult airway (i.e. Ankylosing spondylitis, previous cervical fusion surgery)
- The patient has had previous failed intubation attempts.
- The patient has a potentially unstable cervical spine (i.e. cervical trauma, rheumatoid arthritis)
Fiberoptic intubation is achieved by using a variety of types of topical anesthetics to freeze the vocal cords and diminish the gag reflex (i.e. Lidocaine mouthwash, sprays, tracheal injection). The patient is also given a mild sedative to relieve anxiety and discomfort, yet allowing them to maintain a spontaneous airway. (This process may take approximately 15 to 20 minutes).
When an adequate level of topical anesthesia is achieved, a flexible endoscope (with an ETT threaded over the end) is used to visualize the vocal cords. The scope is inserted into the mouth (more common than the nasal route) and passed through the vocal cords into the trachea. The ETT is then directed down over the scope and into the trachea. The scope allows for suctioning of secretions and confirms definitive placement of the ETT. Once the ETT is in place, the scope is removed, the cuff is inflated and secured. Anesthetic drugs are immediately administered once the airway is in place and secured.
Use of a fiberoptic scope to place an ETT tube via the nasal route
Additional Intubation Supplies #
In addition to the laryngoscope and ET tubes, the following supplies may be required for airway management:
1. Magill forceps
2. Bougies
3. Stylettes
4. Oral airway: used to keep the patient’s tongue from obstructing the airway during preoxygenation prior to intubation (sized by # i.e. #3).

To choose the proper size oral airway, hold the airway against the side of the patient’s face – it should extend from the corner of the patient’s mouth to the angle of the jaw (below the ear lobe).
5. Nasal airway: a nasal airway may be used instead of an oral airway (sized in French). It is more often used postoperatively.

6. Breathing Circuit: used to manually ventilate the patient (until end Tidal O2 is about 80%) and to preoxygenate prior to intubation. After preoxygenation, the patient will undergo an apneic period during the intubation. The intubating mask is attached to anesthetic tubing, which attaches to the anesthetic machine. A filter is placed at the expiratory end of the tubing to prevent any infectious matter from entering the anesthetic circuit. The rebreathing bag is a reservoir filled with oxygen that the anesthesiologist will use to “bag” the patient during manual ventilation. Squeezing the bag forces oxygen through the inspiratory end of the anesthetic tubing and into the patient’s lungs. After intubation, the anesthetic tubing is connected to the ETT.



Sizes of intubating masks—– (sized by # i.e. #3)–Anesthetic circuit———–tubing, mask & rebreathing bag Filters
7. Lidocaine spray: given to prevent larygospasm and numb vocal cords as the ETT passes. The spray comes in a prefilled syringe (i.e. Laryngojet) or as an aerosol spray with disposable nozzle.
8. Syringe: a 10-20 cc syringe is necessary to inflate the cuff of the ETT tube a larger syringe maybe used for an LMA.
9. Tape or ties: used to secure the ETT
10. Lubricating jelly: used to ensure easy removal of the stylette from the lumen of the ETT or for inserting the LMA (less mucosal trauma).
Difficult Intubation versus Awake Intubation #
Difficult Intubation
Some patients may be difficult to intubate and require different intubation techniques for a variety of reasons (i.e. short neck, large tongue, anterior larynx, cervical arthritis, etc). The anesthesiologist may initially start with direct laryngoscopy, then progress to the following items to assist with a difficult intubation:
1. Stylette – A stylette is a bendable metal guide coated with plastic that is inserted inside the ETT. The stylette is used to shape the ETT into a more pronounced curvature so the ETT can be passed through the vocal cords. The amount of bend used will depend on the view of the larynx (i.e. used for patient’s whose larynx is situated more anterior).


Stylette——————————ETT with stylette insitu
2. Glideoscope – The anesthesiologist may also use a video assisted laryngoscope called a Glidescope®.


- The anesthesiologist may also request the nurse’s assistance with laryngeal manipulation to push the larynx into view, called BURP (to be discussed in the next module).
3. Indirect Laryngoscope
4. Bougie – a bougie is a long plastic stylette (may be soft and flexible or semi-rigid) that is passed orally through the glottis. Then a ETT is threaded over top of the bougie and passed down the bougie’s length into place. Due to the bougies narrow diameter, the ETT can be easily threaded over it. A bougie can also be used to exchange an ETT that is already in place for one of a different size. The bougie is inserted inside the lumen of the existing tube and once in place, the old ETT is removed and a new ETT threaded down to replace the original one. This is especially helpful in an edematous airway, where reintubation may be difficult.

5. Flexible fiberoptic bronchoscope – as described above.
Awake intubation
An “awake intubation” is also known as a difficult intubation. An “awake intubation” is utilized when a patient is known to have a difficult airway. Instead of attempting any other intubation method, the patient is kept awake and an attempt is made to intubate them with the fiberoptic bronchoscope (as outlined in the preceding section).
To summarize the difference: an awake intubation is always a difficult intubation, but a difficult intubation may not always require an awake intubation.
Pharmacology of Muscle Relaxants #
Muscle relaxants are used to facilitate intubation and provide the relaxation of muscle tension for abdominal and some orthopedic surgeries. In the postoperative recovery area, they are used to facilitate ventilation management on intubated critically ill patients. The muscles that are affected by these drugs are mainly the skeletal muscles, with cardiac and smooth muscles not being affected. This category of drugs are sometimes called neuromuscular blocking agents, based on their pharmacokinetic action on the neuromuscular junction of the peripheral nervous system (PNS) – somatic system – of skeletal muscles.
Acetycholine is the main neurotransmitter of the fibers of the PNS. Acetylcholine binds to the post-synaptic nicotinic (skeletal muscle) receptors at the target organ/ muscle.
A muscle contraction begins when an impulse arrives at the motor nerve’s (or motoneuron) terminus: the neuromuscular junction. The impulse causes the release of Acetylcholine (Ach). Acetylcholine travels across the synaptic cleft carrying the message (transmission impulse) and binds to the Ach receptors located at the motor end plate. When these receptors sites are occupied by Ach, the muscle fiber depolarizes and muscle contraction occurs (pictured below).
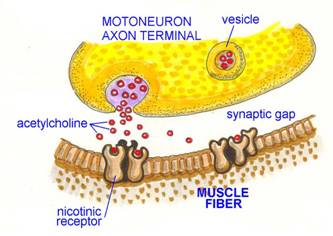
Neuromuscular junction of skeletal muscle (nicotinic receptor sites)
Termination of muscle contraction occurs when the enzyme Acetylcholinesterase breaks down the Ach thus preventing a sustained muscle contraction – this process happens very quickly.
Neuromuscular blocking agents act in the neuromuscular junction by interfering with or binding with the nicotinic receptor sites of skeletal muscle cells, that is to say, they do not allow the Ach to bind to the receptors, and thus prevent any transmission signal for the muscle to contract.
The muscle relaxants used during surgery work in one of two ways; they are either depolarizing or nondepolarizing
Depolarizing Muscle Relaxants #
Depolarizing muscle relaxants (DMR) have a brief duration of action (5-10 minutes) and a rapid onset (30-40 seconds). Succinylcholine is the only one still widely used; mainly for rapid sequence induction (a technique used to prevent regurgitation in certain patient populations) or when muscle relaxation is required for a very short period of time. As it is the main DMR used today, we will use Succinylcholine and DMR interchangeably.
Succinylcholine mimics the action of the neurotransmittor Acetylcholine at the neuromuscular junction. Succinylcholine so closely resembles Ach that it fools the receptors at the motor end plate and causes the muscle to contract (depolarize). This depolarization can be witnessed as a general wave of muscular contraction (fasciculation). Succinylcholine is not broken down as quickly as Ach, so it will remain attached to the receptor sites preventing any further depolarizations (contractions).
Succinylcholine is broken down by hydrolysis by pseudocholinesterase enzymes, which takes about 5-10 minutes. There is NO REVERSAL agent/drug that can be given to inactivate Succinylcholine – it can only be inactivated by metabolism.
Succinylcholines primary effect is muscle relaxation, it has no effect on consciousness or analgesia. Therefore if the muscle relaxant is given too soon, the patient will be unable to breathe and be aware of it. This could be also be true of the nondepolarizing muscle relaxants, but as their onset is not as swift as Succinylcholine it is not usually a problem.
Secondary effects of Succinylcholine include:
- The initial muscle fasciculations can cause postoperative pain and muscle aches. This is most often noted in patients who have short procedures and are discharged the same day. The fasciculations may also cause increases in intraocular, intracranial and intragastric pressures. Sometimes a small dose of nondepolarizing muscle relaxant is given to prevent the fasciculations.
- Succinylcholine is a known trigger for patients with a condition called Malignant Hyperthermia. Its use should be avoided in these patients.
- Patients with pseudocholinesterase deficiency are missing the enzyme that hydrolyses succinylcholine, which makes for a prolonged muscle paralysis.
- Patients with Myasthenia gravis (an autoimmune disorder in which antibodies block Ach at the post-synaptic neuromuscular junction) should not be given depolarizing muscle relaxants. These patients should be given nondepolarizing agents. If Succinylcholine is given to these patients then postoperative ventilation will be required until the Succinylcholine is eventually eliminated from the body.
- Succinylcholine is contraindicated in patients with multiple trauma where spinal cord injury is suspected, major burn injury, neuromuscular diseases (i.e. Muscular Dystrophy). This is because in these patient populations, Succinylcholine can precipitate a massive outflow of potassium from the skeletal muscle cell into the plasma resulting in hyperkalemia and possible cardiac arrest.
- In the pediatric population, undiagnosed Duchenne’s muscular dystrophy can lead to cardiac arrest following the administration of Succinylcholine.
Non-depolarizing Muscle Relaxants #
Non-depolarizing muscle relaxants (NDMR) compete with Acetylcholine at the receptor sites. If there is more NDMR than Acetylcholine, then they will win out and bind to the receptor sites and prevent depolarization which results in a flaccid paralysis. They will continue to bind to the receptor sites until a reversal agent is given or they are eventually metabolized. NDMRs have an intermediate to long onset (1-5 minutes) and a long duration (20-60 minutes). Some common NDMRs are Rocuronium bromide, Vecuronium, Cisatracurium, Mivacurium and less commonly Pancuronium. Rocuronium has the quickest onset (< 60 seconds) and is the drug of choice for intubation (replacing Succinylcholine). Cisatracurium is metabolized differently and so may be used in patients with liver or renal failure.
A peripheral nerve stimulator is used to determine when the NDMR is wearing off, if the twitch is strong, then more of the drug is given. Of course, the anesthesiologist will determine the dose depending on the length of the procedure remaining. If there is too much NDMR in the patient’s system, it can and must be reversed by a Reversal Agent (e.g. Neostigmine).
Certain drugs and conditions can potentiate the action of NDMRs. Drugs such as Tetracycline, Lidocaine, Inderal, “mycin” drugs like Gentamycin, and most general anesthetic drugs; and conditions such as acidosis, hypo- kalemia & natremia, hyer- carbia & magnesia, hypothermia and neuromuscular disorders.
Reversal agents
Reversal agents are antagonist drugs. They are called Anticholinesterase drugs and work by inactivating Acetylcholinesterase. As previously mentioned, Acetylcholinesterase breaks down Acetylcholine. The Anticholinesterase drugs prevent the breakdown of Acetylcholine, allowing it to build up and therefore win over the NDMRs in competing for the receptor sites and once again allow for the normal transmission of impulses that result in depolarization of the muscle cell (contraction). Some common reversal agents are Edrophonium chloride and Neostigmine. Another drug in this category is Pyridostigmine, which is most commonly used as a medication to treat Myasthenia gravis.
The desired target of reversal agents is the nicotinic receptors of the neuromuscular junction, but unfortunately they are not as specific as the muscle relaxant drugs themselves, in that they also target the muscarinic receptors. Thus producing the muscarinic effects of the PNS such as bradycardia, bronchoconstriction, ↑ peristalsis, ↑ salivation & pulmonary secretions and coronary artery constriction, to name a few. Therefore in order to counter these cholinergic effects, it is often necessary to administer an anticholinergic drug such as Atropine or Glycopyrolate (has less CNS effects than Atropine) along with the reversal agent.
Responsibility of nurses
- Be aware if your patient has Myasthenia gravis, other muscular disorders or Malignant hyperthermia.
- Be aware of when Succinylcholine will be used – expect fasciculations to some degree and so ensure patient has safety straps in place on legs and that arms are secure. Although the fasciculations have the appearance of slight twitching, it is possible for a loosely tucked arm to move.
- Provide a nerve stimulator to test for when muscle relaxants are wearing off
- Be prepared to wait for extubation of patient until muscle relaxant is worn off or reversal agent has taken effect – you may be asked to have the patient squeeze your hand – if the grip is fairly strong then the patient will be extubated
- Be prepared to take the patient to PAR with the endotracheal tube insitu, if reversal of muscle relaxation is prolonged – prepare Ambu-bag and inform PAR (may need to prepare ventilator)
- Know the difference between the muscle relaxants that can and cannot be reversed
- Know the patient populations susceptible to DMR reactions
- Prevent hypothermia
Assisting with Intubation #
Anesthetizing the patient and keeping them safe while under anesthesia is a team effort. It is the perioperative nurse’s responsibility to be familiar with the steps in administering a general anesthetic and how to best assist the anesthesiologist.
Preintubation #
After the anesthesiologist has seen the patient in the preoperative holding area (to introduce themselves, answer any questions, do a preoperative assessment or review a prior preoperative visit assessment), they will return to the operating room to do a thorough check of the anesthetic machine to ensure it is in working order. They will then begin to draw up necessary drugs and prepare for any IV or invasive line insertion and prepare the intubating supplies. For an intubation where difficulties are not anticipated, these supplies would include:
- Laryngoscope
- Oral Airway
- Yankauer (tonsil) suction tip and tubing
- Endotracheal tube (oral, oral Rae® or nasal) – if using a cuffed tube, ensure that the balloon inflates and deflates or LMA
- 10-20cc syringe (“cuff puff” – to inflate ETT balloon)
- Intubating mask, rebreathing bag and anesthetic tubing (with filter) affixed to anesthetic gas machine
- Magill forceps
- Stylette (optional) – if used the anesthesiologist will lubricate stylette and insert it into the ETT – desired bend is created
- Lidocaine spray (Laryngojet® or aerosol with nozzle)
At this time the perioperative nurse should:
- Discuss with the anesthesiologist what their plan is re: intubation, invasive lines, regional anesthesia, patient concerns & condition
- Ensure that the OR is ready for the patient to enter the room
- The OR should have the correct bed for the surgery – know how it can be placed in trendelenberg
- Anesthetic machine breathing circuit is assembled, suction tubing and tip present and in working order – although the anesthesiologist is responsible for assembly; it is also the perioperative nurse who should make note of any obviously missing supplies
- Complete a pre-operative check of the patient before the patient goes into the operating room (allergies, NPO status, patient ID, lab work, etc)
- Provide support and reassurance to the patient and family members. Answer questions.
- Supply patient with warm blankets and apply safety strap. Attach armboards to OR table.
- Anesthetic monitoring equipment is turned on
- Attach ECG, BP cuff (obtain first reading) and pulse oximeter to patient
- Assist with insertion of IV
- Assist with insertion of any invasive lines – most likely these will be inserted after intubation, but at times unstable cardiac patients may require arterial line placement prior to administration of a general anesthetic
- Assist with insertion of epidural or spinal anesthetic – these procedures will be discussed in the next section. At times these will be the primary method of anesthesia, but often they will be used for postoperative pain control and a general anesthetic will also be given.
- Assist the anesthesiologist in applying the appropriate number of pillows under the patient’s head and shoulders to assist with appropriate head positioning during intubation (may ask for a TROOP pillow)
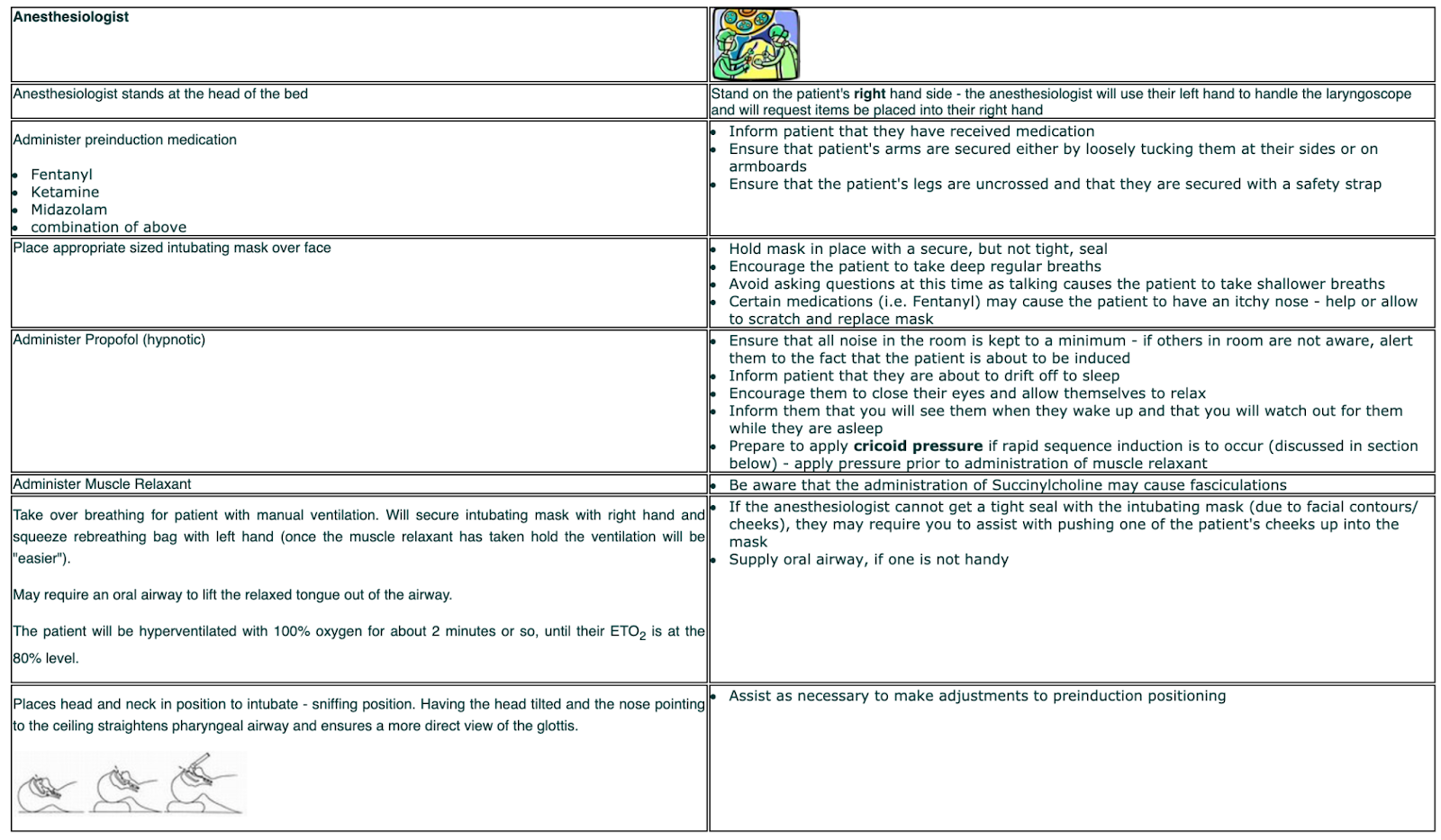
- Adjust OR table to appropriate height for the anesthesiologist to intubate – they will always stand at the patient’s head and you will stand on the right hand side of the patient near their head
Intubation #
The order of events for the induction phase of general anesthesia and nursing responsibilities usually proceed as follows:
The next step is the insertion of the LMA or ET tube, the steps for this are as follows:
Fiberoptic Intubation – refer to the module – Intubation Techniques & Supplies. The technique is outlined in the module and basic information is given. As this is an intubation method for difficult intubations or emergency situations and for awake intubations, it is an advanced technique that will be demonstrated in the clinical setting.
After ETT placement, the anesthesiologist will manually ventilate and verify correct tracheal position by at least two clinical methods – end tidal C02 and auscultation. The ETT is inspected for condensation (a sign of exhalation) and the capanograph is noted for presence of an end tidal CO2 reading. The lungs are auscultated bilaterally for breath sounds, the epigastrium for absence of gastric sounds and the chest is inspected for equal bilateral expansion. A loud gurgling sound on manual ventilation indicates esophageal placement – reintubation is required.
Securing the Airway & Inflating the Cuff #
ETT
Once the ETT is in place, it will be the nurse’s responsibility to hold it in place until it can be taped or tied into place. For patient’s with facial hair the preference is to use ties.
The anesthesiologist will connect the anesthetic breathing circuit to the ETT, turn on the mechanical ventilator and adjust the flow of oxygen and possibly volatile gases – therefore it may be a minute before the airway is secured. When holding the ETT, hold it at the point where it exits the patient’s mouth, resting your hand on their chin. The objective is to ensure it does not dislodge and that it remains at the mark it was placed at and does not move up or down.
When a cuffed ETT is used, it is necessary to inflate the cuff as soon as the ETT is in place – this can be done while you are holding the ETT in place, awaiting taping or tying. If the cuff is not inflated the airway is left unprotected and at risk for gastric aspirations. The cuff should be inflated to the point that there is no air leakage past the cuff upon expiration – too much air in the cuff can result in tracheal necrosis.
A preinduction preparation of the ETT should be to attach the syringe to the cuff. Once the ETT is in place, inject approximately 3cc of air – the anesthesiologist will then be manually ventilating the patient to ensure placement. If there is an air leak, it will be heard as a “rasping” sound – continue to inject air until the sound is no longer heard. Some will say to just inflate until the cuff port balloon is full and soft to the touch; this is a subjective finding and although it indicates that there is air in the cuff it is not completely indicative of the pressure of the cuff.
 Cuffed ETT – note blue cuff port balloon #
Cuffed ETT – note blue cuff port balloon #
LMA
Once the LMA is in place the anesthesiologist will inflate the device with approximately 30cc of air and then secure it to the breathing circuit. It may or may not be taped. The mechanical ventilator may or may not be used, depending on whether the patient is left to breathe spontaneously under heavy sedation rather than a full general anesthetic.
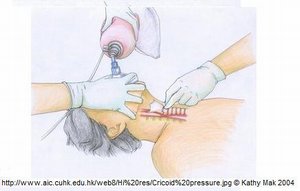
Rapid Sequence Induction #
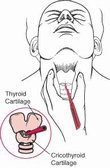
Patient’s at high risk for aspiration (pregnant women, < 6 hours NPO, esophageal reflux disease, obese, trauma, etc) will require a rapid sequence induction. This is a technique whereby the cricoid cartilage is compressed to occlude the esophagus – this is called cricoid pressure. Cricoid pressure is contraindicated in patient’s who are actively vomiting as the occlusion could cause esophageal rupture.The larynx consists of five cartilagenous rings the two most common are the thyroid, which you will recognize as the adam’s apple and the cricoid directly below. The cricoid is the only full circle cartilaginous ring therefore when pressure is exerted on the anterior side of the cartilage it presses toward the posterior section of the cartilage, effectively occluding the esophagus behind it.
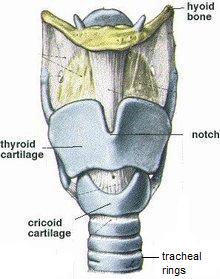
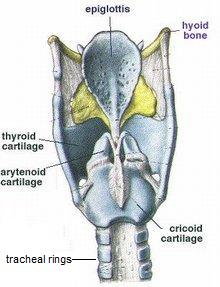
Anterior view of larynx Posterior view of larynx
To locate the cricoid cartilage: place your thumb and index finger on either side of your larynx; find your adam’s apple; slide your fingers down until you feel a small space; continue moving downwards until you feel the next ring of cartilage – that is the cricoid cartilage. The pressure you exert should begin just as the patient is falling asleep and should be kept at a constant level until the ET tube is inserted, the cuff is blown up and the anesthesiologist has checked tube placement (and tells you to stop – ask prior to releasing pressure). How do you judge the correct amount of pressure to apply? Some say to push down on the bridge of your nose until it hurts – that’s the amount of pressure you apply to the cricoid ring; or scientifically it is suggested that 30 newtons of force (~7lbs). Both of these are hard to judge and subjective, therefore, one should push quite firmly and practice on specially designed mannequins to become used to the amount of force required. Try to push with the pads of your fingertips and keep fingernails short – you may leave a temporary nail imprint. Does it hurt the patient? Surprisingly the patient does not find this pressure uncomfortable and will not try to pull away.
The steps in a rapid sequence induction are as follows: the induction agent and muscle relaxant are given; cricoid pressure is applied; the ET tube is inserted and cuff is blown up (the syringe for blowing up the cuff should already be attached to the tube); placement of the ET tube is confirmed; and then the cricoid pressure is released. No matter what is happening, do not release the pressure, there are other individuals that can perform any required tasks away from the patient that the anesthesiologist requires – when applying cricoid pressure for rapid sequence induction that is your main focus (your other hand can be used to pass the ETT if it is within reach).
Cricoid pressure vs BURP
A final note – Cricoid pressure is not BURP. They are performed for different reasons and to different cartilages. They are not interchangeable. If the anesthesiologist has difficulty viewing the larynx and requires BURP (on the thyroid cartilage), then once the ETT is in place, the pressure can be removed.
For cricoid pressure, it will be planned and announced ahead of time if a rapid sequence induction is required. The pressure will be applied (to the cricoid cartilage) as drugs are being administered and the pressure will be maintained until the ETT is in place, placement has been checked and the anesthesiologist is satisfied the airway is safe. The anesthesiologist will tell you when the pressure can safely be released.
What does this all look like? #
Watch the following video – it is a review of the above information put into practice:
Regional Anesthesia #
Regional anesthesia is achieved by the temporary interruption of the transmission of motor and sensory nerve impulses to and from a specific area or region of the body. Regional anesthesia produces analgesia and muscle relaxation (two of the goals of anesthesia) without altering the patient’s level of consciousness. General anesthesia requires total body anesthesia, whereas regional anesthesia produces anesthesia that is selective to the surgical site.
Local anesthetic drugs are injected in close proximity to selected nerves and produce anesthesia in the region of injection. Depending on the dose, the drug provides absence of sensation (anesthesia) and absence of pain without disruption of other sensory modalities (analgesia). The patient will also receive an anxiolytic drug (i.e. Midazolam or Propofol) in sub-anesthetic doses to relieve anxiety. Opioid analgesics may also be administered to supplement pain management.
Regional anesthesia involves a number of techniques and are classified according to the site where the local anesthetic is injected. The types of regional anesthesia to be discussed are:
- Topical and Infiltration
- Peripheral nerve blocks
- Intravenous Bier block
- Neuroaxial (Central) blocks: spinal and epidural anesthesia
Each of these techniques will be discussed in the following modules.
Local Anesthetic Drugs #
The two categories of local anesthetic agents are:
- Aminoesters: Procaine, Chloroprocaine, Tetracaine
- Aminoamides: Lidocaine (Xylocaine), Prilocaine, Bupivacaine (Marcaine), Mepivacaine, Ropivacaine
The main differences between the two are that aminoamides are cleared by the liver and aminoesters are inactivated in the plasma by cholinesterases; and that aminoesters appear to be more allergenic than amides (rare true allergic reactions).
The most commonly used drugs for anesthetic injection are Lidocaine, Bupivacaine, Ropivacaine and Chloroprocaine.
The choice of drug is based on a number of factors, but the main reasons are:
- Duration of the surgical procedure in relation to the duration of the drug; not a contraindication for epidural catheter placement
- Regional technique selected
- Surgical procedure requirements (i.e. more sensory than motor blockade)
- Location of surgical procedure; any procedure performed above the nipple line is not conducive to a central nerve block
- Potential for systemic toxicity; high in intravenous Bier blocks
- Whether regional anesthesia is being used for intraoperative purposes or postoperative pain control
- The addition of opoids (Hydromorphone or Fentanyl) to enhance the duration and analgesia for central nerve blocks
- The addition of a vasoconstrictor (Epinephrine, usually shortened to Epi) may be used for local injection to minimize the bleeding of tissue during the surgical procedure and increase it’s duration of action
Characteristics of commonly used drugs (Note: this information is for understanding only):
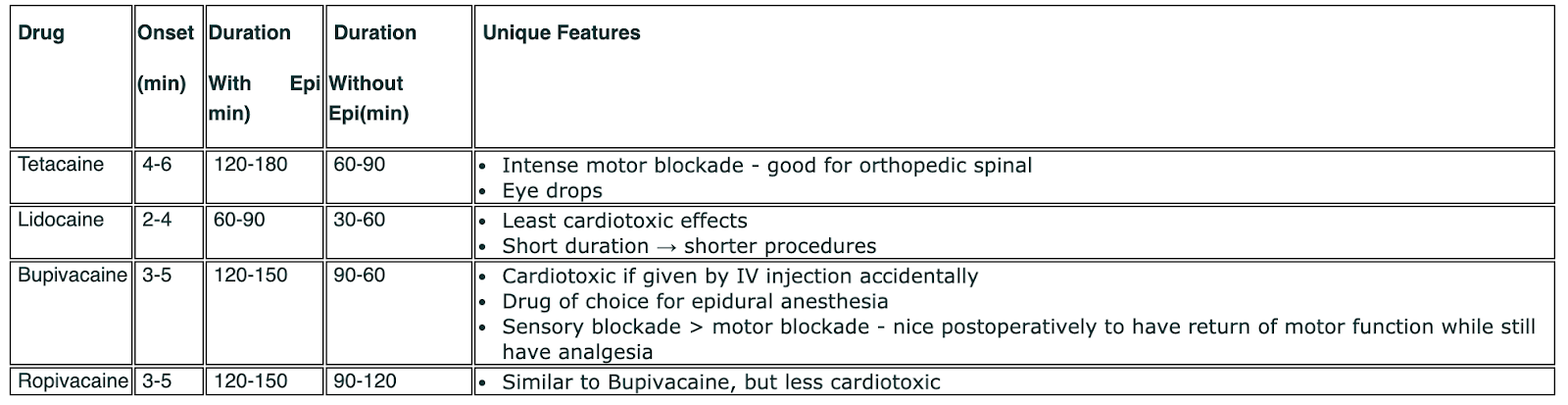
The special pharmacological properties that certain local anesthetics possess will be discussed in relation to each regional technique.
Topical and Infiltration Anesthesia #
Topical and Infiltration Anesthesia #
Topical and infiltration anesthesia are often referred to as local anesthesia. The patient is generally awake or slightly sedated during this type of anesthetic. It is important to keep noise to a minimum and ensure that conversation is appropriate and confidential.
Topical Anesthesia #
A local anesthetic may be applied directly to the surface of an area requiring desensitization for a short period of time. Examples include:
- Lidocaine spray or gel applied to the mucous membranes of the respiratory tract prior to intubation (i.e. awake intubation)
- Tetracaine drops used for short examinations of the eye
- Emla cream applied to the skin for painful intravenous insertions
Responsibility of nurses:
The main nursing responsibility surrounding topical anesthesia are:
- Providing the the drugs
- Assisting the anesthesiologist during an awake intubation. The patient requires support during the process of numbing the gag reflex and vocal cords which can take some time. Assist with helping the patient take Lidocaine viscous gel, asking them to gargle but not swallow it, and assist with suctioning or providing a tray to spit into. Assist with holding a patient’s tongue, as the anesthesiologist sprays the back of the throat. The anesthesiologist may ask you to inject Lidocaine into a port of the flexible laryngoscope or they may inject it directly into the trachea (between the thyroid and cricoid cartilages) to bathe the area with local anesthetic.
- Ensure Tetracaine drops have been given over a certain time period prior to the start of the surgical procedure
- Document any drops given on operative record. The anesthesiologist will document any drugs administered during an awake intubation.
Infiltration Anesthesia #
Infiltration of local anesthetic involves injection of the drug directly into the surgical area (local block) or into the tissue surrounding the surgical area (field block). Infiltration of local anesthesia may be injected into a surgical site prior to the suturing a superficial wound and at the beginning of the procedure or at the end of a surgical procedure in order to provide postoperative analgesia. A vasconstricting agent may be injected in addition to the local to reduce bleeding in and around the surgical site (i.e. Marcaine 0.25% with 1:200,000 Epinephrine). The vasoconstrictor also aids in decreasing blood flow around the area, causing a slower redistribution of the drug away from the area. Local combined with Epinephrine will double the duration of action.
Responsibility of nurses:
- Label all drugs on the surgical field – container and syringe. Verify with the surgeon what local anesthetic drug you are passing to them.
- Pass up syringe and needle using safe sharps practices (i.e. neutral zone)
- Count needle (and syringe) on operative count sheet (see PN 4)
- Document amount used on operative record
Monitored Anesthetic Care (MAC) #
Monitored anesthetic care (MAC) is the term to describe that the anesthesiologist is monitoring the patient vital signs and level of comfort but the surgeon is administrating of the anesthetic in the form of topical or infiltration anesthesia. If the local anesthetic drugs are inadequate for the patient, the anesthesiologist may administer a light sedative or convert to a general anesthetic, if required. An anesthesiologist will also monitor for side effects of local infiltration (i.e. total anesthesia after a retrobulbar block is administered).
When MAC is not required (i.e. simple wound suturing, a registered nurse will be responsible for monitoring the patient. Usually pulse oximetry and blood pressure monitoring are sufficient, but in some institutions require ECG monitoring. Two nurses should be present: a registered nurse to monitor the patient and another perioperative nurse to assist the surgeon.
Peripheral Nerve Blocks (PNB) #
Peripheral Nerve Blocks (PNB) #
A peripheral nerve block is when a local anesthetic is injected around a peripheral nerve or nerve plexus that innervates a particular area of the body (encompassing the surgical site). Peripheral nerve blocks provide anesthesia as well as some akinesia (lack of movement), as sensory and motor impulses are blocked to and from the injected nerves. PNB can be performed for surgical anesthesia or for postoperative pain control. For longterm postoperative pain control, an indwelling catheter may be placed to allow for repeated injection of local anesthesia. Examples of PNB are brachial plexus (for the shoulder), axillary block (for the hand and medial side of the forearm), ulnar/median/radial nerve blocks (for the hand), femoral nerve block (for the leg), popliteal block (for the lower leg) and peribulbar and retrobulbar blocks (for the eye).
To administer a peripheral nerve block, the anesthesiologist will follow these steps:
- Cleanse the area with antiseptic solution around the nerve location
- Locate the nerve or nerve plexus with the use of a special insulated needle (regional block needle). This needle has wires attached that will connect to a nerve stimulator; one conducting wire and one ground wire. The nerve stimulator will send impulses down the needle shaft which will help to locate the nerve (motor branch), by stimulating the nerve and producing twitching of the muscles around it.

- The anesthesiologist will landmark the location of the nerve and insert the needle with the nerve stimulator turned on. Once the desired twitching is achieved, syringes with the local anesthetic will be attached (via an extension tubing attached to the needle) and the syringe is aspirated first to ensure that the needle is not in a vessel (no bloody return). The local is then injected and depending on the volume (usually around 40-80cc), the syringe will be aspirated a few times to ensure that the needle has not moved. Sometimes, the local anesthetic will contain CO2 (carbonated) to promote and increase the absorption

- An ultrasound device may be used to assist with locating the nerve and to guide imagery of the needle insertion. The anesthesiologist will be able to see the anesthetic drug being injected and visualize the tissue around the nerves being infiltrated. The ultrasound can prevent the inadvertent introduction of the needle into an artery or vein which are often located near the nerves.
Ultrasound assisted needle insertion & Ultrasound image of needle placement( 2 photos below)

- A tourniquet is often used for surgery of the extremities so it is important that the block extend far enough up the limb to anesthetize the discomfort of the tourniquet site as well as the surgical site.
Peribulbar and Retrobulbar Blocks #
Ophthalmic blocks are often administered by the ophthalmalogist or eye surgeon with the anesthesiologist providing MAC, as these blocks have potentially serious side effects.
The peribulbar block involves injections above and below the orbit, with local anesthetic deposited in the orbicularis oculi muscle and beneath, above and behind the globe. The potential for intraocular or intradural injection is limited because the anesthetic is deposited outside the muscle cone. The risk of intraconal hemorrhage and direct optic nerve injury is also less than with a retrobulbar block.
A retrobulbar block is a regional anesthetic nerve block into the retrobulbar space, the area located behind the globe of the eye. Local anesthetic is injected into this space. This injection provides akinesia of the extraocular muscles by blocking cranial nerves III, IV, and VI, thereby preventing movement of the globe. It also provides sensory anesthesia of the conjunctiva, cornea and uvea by blocking the ciliary nerves. This block are often used for retinal or orbital surgeries but may be used for other intraocular surgeries. The risk of complications with the retrobulbar blocks is leading to more frequent use of the peribulbar block.

Potential complications for retrobulbar blocks include: bradycardia, junctional rhythm, or asystole which can occur secondary to traction on the eye and ocular muscles. This is called the oculocardiac reflex (OCR). Atropine or Glycopyrrolate can be used to treat this reflex. Caution should be used when massaging the eye after placing the block. The eye is commonly massaged with light pressure after the local anesthetic is injected to promote onset and completeness of the block. In some institutions, a pressurized headband is worn after the block is administered and the surgical procedure is not commenced until after a short waiting period. Another complication of a retrobulbar block is total anesthesia or apnea due to the accidential injection of the local backwards into the brain circulation or cerebral spinal fluid (CSF). It is also possible to cause rupture of the globe during a retrobulbar injection which is why the surgeons favor the peribulbar block.
Nursing Responsibilities for Peripheral Nerve Blocks #
- Know the location of regional block needles and different types. Know location of and how to work nerve stimulator and ultrasound machine.
- Provide comfort during the peripheral nerve block; verify that the muscle twitching is normal. Adjust settings if twitching painful or excessive (at discretion of anesthesiologist)
- Turn on and adjust nerve stimulator
- Inject local anesthetic as directed once nerve location identified
- Prepare to provide local anesthetic for injection onto sterile field as an adjunct in case nerve block inadequate
- Ensure that patients receiving a peribulbar or retrobulbar block are continuously monitored. These patients can never left alone (especially in the preoperative area where the block may be administered).
- Ensure that the perioperative team completes the SSCL and verifies the site and side prior to administration of the PNB.
Intravenous Block (Bier Block) #
Intravenous Block (Bier Block) #
An intravenous block, commonly referred to as a Bier block, is the type of anesthesia used on an extremity (the arm or the leg) for procedures that are completed in approximately one hour (i.e. hand procedures such as tendon repair). The Bier block works by injecting the local anesthetic via an intravenous line while circulation to the limb is occluded by a pneumatic tourniquet. The tourniquet ensures that the local anesthetic remains within the extremity, until the pressure is released. The dosage of the drug is determined by the length of the procedure.
NOTE: It is very important to consult the anesthesiologist before deflating the pneumatic tourniquet. The tourniquet should not be deflated until most or all of the local anesthetic is metabolized. Pre-mature deflation of the tourniquet can result in the release of a bolus of the local anesthetic drug into the rest of the patient’s body causing systemic toxicity.
Note: Students are expected to have a basic understanding of what a tourniquet is and how it work. Students will have a chance to practice and learn more about tourniquets and Bier Blocks during the full-time clinical portion of the program.

The steps for administering a Bier block are:
Intravenous access is attained in the non-operative arm for the administration of sedatives and for hemodynamic control (if necessary). On the operative arm:
- A small gauge intravenous is started near the hand of the operative arm
- A double-cuffed tourniquet is applied – it should fit snugly (should only be able to insert two fingers under it) and should overlap 3 to 6″. The tourniquet hoses are attached and both cuffs of the tourniquet are set for a pressure of 250mmHg for the arm (for a leg – set to 300mmHg)
- The limb is elevated to reduce venous pooling. At times an esmarch bandage (a thin elastic tensor-like bandage) may be applied from the distal end of the extremity to the tourniquet in a circumferential manner, assisting to squeeze (exsanguinate) the limb.
- Prior to lowering the limb the upper (proximal) tourniquet cuff (cuff A) is inflated
- The local anesthetic is injected
- The lower (distal) tourniquet cuff (cuff B) is inflated
- Once the lower cuff is inflated, then the upper (proximal) cuff is deflated – one cuff must be inflated at all times once the local anesthetic has been injected. Some anesthesiologists will vary as to which cuff they inflate first; however, it is preferable to inflate the upper cuff first, as this allows for the local anesthetic to rise up to the level of the upper cuff. This creates a situation where when the lower cuff is inflated, it will be over an anesthetized area, making the high pressure of the tourniquet comfortable for the patient
- Often the intravenous is removed, as it will be in the way of the surgical site
- The tourniquet must only be inflated for a maximum of 90 minutes for arms and 120 minutes for legs to minimize the adverse effects of ischemia to muscles and nerves.
- If the procedure is completed more quickly than anticipated, do not automatically deflate the cuff. Premature deflation can cause a bolus of the local drug to be introduced into the systemic circulation and may cause systemic toxicity. The cuff must remain inflated for a minimum of 20 minutes. Always check with the anesthesiologist before deflating the cuff.
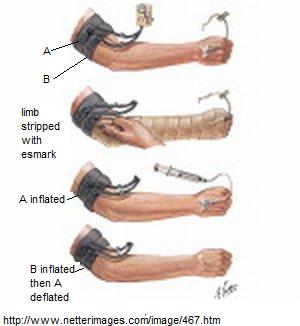
Nurses Responsibility:
- Assist with intravenous insertion
- Apply or assist with applying the tourniquet properly
- Assist with exsanguinating the limb (if necessary)
- Knowledge of the tourniquet machine:settings, inflation, deflation
- Inflate and deflate the tourniquet in proper sequence: always know which one is inflated
- Double-check that cuff has inflated prior to administration of local anesthetic and prior to deflating upper tourniquet (after lower one has been inflated). One cuff must always be inflated and it cannot be deflated for twenty minutes.
- Know the signs of local anesthetic toxicity
Signs and Symptoms of Local Anesthetic Toxicity
Careful monitoring of the patient for any of these signs and symptoms of local toxicity is important to determine if toxicity is due to tourniquet failure, inaccurate inflation/deflation sequence or premature deflation of tourniquet at the end of the case.
Although Bier blocks are effective, they are not done as frequently as peripheral nerve blocks (especially for postoperative pain control) because PNB are easier to administer and more successful.
Systemic toxic reactions to a bolus of local anesthetic (or rarely, an over-administration by repeated injection) are progressive as the level of the drug in the blood rises.
Initial symptoms are: central nervous system excitation such as a ringing in the ears (tinnitus), a metallic taste in the mouth, or tingling or numbness of the mouth.
Later symptoms are: motor twitching in the periphery followed by grand mal seizures, coma, and eventually respiratory arrest. At extremely high levels of toxicity, cardiac arrhythmia or hypotension and cardiovascular collapse can occur.
Symptoms are managed and treated until they resolved and local anesthetic is metabolized.
Central Nerve Blocks #
Central Nerve Blocks #
Neuroaxial (central) blocks are accomplished by depositing the local anesthetic in proximity to the nerve roots of the spinal cord and the spinal cord, itself. There are two types of central nerve blocks that will be discussed: spinal and epidural.
Anatomy and Physiology #
Epidural or spinal analgesia/anesthesia involves the injection of an opioid or a local anesthetic (or a combination of both) into the epidural or subarachnoid space. The spinal cord occupies the upper two thirds of the vertebral canal. It is approximately 42 cm long and usually ends at the level of the first lumbar vertebra (L1).
The brain and spinal cord are continuous and are encased by 3 membranes:
- the dura mater (the tough outermost layer),
- the arachnoid
- the pia mater (thin innermost layer adherent to the brain and spinal cord).
Between the pia mater and the arachnoid is the subarachnoid space which is filled with cerebral spinal fluid (CSF). The total volume of CSF is about 150ml (20-30ml of CSF is found in the spinal canal). Thirty-one pairs of spinal roots and nerves exist in the spinal cord. The autonomic parasympathetic fibers have craniosacral origins, and the sympathetic fibers arise from the thoracolumbar area of the spinal cord. After leaving the spinal cord, the spinal roots and autonomic nerves pass through the subarachnoid and epidural spaces, forming peripheral nerves and nerve plexuses leaving the spinal cord.
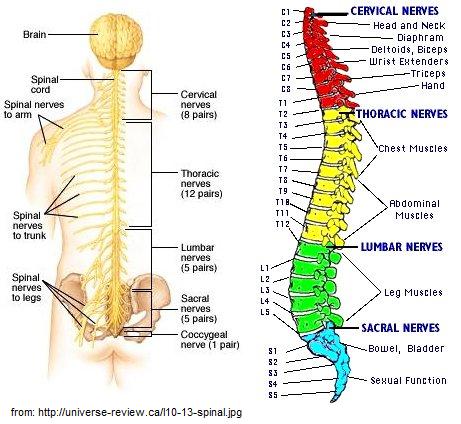
Spinal Anesthesia #
Spinal anesthesia is accomplished by injection of the local anesthetic drug into the subarachnoid (intrathecal) space of the spinal column.
The subarachnoid space is a space between the arachnoid and the pia mater. Medication injected into this space mixes with the CSF around the spinal cord and spinal cord nerve roots. When inserting the spinal needle into this space, it is important to enter the space below the level of the spinal cord termination to reduce the risk of permanent damage to the cord. Anesthesiologists will use the iliac crest, which is approximately the level of L4, as a landmark. The subarachnoid space lies between the pia mater and the arachnoid and is filled with cerebral spinal fluid (CSF) – see diagram below. Local anesthetic is injected into this space and mixes with the CSF around the spinal cord and spinal cord nerve roots.
Blockade Sequence #
Progression of the blockade is based on the size, anatomy and location of the nerve fibers in the subarachnoid space. In spinal anesthesia, the progression usually begins in the feet (caudally) and progresses upward (cephalad), in the following way:
- Vasodilation: increase in cutaneous perfusion; patient will experience a warmth in the affected area
- Cold Discrimination: patient will report advancing sensation of warmth from the toes to head. Patient will report sensation of warmth to cold stimulus (i.e. when touched with ice or alcohol swab)
- Fast and dull pain: patient will report dull pain in affected areas (i.e. when touched by a pin) and sharp pain in unaffected areas. Surgeon should perform a pain test prior to making incision by pinching the patient’s skin with forceps.
- Light versus deep touch: patient should not be able to feel light touch, but deeper touch may still be present
- Proprioception: patient is unable to discriminate position or location of blocked extremities
- Motor: patient will be unable to move affected area/limbs
Once the motor stage of blockade has been reached, it can be assumed that the block is successful and the cephalad block has taken effect.
As the blockade wears off, return of movement and sensation will occur in the opposite order with motor function returning first. Central nerve blocks are appropriate for postoperative pain control due to the lack of sensory perception (i.e. pain) for some time after motor function has returned.
Spinal Anesthesia: Hyperbaric vs Hypobaric Solutions #
Depending on the type of local anesthetic solution used, the patient may be asked to remain in the sitting or lateral position to allowing the local solution to “descend” to levels lower than where it was injected or make the block unilateral (i.e. if lying on the left side it can stay only on the left side and the right side is unaffected). The patient can be positioned so the local solution can “rise” to higher levels. Do not move the patient out of position too soon as it can take up to 10 minutes for the local solution to “settle”. Spinal anesthesia is achieved through the density or baricity of the solution relative to CSF. There are three types of solutions:
- Isobaric: solution has the same density as CSF. This type of solution will remain in the area that it was injected and resist spread. The patient can be repositioned immediately after injection without altering the level of anesthesia.
- Hyperbaric: solution is heavier than CSF. This is achieved by mixing the local anesthetic with a glucose (D5W) solution. Because hyperbaric solutions are heavier than CSF, they tend to settle to the most dependent area of the subarachnoid space. The most dependent area is determined by the patient’s position at the time of local injection. If the local is injected at the L2-3 interspace when the patient is sitting, the greater density will allow the local to sink to the sacral segments of the spinal cord. If the patient is lateral, an injection at the L2-3 interspace will cause the dependent hip and leg to be anesthetized. If the patient is supine or slightly trendelenburg, the drug will gravitate up into the thoracic region, creating unnecessary or unwanted thoracic involvement.
- Hypobaric: solution is lighter than CSF. This is achieved by the addition of sterile water to the solution. This type of solution is not commonly used due to its unpredictable level of spread to the non-dependant area when a patient is in the sitting position.
For the step-by-step sequence to administering a spinal anesthetic block, please click on the following supplemental information: SI – Administering a Spinal Anesthetic Block
Epidural Anesthesia #
Epidural anesthesia is accomplished by the insertion of an epidural catheter into the epidural space and injection of the local anesthetic drug into the epidural space via a epidural catheter.
The epidural space contains blood vessels, lymphatics, fatty tissue and spinal nerve roots. It is located outside the 3 membranes covering the spinal cord, between the dura mater and the ligamentum flavum. Venous plexus are prominent, but no free fluid exists in the epidural space. The ligamentum flavum is a tough ligament binding the spinal vertebra together, and must be punctured in order to access the epidural space found just beyond it.
After the local anesthetic solution is injected into the epidural space, the local eventually diffuses across the dura and arachnoid membranes into the subarachnoid space. Because there is no free fluid in the epidural space, an epidural bolus can be given at prolonged intervals (hours apart) via a catheter without the catheter clotting.
For the step-by-step sequence to administering an epidural anesthetic (block), please click on the following supplemental information : SI – Epidural Anesthesia Block Sequence .
SPINAL Versus EPIDURAL
Spinal
- Injected into subarachnoid space
- Usually one time bolus
- Insertion is below the termination point of the spinal cord to reduce the risk of permanent damage to the spinal cord (L2 but usually L4 – iliac crest level)
- Type of solution injected can affect level of block
- Spinal needle is smaller and has a special tip so that it will enter the tough dura layer and seal after the needle is removed (preventing a CSF leak and complication of post-spinal tap headache)
- Epidural Injected into epidural space
- One time, intermittent or continuous infusions
- Insertion can be in the thoracic, lumbar or caudal areas of the spine
- Epidural needle has a blunt tip to reduce the chance puncturing through the dura and a catheter can be threaded through the needle
- The epidural dose can be ten times greater than a spinal dose.
- If the high dose of medication is injected into the subarachnoid space in error, a profound block will occur causing potential respiratory and circulatory collapse.
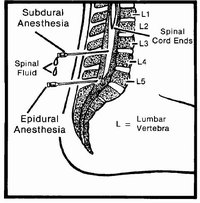
Positioning For a Central Nerve Block #
Lateral Position
In the lateral position, the patient lies with their knees drawn up to the abdomen, the upper arm resting across the chest, the lower arm lying at a right angle to the body, and the head flexed and resting on a small pillow. The vertebral column should rest at the edge of the bed and parallel to the table. Flexion of the lumbar spine opens the interspaces and eliminates the natural lumbar lordosis of the body; making the lumbar vertebrae more visible and enlargng the interspace between each vertebra. The nurse should always stay with the patient ensuring that the correct position is maintained and patient safety and comfort are preserved.
Often elderly patients who present with broken hips will be given a spinal anesthetic. These patients will be placed in the lateral position, usually lying on the unaffected side (broken hip up). This will require flexing only the bottom leg and trying to keep the upper limb straight and undisturbed on a pillow. Unfortunately, this does not allow for the best flexion of an stenotic spine, but it is the safest and most comfortable for the patient (even with sedation). It is important to provide warm blankets to cover shoulders and legs of the patient.
Sitting Position
The patient sits on the edge of the bed with the feet supported by a sitting stool or platform. The head is flexed on the chest, shoulders hunched and arms folded across the upper abdomen resting against a pillow, or supported in front of the chest on a table or stand. An assistant stands in front of the patient to hold the shoulders level and prevent lateral flexion or rotation of the spine. At times, asking the patient to push out their lower spine, “Make your body into the letter C”, “Curl up like a shrimp” or “Make your back like an angry cat” can help them visualize the position they should be in. Asking them to be in the fetal position causes them to lean too far forward as opposed to arching their back. The nurse should always stay with the patient to ensure that the correct position is maintained and patient safety and comfort are preserved. It is important to provide warm blankets to cover shoulders and legs of the patient.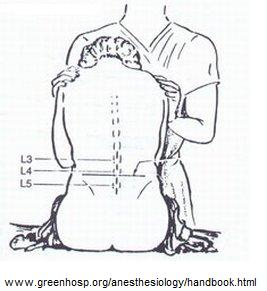
Indications, Contraindications and Complications of Central Nerve Blocks #
The indications for administering a spinal or epidural anesthetic include:
- Patient may be wide awake (if desired) or choose varying levels of sedation ranging from mild anxiolysis to conscious sedation
- Patient consciousness is maintained so airway and ventilatory reflexes are preserved, thereby, avoiding the complications of general anesthesia (i.e hypoventilation, airway obstruction, aspiration)
- Negates the need to attempt a difficult intubation in patient’s known to have a known difficult airway
- Provides regional muscle relaxation without having to paralyze the entire body with a muscle relaxant drug (as in general anesthesia). In addition, after a spinal anesthetic, motor neural pathways return prior to sensory pathways, providing good postoperative analgesia
- An epidural catheter can provide ongoing and continuous analgesia intra-operatively as well as post-operatively
- The sympathetic nervous system (SNS) blockade provided by a spinal anesthetic is beneficial in: facilitating surgical exploration and wound closure by contracting the bowels; inhibiting the metabolic and endocrine responses associated with surgery (i.e. increased cortisol levels); and producing vasodilation which, in turn, reduces arterial blood pressure (which results in less bleeding at the surgical site); and increases blood flow to the extremities (decreases the incidences of thromboemboli).
- Eliminates the need of administering malignant hyperthermia triggering agent drugs (i.e. volatile anesthetic gases & Succinylcholine)
Contraindications for central nerve blocks are:
- CNB are best suited for procedures in the lower abdomen and extremities. Higher surgical site incision on the body result in a more profound the SNS blockade and possible hemodynamic changes. The level of the T4 vertebra (nipple line) is appropriate for some upper abdominal procedures.
- The inevitable vasodilation may not be suitable for patients with aortic stenosis as they require adequate cardiac output (require high venous filling pressures)
- A high level of blockade may be dangerous for patients with respiratory diseases (i.e. COPD) as respiratory function can be impaired.
- Spinal anesthesia is a single dose; therefore, the surgical procedure can be limited to the amount of anesthesia given. An epidural or general anesthetic may be required for longer procedures. Sometimes an unanticipated longer surgery will end up as a spinal anesthetic converting to a general anesthetic.
- Patient refusal: patients may refuse spinal anesthesia because they are anxious and do not wish to be awake during the procedure.
- Infection at the site of injection or systemic sepsis
- Uncorrected hypovolemia or coagulopathies (always check the INR or report abnormal INR to anesthesiologist)
- Anatomical abnormalities of the spinal canal (vertebrae/ligaments) are not an absolute contraindication, but may impede attempts to administer the block
Complications of central nerve blocks include:
- Hypotension – treat with drugs (Phenylephrine or Ephedrine) to maintain BP and IV crystalloid (like IV normal saline) or colloids (like Pentaspan) to restore preload and elevate BP.
- Bradycardia – due to block of cardiac accelerator fibers (T 1-4) or result of hypotension (treated with Atropine)
- Respiratory insufficiency – even when intercostal muscles are affected, the phrenic nerve and diaphragm usually are not affected; therefore, respiratory arrest is rare. Airway clearance due to ineffective cough in some patients (i.e. COPD) does occur.. Repiratory arrest is usually related to hypotensive causes.
- Total spinal block – can be caused by inappropriate drug dosage or positioning and will cause a very high level of spinal blockade up into the cervical segments of the spinal cord. Patient will require intubation. This is the situation described as “I was awake but couldn’t breathe”
- Nausea – due to either hypotension or parasympathetic activity in the GI tract (treat with Atropine)
- Urinary retention – sacral nerve function and innervation to bladder is slow to recover and large amounts of IV fluid can cause urinary retention. Always catheterize elderly patients.
- Post spinal headache – due to an unsealed dural puncture site from a spinal anesthetic and leakage of CSF for several days post-operatively. The headache is often severe in the upright position, located in frontal or occipital area and accompanied by diplopia and tinnitus. It may resolve spontaneously or require treatment. Treatment involves IV infusion of caffeine sodium benzoate or epidural blood patch (10-20 ml of patient’s blood is aseptically injected via lumbar puncture over the dural puncture site to clot/seal over the hole).
Nursing Responsibilities #
- Obtain a blood pressure prior to positioning the patient
- Assist with the opening of sterile supplies from spinal/epidural kit
- Assist with patient positioning and support the patient in maintaining the correct position
- Ensure that the patient does not move, especially during critical moments such as when the spinal needle is inserted; when the local anesthetic is administered and/ or epidural catheter is being inserted.
- Stay with the patient at all times. They are often sedated and can easily fall. Ask others in the room to obtain any necessary items or have someone else stand with the patient if the nurse is needed obtain supplies
- Keep patient warm, but ensure blankets are clear of the sterile field
- Assist anesthesiologist in identifying the iliac crest – helps to determine area to be cleansed with antiseptic and for finding correct vertebral level
- Ensure sedated patients are taking deep breaths; monitor pulse oximeter readings
- Inform anesthesiologist if the patient is exhibiting symptoms of pain. Observe the patient for signs of wincing and other facial expressions or sounds that indicate pain. The patient should feel pressure not pain during the CNB and should be instructed to speak up without moving.
- Assist with taping of epidural catheter in place
- Assist the patient to surgical position after the CNB; may need to be sitting up or lying on side for up to 10 minutes if hyperbaric solutions are used
- Monitor for hypotension and assist with corrective measures
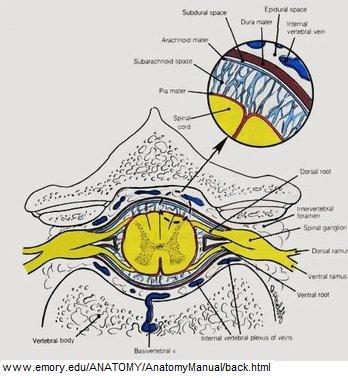
Anesthetic Complications #
Many potential complications can result from various procedures but it is important to recognize the emergency situations that can occur while a patient is undergoing an anesthetic. Six complications from an anesthetic will be discussed.
Malignant Hyperthermia #
Malignant hyperthermia (MH) is a fulminating hypermetabolic state occurring in genetically predisposed individuals when exposed to triggering agents. Potential triggering agents include: commonly used volatile gaseous inhalation anesthetics such as Isoflurane, Desflurane, Sevoflurane, Methoxyflurane; the muscle relaxant Succinylcholine and some local anesthetics (Lidocaine).
The triggering agent increases the intracellular calcium ion concentration. The elevated calcium level produces a chain of reactions that are manifested by: a greatly increased body metabolism, muscle rigidity and a high fever which may exceed 42° C (thus the name hyperthermia). Death or brain damage may result from cardiac arrest, internal hemorrhaging or failure of other body systems. Episodes of malignant hyperthermia are rare and most often occur in children and young adults. The exact incidence is unknown but may range from one in 65,000 to one in 5,000. Susceptibility to MH occurs through an inherited gene, and males are more likely to develop MH than females. MH was first identified in 1960. The mortality rate of nearly 80% has been dramatically reduced by the introduction of the drug Dantrolene sodium (drug for reversing the exacerbated release of calcium) in 1979.
A family history of severe reactions during anesthesia can lead to a suspicion of MH. The diagnosis can be confirmed or ruled out by skeletal muscle biopsy. Patients are anesthetised using an “MH-safe” anesthesia then a piece of muscle is surgically-removed for standardized laboratory testing.
Signs and symptoms of MH
:
Early signs of an MH reaction are increased CO2 in blood or exhaled gas, rapid irregular heart rate, excessively rapid deep breathing, and blueness of the skin. These symptoms are followed by muscle rigidity (masseter muscle of jaw common indicator) due to an intense release of calcium into the muscle cells causing contraction, acidity of the blood and muscle cell damage. The body temperature rapidly rising to extremely high values (> 42°C). If the reaction is unchecked, the muscle cell membrane is disrupted causing leakage of myoglobin (leading to kidney failure), leakage of K+ and Ca++ (leading to heart failure and cardiac arrest), failure of coagulation, and eventually brain death.
MH may be difficult to diagnose as every MH reaction may not exhibit all the symptoms as described.
Treatment:
- Strict preoperative screening (ask re: family history) and in some high risk cases, administration of preventive dose of Dantrolene
- Removal of all triggering agents from the operating room preoperatively (for known or suspected cases)
- Early diagnosis of symptoms and prompt treatment: stop triggering agent, flush with 100% O2 to clear anesthetic machine of all inhalational gases and hyperventilate patient with 100% O2 (may have to manually ventilate patient at this time)
- Administration of IV Dantrolene; needs to be reconstituted and administered in large quantities.
- Cool patient with cooling blanket, sterile ice (slush) in operative wound, ice lavage (gastric, urinary and rectal), ice packs in axillae and groin
- Treat other hemodynamic symptoms (i.e. to correct acidosis, administer Sodium bicarbonate), observe end tidal CO2 and arrythmias
- Isolate the patient in a room in PAR, as the expiration of gases from other patients may also trigger a reaction. Patient is at risk for up to 48 hours after receiving an anesthetic
Nurses Responsibility:
- Call a code: to solicit as much assistance as needed
- Getting the Malignant Hyperthermia cart or bin: every hospital will have a bin with necessary supplies including Dantrolene
- Assisting the anesthesiologist in stopping all volatile anesthetics and Succinylcholine; change the anesthetic tubing; hyperventilate the patient with 100% oxygen; administering drugs such as Dantrolene, Sodium Bicarbonate and anti-arrhythmia drugs.
- Retrieve the cardiac arrest cart
- Mix Dantrolene (discuss at your site)
- Ensure that blankets are cool
- Retrieve cold IV fluids, cold body cavity lavage solutions and ice
- Send blood work to lab
- Inform PAR
Malignant Hyperthermia rarely occurs in a fulminant state due to advanced screening methods and increased understanding of MH. However, MH is a potential anesthetic emergency and it is the responsibility of the perioperative nurse to understand his/her role and to be prepared to manage this emergency, should it occur.
Laryngospasm #
Laryngospasm is a forceful involuntary spasm of the laryngeal musculature caused by sensory stimulation of the superior laryngeal nerve. Stimuli that may trigger laryngospasm include pharyngeal secretions, blood, food, vomitus or a foreign body in the larynx or passing of the endotracheal tube (ET) through the larynx during extubation.
This glottis closure reflex can continue even after the irritation to the mucosa ceases. Varying degrees of laryngospasm produce sounds that range from a high-pitched, squeak, crowing sound to the total absence of sound. The latter indicates complete closure of the cords and there is no airflow. Laryngospasm occurs most commonly upon extubation of the patient. The anesthesiologist will direct the treatment of this condition by suctioning to remove secretions, blood etc and repositioning of the mandible in combination with oxygen by mask, under positive pressure. However, if the condition persists, it may be necessary to administer a short-acting muscle relaxant such as Succinylcholine. As a last resort, the patient may have to be reintubated.
Nurses Responsibility:
- Stay at the patient and anesthesiologist’s side during extubation
- Ensure that the operating room is quiet at this time to allow the anesthesiologist to listen to the patient and determine if stridor is present (i.e. the patient has an occluded airway)
- Assist anesthesiologist to reposition head, assist with suctioning or help to manually ventilate with positive pressure (may ask for help with sealing the mask)
- Prepare to draw up some muscle relaxant
- Prepare to obtain intubation supplies for re-intubation and assist accordingly
- Have oxygen tank and mask available for transport
Airway Obstruction #
Airway obstruction can be described as follows:
- Location: upper or lower. Upper airway obstruction (glottic and supraglottic) can lead to a lack of air exchange for the post-operative patient
- Degree: partial or complete. Laryngospasm is a form of complete airway obstruction. If not treated, partial airway obstruction can develop into a complete obstruction.
Anesthesia-related causes of airway obstruction may include:
- Inadequate reversal of muscle relaxation
- General anesthesia depresses the airway reflexes of coughing and swallowing resulting in the inability to clear secretions
- Glottic edema from tracheal intubation
- Peripheral nerve blocks to the head and neck area can potentially injure blood vessels and the resultant bleeding can compress the airway directly or through mucosal edema from obstructed venous drainage.
Surgery related causes of airway obstruction result from procedures around the head and neck, which can lead to obstruction by causing displacement or compression of the airway due to:
- Soft tissue edema around the head and neck (steroids may be administered preoperatively if this is anticipated)
- Dislodgement of surgical packing or clots
- Bleeding into or adjacent to the airway
- Accidental transection of nerves (i.e. recurrent laryngeal nerve) involved in reflexes (gag, swallowing, coughing).
- Surgical positions that require the patient to be prone or in a “head-down” position may cause facial and neck edema
Patient related causes of airway obstruction can result from:
- Medical conditions resulting in neuromuscular weakness, especially of pharyngeal and laryngeal muscles may prevent spontaneous airway clearance due to a weakened cough (i.e. Myasthenia Gravis or ALS)
- Pre-existing airway diseases (e.g. asthma, bronchitis or smoking-related diseases)
- Excessive soft tissue surrounding the airway increases the risk for edema
- Excess soft tissue of head, neck and trunk impair mandibular and cervical mobility and ability to position airway for maximal patency
- High risk for gastric aspiration secondary to increased intragastric pressure (i.e. pregnancy), increased gastric volume (i.e. recent meal) and decreased tone at the lower esophageal sphincter (i.e. GERD)
- Elderly patients: potential to dislodge teeth; diminished laryngeal reflex reactivity; limited cervical (neck) mobility
- Pediatric patients (under 8 years old): large head causes flexion of short neck; larger soft tissue structures (tongue and epiglottis); larynx is more cephalad than an adult which results in greater airway closure when neck is extended; shorter trachea; and narrower subglottic airway
- Trauma to the head and neck
Nurses Responsibility:
- Prepare for emergency intubation, reintubation or transferring the ventilated patient to PAR
- As above for laryngospasm
- Perform cricoid pressure for at risk patients (i.e. GERD)
- Assist the anesthesiologist in performing rapid sequence induction for patients who have not been sufficiently or suspected of not being NPO, are pregnant, or experienced trauma
- Be prepared to manage the risks of intubation/extubation of geriatric and pediatric patients
- Have difficult airway equipment readily available for obese patient with short necks
Hypothermia #
Hypothermia may negatively affect perioperative patients intraoperatively and during postoperative recovery. Hypothermia may result in:
- Increased incidence of wound infection
- Altered cardiac performance
- Altered coagulopathy
- Altered action of common anesthetic drugs
- Delayed emergence from anesthesia
Perioperative patients are prone to hypothermia because anesthetic agents cause internal redistribution of the body core heat to the extremities and peripheral tissues, which leads to vasodilation. Further heat loss occurs through radiation, convection, conduction or evaporation. Contributing factors include:
- The room is kept cool due to the continuous air exchange for infection control and OR personnel are scrubbed under warm operative lights
- IV fluids may be room temperature
- Irrigation fluids may be room temperature
- Body surface is exposed to the cool room air during positioning and skin preparation
- Some skin prep solutions are alcohol-based
- Body cavities are open to room air during surgery
- Adminstration of gases that are not warmed or humidified.
Take a moment to reflect on what happens to your body when you are cold.
Hypothermia is defined as a patient temperature < 36°C. Hypothermia is detrimental because:
- Postoperative shivering increases the need for oxygen by 300-400% and increases the risk of myocardial ischemia and angina
- During general anesthesia the body cannot compensate for hypothermia: anesthetics inhibit central thermoregulation by interfering with hypothalamic function
- A shift in the oxyhemoglobin dissociation curve occurs; hemoglobin has a greater affinity for oxygen and does not readily release oxygen for cell and tissue use
- Loss of intravascular volume due to vasoconstriction
- When the body rewarms and vasodilation occurs, the patient becomes hypovolemic
- Geriatric and pediatric patients are the most vulnerable to its effect.
Negative effects of hypothermia:
- CNS depression leads to an increased level of anesthesia
- Drugs (especially muscle relaxants) are metabolized more slowly
- Clotting abnormalities (increased platelet activity, decreased fibrinolysis)
- Increases the incidence of wound infection (due to vasoconstriction)
The RN role in preventing hypothermia:
Nurses responsibility:
- Provide warm blankets prior to induction
- Keep patients covered as much as possible – only expose areas necessary for surgical skin prep
- Warm all fluids (IV and irrigation) administered to the patient
- Apply electric forced-air warming blanket on the patient during surgery; cover the patient’s head with the blanket (large amount of heat is lost through the head)
- Always warm the patient’s head and chest area, if possible; more conducive to overall core body temperature. Warm the legs during abdominal surgery.
- Obtain temperature-monitoring equipment (oral, rectal).
- Adjust the room temperature as high as is comfortable for all
Inadvertent hypothermia is a preventable complication of surgery. Recognizing the causes and effects of hypothermia is essential to the implementation of the most effective nursing interventions.
Hypovolemia #
The patient may present to the operating room in a hypovolemic and/or hypotensive state or may become hypovolemic and/or hypotensive during the surgical procedure. Signs and symptoms of hypovolemia include: tachycardia and/or arrythmias, decreased or unstable BP, and with increasing blood loss, coagulopathies can develop. Causes of hypovolemia include:
- Trauma: severed blood vessels, blunt trauma (intrabdominal, intrathoracic)
- Highly vascularized tissue or tumors; some patients may have tumor vessels embolized prior to surgery to cut down on bleeding
- Surgical-induced trauma: inadvertent nicking of an artery
- Medical conditions: patients on anticoagulants that have not been stopped preoperatively, increased INR, coagulopathic diseases (e.g. hemophilia)
- Dehydration: patients who have been NPO for long periods of time may be fluid (and electrolyte) depleted: geriatric and pediatric patients are most vulnerable.
nurses Responsibility:
- Vancouver Coastal Health and Fraser Health requires all multidisciplinary team members that are new or current employees and will be or are involved in transfusion practices to complete an annual review of transfusion education. This review can be accomplished by completing the Safe Transfusion course on the Course Catalogue Registration System (CCRS) at https://ccrs.vch.ca .
- Be aware of the patients hemodynamic status at all times
- Emergent surgeries should be scheduled as soon as possible to prevent prolonged periods of fasting
- For trauma patients or patients with potential for bleeding, have necessary supplies available for the scrub nurse: suture ties, vascular clamps, longer instruments to reach into deep cavities, etc
- Be prepared to assemble the Cell-saver device components (autotransfusion collection machine) if available; usually operated by a perfusionist
- Be prepared to obtain blood products quickly and administer them; double-check any blood products with an RN or physician
- Keep the patient as warm as possible
- For trauma patients, ensure that all equipment and staff are fully prepared to start the surgical procedure; the incision should not be made until all members of the perioperative team (especially the anesthesiologist) are prepared for intraoperative emergency care.
History of Anesthesia #
The science of anesthesia has undergone many changes over the years. A brief synopsis of it’s history is as follows:
Minoan times to early 19th century: Opium and alcohol were used to intoxicate patients for painful procedures or for those requiring muscle relaxation; hypnosis was sometimes also used. Successful surgery was directly related to the speed of the surgeon.
1804: Although herbal medication was reported in Egyptian times – a Japanese surgeon (Hanaoka) performed a mastectomy using herbal medication
1842: Long (US physician) used ether, but did not publish this fact
1844: Wells used nitrous oxide in dentistry (also in the US). Morton, a former partner of Wells, studied medicine and learned of the anesthetic effects of ether; he used ether to fill a tooth without the patient feeling any pain, and then to extract a tooth. Morton convinced a surgeon (Dr. Warren) at the Massachusetts General Hospital (MGH) to try ether for a surgical procedure (excision of tumor under the jaw); Morton acted as the anesthetist – pictured below.
1846: First medical report of anesthesia. The advent of anesthesia led to advances in surgery. Oliver Wendell Holmes upon hearing of Morton’s use of ether, was the first to actually coin the term “anesthesia”
1884: At the suggestion of Sigmund Freud a surgeon (Koller) used cocaine as a topical agent to perform ophthalmic surgery
1885: A neurologist (Corning) in New York accidentally pierced the dura mater of a dog (he was experimenting with cocaine on the nerve roots) and essentially gave the first spinal anesthetic. In 1898 Bier gave the first spinal anesthetic for obstetrics for delivery.
1942: Anesthesia was recognized by the Royal College of Physicians and Surgeons as a separate specialty in Canada – resulted in the creation of the Canadian Anesthesiology Society (CAS) to oversee examinations (this would not be the case in the UK and US until the 1950’s due to disputes over the length of the exam and years of qualification). Prior to proper exams and fellowship lengths, anesthesia could be administered by a general practitioner.
Hingson and Edwards gave the first epidural anesthetic to a patient with rheumatic heart disease undergoing labor.
1943: In Canada, there were only 10 qualified anesthesiologists; McGill University started a course to train physicians going overseas for WWII. The success of surgery no longer depended upon the speed of the surgeon.
1990’s: Use of the term anesthesiologist to describe someone who has completed medical training in the field of anesthesia. The term anesthetist is used today to refer to a nurse who has been trained in anesthetic procedures and techniques (in the US mainly). Anesthesia technicians (usually specially trained respiratory therapists) provide supportive care to the anesthesiologist when they perform difficult procedures or assist with invasive monitoring.
Modern surgical techniques have become feasible because of the advances in the art and science of anesthesia, as well as the improvement in monitoring vital signs and protocols for fluid and electrolyte balance. The ability to carry out advanced resuscitative measures has gone hand in hand with the complexity of the type of surgery that can be attempted.
Preoperative Assessment for Anesthesia #
The information gathered from a preoperative visit is as follows:
History
- Previous anesthetics: when, what type, adverse effects
- Family history of anesthetic problems: malignant hyperthermia, atypical pseudocholinesterase, hemophilia
- Allergies
- Medications: dosage, reason, duration, effectiveness, when last taken
- Smoking history
- Alcohol use
- Recreational drug use
- Possibility of pregnancy
- Most recent solid and clear fluid oral intake (day of surgery)
- General health and organ system review: respiratory, cardiovascular, central nervous system, gastrointestinal, renal, hematological, endocrine, and musculoskeletal
Physical Exam
Vital signs: HR, BP, weight in kg, height in cm
Respiratory exam/ assessment
Cardiovascular exam/ assessment
Airway: for intubation:
- Cervical spine range of motion and ability to achieve “sniffing” position
- Mouth opening – 3 finger breadths
- Dentition – dentures; bridges; caps; crowns; teeth: loose, chipped, cracked, presence of caries, large incisors. Loose, chipped or cracked teeth should be documented preoperatively for comparison.
- Remove dentures or partial plates – risk of damage if dislodgement occurs
- Crowns and caps are at increased risk of damage, especially upper four front incisors. Patient should be aware of risk.
- Airway obstruction or injury to the pharynx
- Hypomental distance of 3 finger breadths & thyromental distance of 4 finger breadths (6 cm) = easier to intubate
- Neck abnormality or masses
- Oral cavity for view of faucial pillars and uvula. The Mallampati score is a classification referring to a correlation between the visibility of the oropharyngeal structures during a physical exam of the patient’s airway and the degree of difficulty of laryngeal exposure during direct laryngoscopy – the poorer the visualization, the more difficult the intubation. The Cormack and Lehane classification, grades the difficulty of intubation based on the amount of visualization of the vocal cords during direct laryngoscopy.
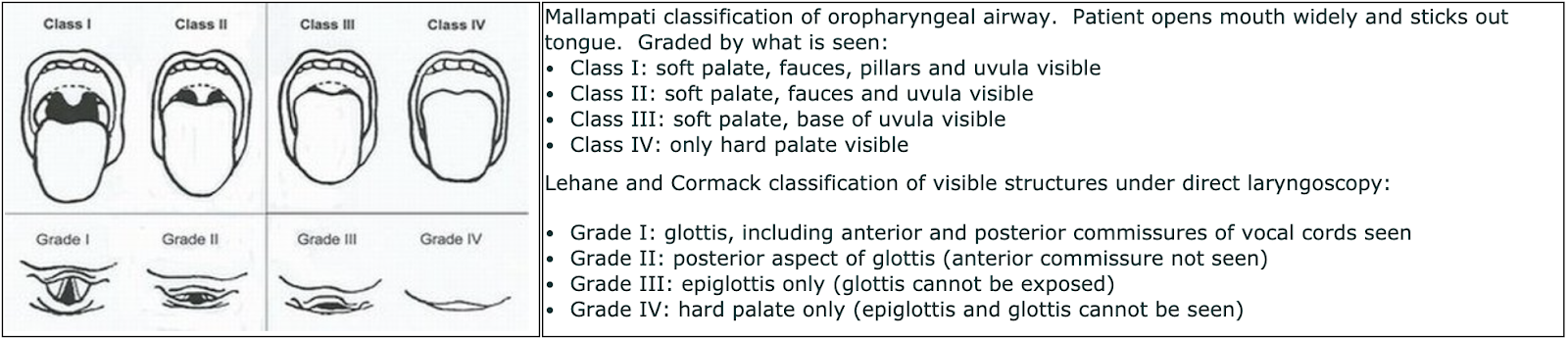
Laboratory tests:
No tests are routinely done preoperatively; it will be patient specific, procedure specific or where clinically indicated. For example a group and screen will be done in procedures where blood loss may be an issue; an ECG is done if the patient has cardiac disease, risk factors or if the patient is over 50 years of age. In most hospitals an INR, G&S and hemoglobin are usually done.
Optimization
Prior to commencing surgery the anesthesiologist (or surgeon) will try to improve the patient’s condition as much as possible. If the surgery is not urgent, it will be delayed until the patient’s condition improves. This may involve:
- Improving coexisting medical problems i.e. Ventolin for asthmatic with wheezing
- Usual medications i.e. cardiac medications, antihypertensives
- Hold diuretics, oral hypoglycemic agents and ACEI (Angiotensin-converting enzyme inhibitor) and A.R.B. (Angiotensin II Receptor Blockers) which may cause hypotension
- Alter dose of insulin – due to stress of surgery and NPO status – insulin orders postoperatively may not be the same as preoperatively
- Alter dose of oral steroid medication – surgery can suppress the adrenals
- Aspiration prophylaxis for patients at risk for aspiration – history of GERD, pregnancy, obese, ophthalmic patients (cannot strain postoperatively):
- Metoclopramide – increases gastric motility and lower esophageal sphincter tone
- Ranitidine – decreases gastric acidity, but ideally dose given the night before and 90 min preop
- Sodium citrate – non-particulate antacid
- Sedation for select patients only:
- Temazepam 60-90 min preop
- Ativan 90 min preop
- Midazolam 10 min preop
- Ketamine 10-15 min preop
- Antibiotic prophylaxis is usually ordered by the surgeon to prevent postoperative surgical site infection (SSI), but from an anesthesia perspective – antibiotic prophylaxis is used to safeguard against infective (bacterial) endocarditis in patients with prosthetic valves, previous infective endocarditis or congenital heart disease
- Multimodal analgesics – Acetaminophen orally for most patients, consider NSAIDS unless contraindicated
- Narcotics for pain control – it is important to not withhold the patient’s usual dosing of narcotic – especially if the surgery is delayed for any reason
- Heparin – subcutaneous heparin for DVT prophylaxis
- Oral anticoagulants – patients should stop their oral anticoagulants prior to surgery to prevent undue bleeding: Warfarin – stopped 4-5 days prior; Unfractionated heparin – stopped 4 hours prior; Low molecular weight heparin (LMWH) – stopped 12 -24 hours prior (depending on the dose); Plavix – stopped 7 days prior. The patient must have an INR prior to commencement of surgery or administration of a neuroaxial technique (spinal or epidural anesthetic). The INR result will determine what type of anesthetic can be given and if surgery will commence or in emergent cases fresh frozen plasma may be given to achieve a safer INR.
Review of the Peripheral Nervous System and its Effects on Pharmacology #
Pharmacology of the Peripheral Nervous System #
The body’s nervous system is divided into the:
- Central nervous system – brain and spinal cord
- Peripheral nervous system – somatic (voluntary control of skeletal muscle) and autonomic nervous system (involuntary control).
The neuron pathways of the peripheral nervous system are composed of pre-ganglionic and post-ganglionic neurons – the ganglion is a cluster of nerve cell bodies located outside of the CNS (see below). Transmission of impulses is accomplished by chemical neurotransmitters that are secreted at the terminals of the pre- and post-ganglionic fibers. These neurotransmitters interact with receptor sites on the various effector organs (target) to elicit or inhibit a response.
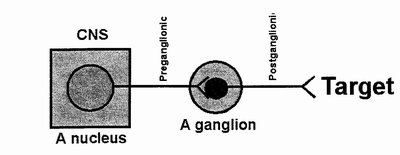
The somatic nervous system consists of sensory and motor neuron pathways and result in the voluntary control of skeletal muscle (and also reflex arcs – automatic responses to certain stimuli).
The autonomic nervous system is further divided into the sympathetic (SNS or adrenergic) and parasympathetic (PSNS or cholinergic) nervous systems. Most organ systems in the body receive both sympathetic and parasympathetic innervation although not always in equal proportion.
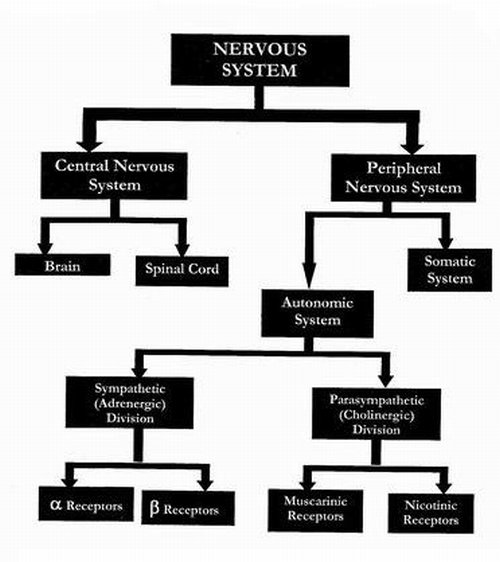
It is not the intent of this module to give a full synopsis of the peripheral nervous system. Please review any anatomy textbook regarding the location of the nerve fibers – in relation as to how they exit the spinal cord and the length of their pre- and post-ganglionic fibers. It is however, important to note what type of neurotransmitters each utilizes.
The two major neurotransmitters of the peripheral nervous system are Acetylcholine (Ach) and Norepinephrine (NE).
The efferent and afferent fibers of the somatic nervous system release Acetylcholine. The receptors are basically nicotinic in nature.
All pre-ganglionic fibers of the ANS release Acetylcholine. Post-ganglionic fibers may release either Acetylcholine or Norepinephrine.
The sympathetic nervous system post-ganglionic fibers release Norephinephrine. Sympathetic receptors include alpha (α), beta (β) and dopaminergic receptors. Sympathetic neurons are widely distributed throughout the body and as a result, activation produces a diffuse physiological response – a mass reflex (fight or flight response).
The parasympathetic system uses Acetylcholine at its post-ganglion fibers. There are two types of cholinergic receptors – nicotinic and muscarinic. Activation of the parasympathetic system tends to produce discrete, single organ responses.
The parasympathetic and sympathetic nervous systems usually have an opposite effect on a given organ. In the normal resting state, equilibrium exists between the two. In anesthesia and anesthetic recovery, specific drugs may either stimulate or inhibit activity of either branch and cause an imbalance in the system (see diagram below). The ANS effects of a drug may be primary (i.e. Atropine is given to treat bradycardia) or secondary/side effect (i.e. bronchospasm after giving a β-blocking drug).
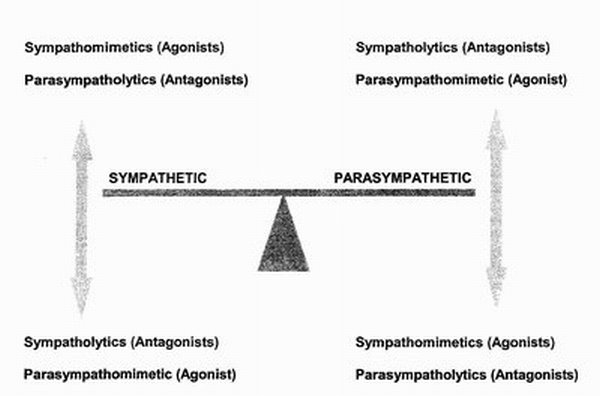
The major drug classifications that impact on autonomic equilibrium are:
- Sympathomimetics (sympathetic agonists): drugs that have similar actions to the post-ganglionic fibers of the SNS (i.e. resemble Norepinephrine). Classified according to action on the SNS receptors – α, β and dopaminergic receptors.
Most sympathomimetic drugs activate both the α and β receptors, but some have pure α-receptor effects (i.e. Phenylephrine) and some have pure β-receptor effects (i.e. Isoproteronol). Drugs are usually given to increase blood pressure by improving heart rate, contractility and systemic vascular resistance (depending on the receptor involved).
- Sympatholytics (sympathetic antagonists): drugs that oppose the actions of the post-ganglioic fibers of the SNS. Sympatholytics work by blocking either α or β receptors.
Familiar drugs are β-receptor antagonists (Beta blockers) such as Metropolol and Proprandolol used to manage cardiac conditions such as post-MI and hypertension. Alpha-receptor antagonists are less common but are used for their vasodilating properties (i.e. Phentolamine).
- Parasympathomimetics (parasympathetic agonists): drugs that stimulate post-synaptic muscarinic receptors (i.e. resemble Acetylcholine).
The muscarinic receptors are the main target of drugs that act directly on the PSNS. Direct acting muscarinic agonists are seen infrequently (i.e. Pilocarpine is used to topically treat glaucoma).
Drugs that have an indirect effect (agonist) are more common. These drugs are used extensively in anesthesia to reverse neuromuscular blockade (after administration of muscle relaxants). They inhibit the breakdown of Acetylcholine and increase neuromuscular transmission – two such drugs are Edrophonium and Neostigmine.
- Parasympatholytics (parasympathetic antagonists): drugs that oppose PSNS action at the muscarinic receptor by blocking the actions of Acetylcholine. These drugs are mostly muscarinic receptor antagonists – they interfere with the action of Acetylcholine at muscarinic receptor sites.
These drugs are used to treat symptomatic bradycardia and to reduce oral and respiratory secretions. They are also given in conjunction with the parasympathomimetic drugs mentioned above (Neostigmine) as these anti-cholinergic drugs (i.e. Atropine and Glycopyrrolate) will deal with Neostigimine’s muscarinic effects (bradycardia, excessive salivation and ↑ peristalsis). Low dose effects include reduced salivation and bronchial secretions, but at higher doses dilated pupils and tachycardia are seen.
Spinal Anesthetic Block #
Spinal Anesthetic Block #
The step-by-step sequence to administering a spinal anesthetic block is as follows:
1.The anesthesiologist will cleanse the patient’s skin with antiseptic solution. The anesthesiologist will then landmark the iliac crest and spinous processes of the spine; the iliac crest is level with the L4 spinous process. They will then count up or down to determine which level they wish to inject the local anesthetic. The level of spinal needle placement is based on knowledge of which nerve roots innervate dermatomes in the body.
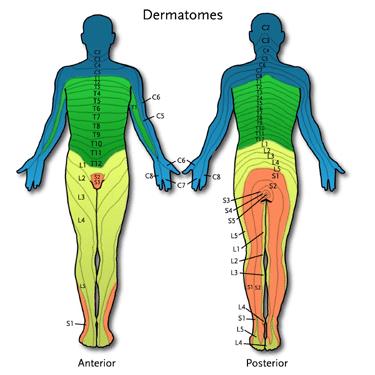
2.
A nerve block that is too high (above the level of the T4 vertebra) can interfere with the intercostal muscles and spontaneous breathing. This presents a dangerous situation as the patient is often receiving a spinal anesthetic to avoid a general anesthetic. Emergency intubation may be required.
3.
Once the right level on the spine is determined (i.e. L4 vertebra), the anesthesiologist will feel for the interspace between the vertebras above or below the selected vertebra (i.e. L3-4 or L4-5 interspace). A 30 gauge (G) 5/8″ needle is used to inject local anesthetic intradermally and a 25 guage 1 1/2 ” needle is used for a deeper injection. This provides local infiltration of the area and the patient does not feel pain during the insertion of the spinal needle. The patient will feel pressure only
4. The spinal needle is a fine needle (22, 25 or 27 gauge) with a sharp tip (Quincke or Whitacre) and is about 3 1/2″ long. The spinal needle is inserted via a midline or paramedian approach to the identified interspace, and advanced through the skin, spinous ligaments (supraspinal, interspinal and ligamentum flavum), the epidural space and finally through the dura mater into the subarachnoid space. This may take some time as some patients have stenotic (narrowed) vertebrae making it difficult to find and enter the interspace. Once the needle has traversed the dura, a distinct “pop” is felt in the anesthesiologist’s fingers and confirmed by the presence of CSF dripping out of the needle hub (see picture below). In elderly patients, the CSF pressure may be low and it may take a moment to for the CSF to appear.
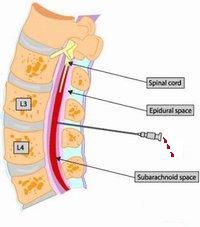
5.The syringe containing the local anesthetic is checked to make sure it is free of air bubbles and then attached to the hub of the spinal needle. Prior to injection, the anesthesiologist will aspirate about 0.2 ml of CSF to ensure proper placement. The drug is injected, CSF is aspirated a second time and the needle and syringe are removed.
Epidural Anesthesia Block Sequence #
The sequence to administering an epidural anesthetic block is as follows:
Epidural Anesthesia #
The sequence to administering an epidural anesthetic (block) is as follows:
1. Position the patient as you would for a spinal anesthetic. Follow the sequence for administering a spinal anesthetic: Steps 1-3.
2.The needle used for an epidural differs from a spinal needle in that it has a blunt tip, has a wider bore (to introduce the epidural catheter through it) and is approximately 3 1/2″ long. The needle is placed through a midline or paramedian approach to the identified interspace, and advanced through the skin and spinous ligaments (supraspinal, interspinal and ligamentum flavum). A syringe of saline is attached to the hub of the needle, and the needle is advanced further into the epidural space. Continuous pressure is placed on the barrel of the syringe as the needle is advanced. The epidural space is a potential space, therefore when the needle advances into the epidural space there will be a sudden loss of resistance and the syringe barrel will be easily depressed. This is called the loss-of-resistance technique: pictured below.
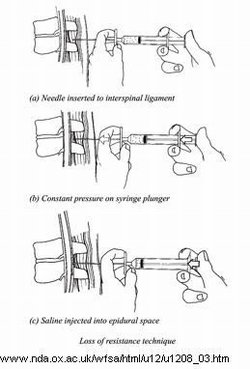
3. Once the needle is in place, the epidural catheter will be threaded through the needle. If it advances easily, the needle placement is assumed to be in the correct location. The catheter is inserted to a depth of 7″. The catheter is taped to the patient’s skin (according to the anesthesiologist’s preference) in such a way that kinking of the catheter is avoided.
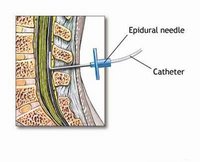
4.A filter is placed onto the end of the catheter to prevent bubbles or debris from entering the catheter. The catheter is aspirated to ensure that there is no CSF return. A test dose is given via the catheter to ensure that the appropriate level of blockade is achieved and that the catheter is in the correct position. The sequence of blockade is similar to a spinal anesthetic. A higher dose of anesthetic drug must be administered as it must traverse through the spinal meninges to affect the spinal nerves. Extreme care must be taken to prevent the catheter tip from advancing past the dura mater and allowing the large dose of local anesthetic to be injected into the CSF.
5.Further injections will be given via the catheter during the surgical procedure, depending on the length of the procedure. Alternatively, a dose will be given at the beginning and at the end of the procedure for post-operative pain control. In the PAR, a continuous infusion will commence to provide post-operative analgesia. The catheter is usually kept in place for up to five days post-operatively and will be monitored by an anesthesiologist on the surgical ward.
Cardiac Arrest #
Learning Objectives #
At the end of the module the nurse will be able to:
- Describe the heart’s conduction system.
- Recognize and list the causes of certain life threatening heart rhythms.
- Understand how to respond to a respiratory and a cardiac arrest.
- Identify the common medications used in a cardiac arrest.
- Recognize the roles of nursing in a cardiac arrest.

Definitions #
Definitions #
Patients undergoing surgical intervention are at risk for cardiac arrest due to the potential complications of surgery. The perioperative nurse has a professional responsibility to understand the complexities of a cardiac arrest and its treatment. The following definitions distinguish between a cardiac arrest, respiratory arrest, and code blue.
Cardiac Arrest #
A cardiac arrest is the sudden, abrupt loss of normal blood circulation due to the failure of the heart to function. Sudden death may occur within minutes after symptoms appear. Ventricular fibrillation (VF) constitutes the most common electrical mechanism in cardiac arrest and is responsible for 65 to 80% of occurrences. Another 20-30% of cardiac arrests are caused by severe bradyarrhythmias, pulseless electrical activity (PEA) and asystole. Other causes of cardiac arrest are associated with impaired circulation due to a state of shock.
Respiratory Arrest #
Respiratory Arrest is the cessation of the normal tidal flow of the lungs due to any number of respiratory failure mechanisms. Respiratory arrest is a medical emergency and may be related to or coincide with a cardiac arrest. Cardiac arrest may quickly follow a prolonged respiratory arrest because progressive hypoxemia impairs cardiac function. Respiratory arrests are less prevalent in the operating room because most patients are usually intubated and mechanically ventilated.
Code Blue #
“Code Blue” is one of many standardized hospital emergency codes. A Code Blue is called to alert staff that an emergency situation has occurred. A Code Blue is often called due to cardiac or respiratory arrest, but may also be called for a real or suspected imminent loss of life. A Code Blue can be called if any immediate and urgent treatment and/or back up are required.
Causes of Cardiac Arrest in the Operating Room #
Causes of Cardiac Arrest in the Operating Room #
Many factors (single or in combination) can contribute to a cardiac arrest in the operating room. Factors that may lead to cardiac arrest include:
- Surgical management
Surgical management problems may include: uncontrollable hemorrhage, error in technique (surgeon accidentally nicks an artery), air embolism or cerebral vascular accident.
- Anesthetic management
Anesthetic management problems may include: improper premedication, improper management of anesthetic, inadequate ventilation, myocardial depression, complication of regional techniques, aspiration, technical failure, failure to secure an airway, administration of the wrong anesthetic gas, and improper management of the immediate postoperative period (ventilation).
- Intraoperative pathological events
Intraoperative pathological events may include: coronary ischemia mainly due to coronary vasospasm, arrhythmias, pulmonary embolism, and other conditions.
- Preoperative complications
Preoperative complications may be due to pre-existing conditions such as allergies, coronary artery disease, cardiomyopathy, hypokalemia, digitalis toxicity, severe myocardial depression, peritonitis, severe trauma, ruptured aortic aneurysm, abdominal hemorrhage, inhalation of blood and/or gastric contents, pulmonary embolus during induction, intracerebral hemorrhage, cerebral edema and meningitis.
Events Leading to a Cardiac Arrest #
There are certain events that may lead to a cardiac arrest in the operating room because they trigger the patient’s vasovagal responses during surgery. A vasovagal reaction activates the body’s parasympathetic nervous system and inhibits the body’s sympathetic nervous system leading to vasodilation and bradycardia. This response may occur during:
- Tracheal suctioning
- Intubation and extubation of the endotracheal tube
- Downward traction of the stomach or manipulation of the abdominal viscera
- Manipulation of the abdominal organs, common bile duct, and gallbladder
- Postural changes
- Pressure from positioning equipment or turning the patient under anesthesia
- When traction is placed on the peritoneum during closure
- Eye procedures (stabismus, scleral buckle, pressure on the eye)
- Patient with undue fear or apprehension
- Injection of contrast dye during an angiography
- Removal of aortic clamps during a surgery
- Placement of a Cardiac Catheter (Pulmonary Aortic) in the right ventricle.
Treatment includes the restoration of venous return and correction of blood volume deficits.
Heart Rhythms #
To understand the implications of arrhythmias on the patient, the perioperative nurse must have a working knowledge of cardiac anatomy, physiology, and electrophysiology. Please refer to the ECG interpretion module for more information on waveforms and a normal sinus rhythm.
Normal Heart Rhythm #
The heart’s rhythm is coordinated by special tissue in the myocardium which forms its conduction system. With each heartbeat, the electrical impulse begins at the sinoatrial or SA node. The SA node is also called the heart’s natural pacemaker. The SA node is a cluster of specialized cells, located in the right atrium. The SA node produces the electrical impulses that set the rate and rhythm of a heartbeat. The impulse spreads through the walls of the right and left atria, causing them to contract (atrial contraction), forcing blood into the ventricles. The impulse then reaches the atrioventricular (AV) node, which acts as an electrical bridge allowing impulses to travel from the atria to the ventricles. There is a short delay before the impulse continues it’s journey along the interventricular septum via two branches of fibres called the Atrioventricular bundle (Bundle of His). The actual contraction of the ventricles (ventricular contraction) is stimulated by the Purkinje fibres that emerge from the bundle branches and pass into the cells of the myocardium. This contraction forces blood out of the heart to the lungs and body. The SA node fires another impulse and the cycle begins again.
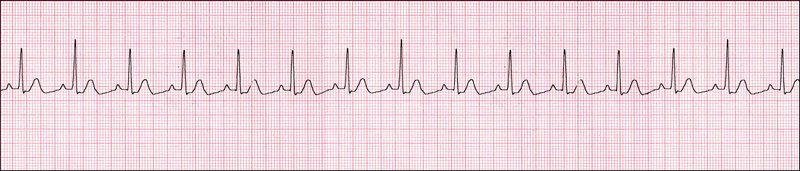
Arrythmias #
An arrhythmia is an irregular or abnormal heartbeat. It can be referred to as a dysrhythmia or an irregular heart rhythm.
Most cardiac arrests occur when the electrical impulses of the heart become rapid, chaotic or both. Some arrests are due to extreme slowing of the heart (bradycardia). An irregular heart rhythm or arrythmia can cause the heart to suddenly stop beating (asystole).
Common arrythmias causing cardiac arrest in the OR include:
Ventricular Fibrillation (V-fib) – Most common cause of cardiac arrest in the OR.
V-fib is an erratic, rapid and irregular firing of impulses from the ventricles. The ventricles quiver and cannot generate an effective contraction, making the heart unable to deliver blood to the body. V-fib may be caused by hypoxia, electrolyte imbalance, and shock.
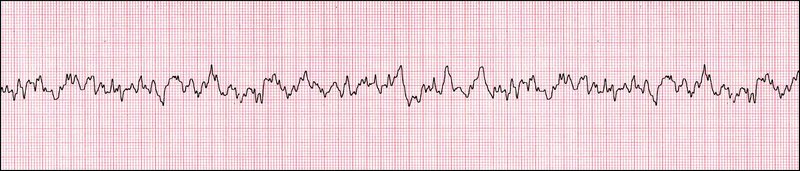
Treatment: V-fib is treated with CPR, defibrillation, and IV drug therapy.
Asystole
Asystole is cardiac standstill with no cardiac output and no ventricular depolarization.

Treatment: Asystole is treated with CPR, 100 % oxygen, Epinephrine and Atropine.
Atrial Fibrillation
Atrial Fibrillation is a very common irregular rhythm. Many impulses begin and spread through the atria, competing for a chance to travel through the AV node. The resulting rhythm is disorganized, rapid and irregular because the impulses are traveling through the atria in a disorderly fashion, there is a loss of coordinated atrial contractions. Pulse ranges from 160 to 180 bpm. Waveform is denoted by the lack of a P wave. Atrial Fibrillation may be caused by hypotension, stress, alcohol, caffeine, hypoxia, and a pulmonary embolism.
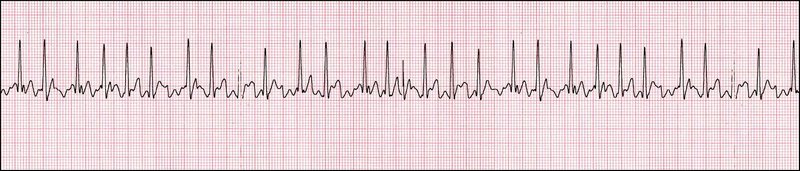
Treatment: Atrial fibrillation is treated with oxygen, Digoxin, synchronized cardioversion and anticoagulant therapy.
Atrial Tachycardia
Atrial Tachycardia is a rapid heart rhythm that originates from the atria with atrial rhythm between 100-180 beats per minute.
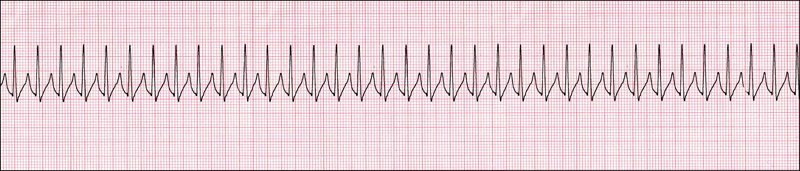
Treatment: Atrial Tachycardia is treated with oxygen and correcting underlying cardiopulmonary process, toxicity, or metabolic abnormality.
Atrial Flutter
Atrial Flutter is an atrial arrhythmia due to one or more rapid circuits in the atrium. It is usually a regular rhythm beating at a extremely fast rate (300+ bpm). The waveform is denoted by its sawtooth appearance. Atrial Flutter may be caused by heart-valve disease, coronary artery disease, thyroid disease, swelling or irritation near the heart and heart failure.
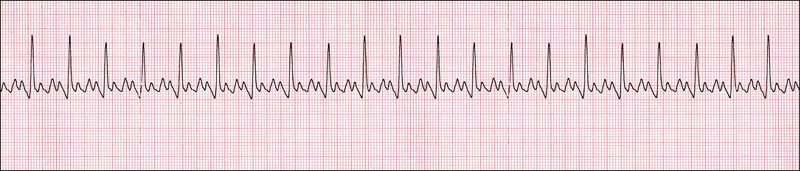
Treatment: Atrial Flutter is treated with cardioversion, pacing and antiarrythmics.
Ventricular Tachycardia (V-tach)
V-tach is a rapid but regular rhythm originating from the lower chambers of the heart. This rapid rate prevents the heart from filling adequately with blood, and less blood is pumped through the body. V-tach may be caused by an acute myocardial infarction, congested heart failure or coronary artery disease.
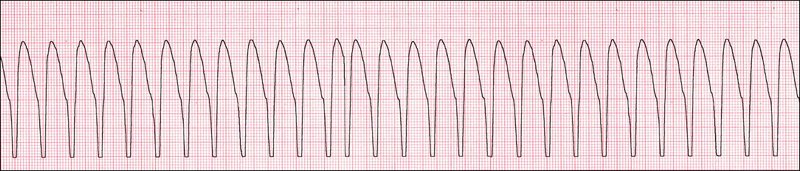
Treatment: V-tach is treated with Procainamide (drug of choice) with cardioversion and IV drug therapy.
Pulseless Electrical Activity (PEA)
Any rhythm without a pulse can be called a pulseless electrical activity (PEA). Usually it is a fast ventricular tachycardia. It could present as a supraventricular tachycardia (SVT), but this is less likely to cause a PEA. If untreated, the PEA soon progresses to ventricular fibrillation or asystole. The EKG can resemble many different rhythms, the differentiation being that no pulse will be recorded. Correction of metabolic abnormalities like acidosis, hypokalemia and hypomagnesemia help prevent recurrence.
Treatment: Defibrillation – If it is a shockable rhythm like ventricular tachycardia or fibrillation. If it is asystole, see treatment as above.
Premature Ventricular Contractions (PVC’S)
PVCs are early, extra beats (ectopic beats) caused by early depolarization of either ventricle. PVCs are common. Most of the time they cause no symptoms and require no treatment. In some people, they can be related to stress, too much caffeine or nicotine, or exercise. But sometimes, PVCs can be caused by heart disease or an electrolyte imbalance.
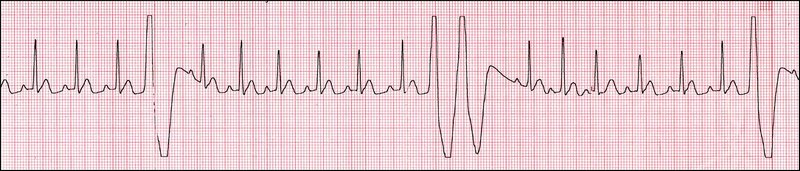
Treatment: There is usually no treatment for PVCs unless symptomatic. If treated, Lidocaine is used.
Sinus Tachycardia
Sinus Tachycardia is an acceleration of the SA node beyond a normal discharge rate resulting in a heart rate of over 100 bpm.
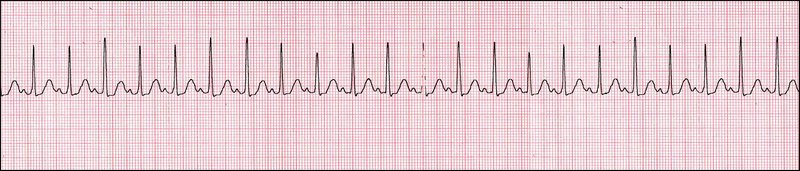
Treatment: The treatment goal for Sinus Bradycardia is to reduce the heart rate by treating the symptoms.
Sinus Bradycardia
Sinus Bradycardia is deceleration of the SA node below a normal discharge rate resulting in a rate below 60 bpm.
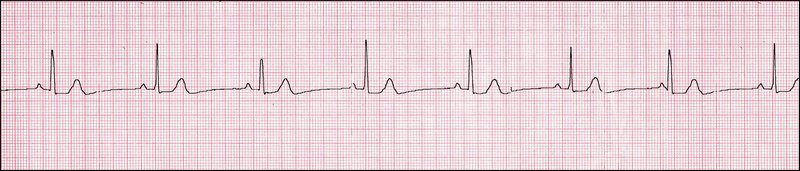
Treatment: Sinus Bradycardia is treated with IV Atropine.
Defibrillation #
Defibrillation #

Defibrillation is a process of administering an electric shock to the heart to re-establish normal contraction rhythms in a heart having dangerous arrhythmia. Defibrillation is not effective if the patient is in asystole. The electrical shock is measured in Joules (J).
Biphasic Defibrillation #
Until recently, external defibrillators relied on monophasic shock waves. Electrical pulses are sent rapidly from one electrode to the other, only in one direction.
Biphasic defibrillation, however, alternates the direction of the pulses, completing one cycle in approximately 10 milliseconds. When applied to external defibrillators, biphasic defibrillation significantly decreases the energy level necessary for successful defibrillation. This, in turn, decreases risk of burns and myocardial damage. Biphasic defibrillation may start at 120J, 150J or 200J and gradually increase in these increments or start at 200J (hospital specific) – or 2-5J/kg for pediatric patients.
Cardiac Pacing #
Cardiac pacing refers to the process where an electronic device called a pacemaker is used to treat patients who have symptoms caused by abnormally slow heartbeats. A pacemaker is capable of keeping track of the patient’s heartbeats. If the patient’s heart is beating too slowly, the pacemaker will generate electrical signals similar to the heart’s natural signals (SA node), causing the heart to beat faster. The purpose of the pacemaker is to maintain heartbeats so that adequate oxygen and nutrients are delivered through the blood to the organs of the body. The pacemaker can be preset to trigger an impulse if the heart beats less that a predetermined rate (this is called demand mode). The defibrillator has the capacity to externally pace a patient during surgery (external defibrillator pads). Temporary pacing can also be achieved for longer periods of time (i.e. postoperatively) with the use of a special pacing pulmonary catheter or with pacing wires sutured to the patient and attached to a pacer box.
Cardiac pacing is often used to treat patient’s with atrial fibrillation and atrial flutter during surgery or in the preoperative area.
Synchronized Cardioversion #
Cardioversion refers to the ability to revert an arrythmia (i.e. atrial fibrillation) back to a more regular rhythm. This is achieved through synchronized cardioversion. Synchronized cardioversion occurs when the defibrillator is programmed to administer a shock only during the R wave of the patient’s cardiac rhythm thus avoiding the possibility of discharge on the vulnerable T-wave. By the end of the T wave, all the ventricular cells have returned to their normal polarized state; they are in a uniform state and “stable”. The “ECG portion” of the defibrillator searches for certain criteria such as slope and amplitude that distinguish an R wave from P or T waves. When an R wave is detected, the defibrillator monitor places a flag or sync marker on that R wave, and the defibrillator will fire. When in the synchronized mode (commonly referred to as ‘synch’ mode) the setting is usually 120-200J (or 0.5-1J/kg for pediatric patients).
If for any reason the patient’s rhythm changes (i.e. ventricular fibrillation where there is not R wave to detect) and they require defibrillation – the defibrillation machine must be taken out of the synchronized (or synch) mode in order to discharge properly.
Resuscitation Procedure #
Cardiopulmonary Resuscitation Procedure #
Cardiac or respiratory arrest may occur in patients undergoing surgery because of the potential complications of surgery including hemorrhage, shock, or unfavourable reactions to anesthesia. Cardiopulmonary resuscitation (CPR) is the immediate restoration of circulatory and respiratory functions by mechanical or manual methods and includes the administration of drugs to stimulate ventilation and cardioversion to a normal sinus rhythm. In a cardiac arrest, CPR is critical for the patient’s survival. All perioperative nurses must have current CPR certification.
Resuscitation Procedure for a Cardiac Arrest in the Operating Room #
The resuscitation protocol for a cardiac arrest in the operating room must be clearly understood by all operating room staff. The primary priorities in a cardiac arrest are:
- AIRWAY management
- CHEST COMPRESSIONS, defibrillation if required
- Treatment of any dysrhythmias.
The hospital’s code team may not be called to the perioperative areas. The operating room staff is expected to assume the role of the code team. When a cardiac arrest occurs in the operating theater, the anesthesiologist takes charge of the resuscitation.
Role of the Circulating Nurse #
It is crucially important that the circulating nurse is a registered nurse in a cardiac arrest situation. Registered nurses are educated to perform the specialized duties (IV medication, defibrillation, etc.) that are life-saving during a cardiac arrest. The appropriate staff must be available to respond to a cardiac arrest in the operating room immediately.
The circulating nurse is the designated “In-Charge” nurse in a CODE BLUE situation. Other nurses will respond to the code but the circulating nurse will know the patient the best. The circulating nurse should always stay with the patient and control traffic in the room, ensuring that only essential staff is present. When a code blue is initiated (usually by the anesthesiologist), the circulating nurse is responsible for:
1. Calling for help with the emergency call system within the OR or perioperative area (CODE BLUE)
2. Ensuring CPR is initiated and providing assistance as needed.
3. Assisting the surgeon and anesthesiologist with resuscitation and defibrillation.
4. Assigning a nurse to be the “recording nurse” to document during the event
5. Delegating duties to other responders
Role of the Scrub Nurse #
The scrub nurse is responsible for:
1. Remaining sterile, moving sterile items out of the way, and maintaining the sterility of the sterile items unless additional assistance is required (then scrub out and assist).
2. Noting the start time of the CODE BLUE.
3. Quickly covering the incision site with a sterile drape or towel.
Role of other OR Personnel responding to the Code Blue #
The nurses or OR personnel responding to the code blue are responsible for:
- Bringing the cardiac arrest cart to the operating room or code blue location. Plugging in the defibrillator.
- Being the Recording Nurse (if assigned to do so).
- Assisting the anesthesiologist or surgeon in preparing drugs, blood transfusions, and treatments.
- Assisting and sending blood specimens to the lab.
- Acting as a runner to obtain supplies.
- Relieving rescuer performing chest compressions as required.
- Removing excess furniture and or equipment from area to allow more room.
Role of the Recording Nurse #
The recording nurse is responsible for:
1. Recording the times and events on the Resuscitation Record using the same clock or watch throughout the code. Confirm the start time with the anesthesiologist and the scrub nurse.
2. Noting the procedures, drugs, defibrillation and the patient’s response to the resuscitation.
3. Ensure that the Resuscitation Record is completed, signed, and copies filed correctly. Documentation should be logical and concise.
View the following example of one hospital’s resuscitation record in regards to the information it contains.
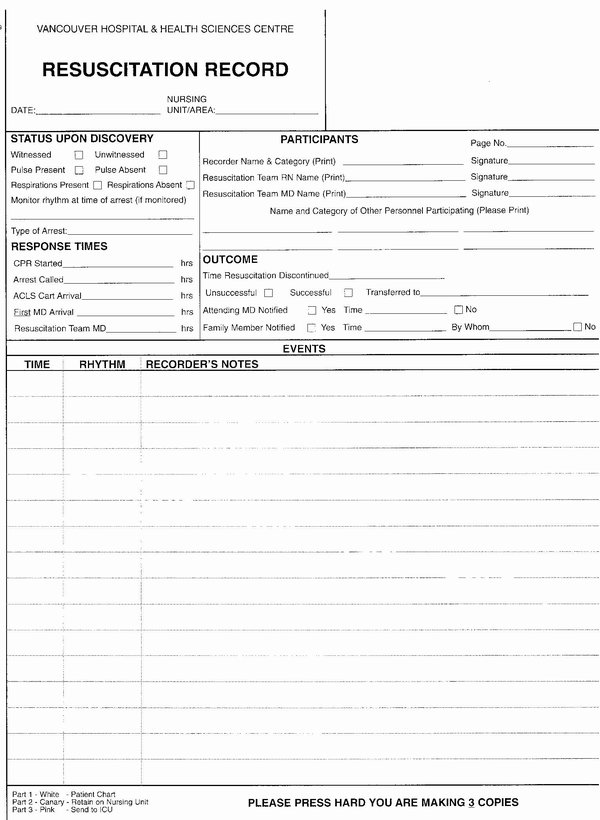
Drugs #
Emergency Code Cart #
The Emergency Code Cart contains medications that may be administered during a Code Blue. The circulating nurse may be responsible for reconstituting, drawing up or assembling medications for the anesthesiologist to administer during an emergency situation. It is the responsibility of the perioperative nurse to:
- Be familiar with the resuscitation drugs in the Emergency Code Cart. For an example of some commonly found drugs on an Emergency Code Cart, click here.
- To access an algorithm of the steps followed for advanced cardiac life support (of an adult), please click here (from the Heart and Stroke Foundation of BC & Yukon).
- Perform checks on the Emergency Code Cart to ensure that the defibrillator is in working order and all contents are present. The defibrillator is checked daily, certain functions are checked weekly and drawer contents are checked on a per use and/or monthly basis (i.e. drug out-dates).
Death in the Operating Room #
The nursing responsibilities for a death in the operating room are hospital-specific. It is important that the perioperative nurse understands the institution’s policy and procedure for caring for a deceased person in the operating room. Important considerations include:
1. The surgeon or anesthesiologist is responsible for pronouncing the death of the patient.
2. All OR deaths are coroner’s cases because it is an unexpected outcome. It is the surgeon’s responsibility to notify and speak to the coroner.
3. Do not remove any tubes or lines from the patient until cleared by the coroner.
4. Do not remove any drugs, supplies or equipment from the room until cleared by the coroner.
5. It is the surgeon’s responsibility to notify the patient’s relative(s) or significant other(s).
6. The family may wish to view the patient prior to sending the patient to the morgue. Prior to bringing the family in (and after clearance from the coroner), clean the OR and make patient as presentable as possible for viewing. Support the family in their grief; call in a social worker or chaplain if desired
7. Debrief, as a group, after the critical incident. A death can be traumatic for all involved.