Description
This unit will provide the student with the required knowledge (Pharmacology, indications, contraindications, action, onset duration and side effects) related to the common medications used in Procedural Sedation and Analgesia (PSA)
Learning Objectives #
At the end of the module the student must be able to :
a) understand the pharmacology of sedatives and analgesics
b) Identify the indications, contraindications, action, onset, duration and side effects of commonly used drugs in Procedural Sedation and Analgesia (PSA)
DEFINITION #
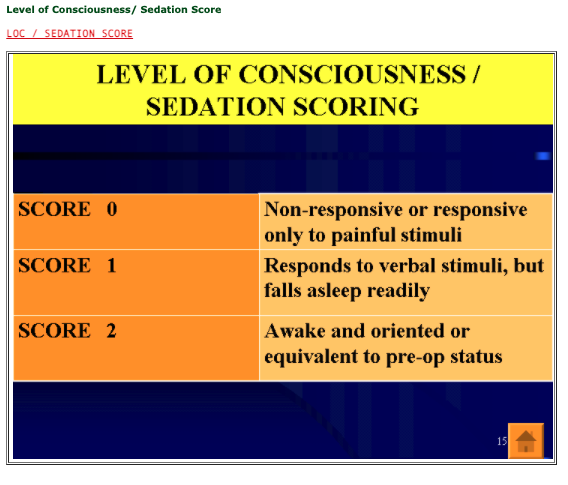
Sedation:
To minimally depress the level of consciousness using sedatives and/or narcotics, while retaining the patient’s ability to independently & continuously maintain an airway and respond appropriately to physical & verbal stimuli. Unconsciousness & unresponsiveness are not Objectives of Procedural Sedation!!!
MEDICATIONS #
- Procedural Sedation is achieved by administering pharmacological agents
- The most common route of administration is intravenous (IV), although medications may be given orally (P0), rectally (PR), intramuscular (IM), subcutaneously (SQ), or nasally. The most commonly used agents are benzodiazepines, narcotics, barbiturates, and certain hypnotics (such as Chloral Hydrate)
- The choice of sedative is largely operator dependent, but generally consists of benzodiazepines used either alone or in combination with an opiate. The most common benzodiazepines are Midazolam and Diazepam. Midazolam is favoured for its fast onset of action, short duration of action, and high amnestic properties
- Opiates, such as Meperidine or Fentanyl administered intravenously provide both analgesia and sedation
- Combinations of benzodiazepine and opioid agents are frequently used, especially for longer procedures. However, such combinations may increase the risk of desaturation and cardiorespiratory complications
- Specific antagonists of opiates (Naloxone) and benzodiazepines (Flumazenil (Anexate, Romazicon)) are available and should be present in every unit to treat over-sedated patients
- The patient should then be observed for several minutes to establish effectiveness of the dose given
- Desired results of the medication include slightly slurred speech and slow responsiveness with no respiratory distress or hypotension and a calm, relaxed state
- Infusion of additional drug can be given if needed at usually half the initial dose
#
MEDICATION IMPORTANT POINTS #
During Procedural Sedation, it is important to remember that we are trying to achieve is relaxation, amnesia, and analgesia with little hemodynamic variance and are rapidly eliminated from the body
- Titration of these medications to patient response will help maintain the patient in a “consciously sedated” state and decrease the complications associated with excessive dosing
- Despite careful titration and patient monitoring however, patients may still experience untoward reactions to medications
- Knowledge of a drug pharmacokinetics (i.e., absorption, distribution, metabolism and elimination) will greatly enhance your ability to anticipate the patient’s reaction(s) to the medications used
MEDICATION PHARMACOKINETICS
ABSORPTION
- Refers to the movement of a drug from the site of entry (i.e. IV, IM, SC) to another site, which is usually the blood stream. The rate and extent of absorption will determine the intensity and duration of the drug’s effects
- Factors influencing rate and extent of absorption include:
- Amount and depth of surface area for absorption
- Perfusion to the site of administration
- -Drug concentration
- -Drug pH
Clinical Considerations:
e.g. IM vs. inhalation administration
- Adequacy of blood flow
- Lipid soluble drugs are more easily absorbed than water soluble
- Passive transport occurs more readily with drugs that are more highly concentrated
- Drugs that are more similar in acid/base to body fluids will absorb more readily
DISTRIBUTION
- Refers to the transportation of the drug to its site of action (receptor sites on cell walls) following absorption into the bloodstream
Factors influencing rate and extent of absorption include:
- Cardiac output
- Regional blood flow
- Drug reservoirs: plasma protein (albumin) or tissue binding
Clinical Considerations:
- ↓CO may delay the drug effects due to extended distribution time
- Vital organs receive blood flows prior to periphery-drugs will follow same distribution
- Low serum albumin levels may result in ↑levels of circulating drug and risk of toxicity protein bound drugs will last longer in the system
- Lipid-soluble drugs have a greater affinity for adipose tissue- decreased elimination in obese patients
METABOLISM
- Refers to the enzymatic biotransformation the drug undergoes as it passes the various organs involved. The liver being the primary site for drug metabolism. Depending upon the drug and route of administration, the renal, pulmonary, plasma and intestinal mucosa may also be involved
Factors influencing rate and extent of absorption include:
- Drug reservoirs: plasma protein (albumin) or tissue binding
- Hepatic (or other organ(s) involved) function and blood flow
- Age variances
Clinical Considerations:
- ↑drug reservoir storage and protein binding will result in ↓metabolism of drug
- ↓hepatic perfusion will result in ↓metabolism of drug
- Very young or very old have ↓enzymatic function and therefore will have slower drug metabolism
EXCRETION
- Refers to the elimination of the drug from the body. The kidneys through glomerular filtration and active tubular secretion excrete most drugs. Other organs that may be involved include the GI tract and lungs
Factors influencing rate and extent of absorption include:
- Half-life of a particular drug
- Drug pH in relation to renal tubular fluid
- Age variances
- Hepatic and renal function
- GI function
- Pulmonary function
Clinical Considerations:
- The amount of time it takes for a drug’s serum concentration to fall by half of its original value
- The more similar the drug and renal tubular fluid pH, the more drug will be reabsorbed and therefore less excreted
- Very young or very old have ↓renal function = slower drug excretion
- ↓hepatic or renal function will ↑ half-life
- ↓pulmonary function will result in ↓elimination of drug from lungs
- Other factors to be considered in how a drug will be absorbed, distributed, and metabolized in the body have to do with the route in which a medication is administered and the properties of the medication itself
- The following table outlines the various routes and these implications
MEDICATION ROUTES AND IMPLICATIONS
Transmucosal(TM)
Includes: oral (po), sublingual (SL), nasal / rectal (PR)
• Less predictable gastric absorption with oral ingestion than with either nasal or rectal administration
• Quicker onset with nasal administration, but sneezing, swallowing and noxious sensation may all interfere with appropriate absorption
Intramuscular (IM) or subcutaneous (SM)
• Quicker onset than oral route
• More reliable absorption, longer duration of action
Inhalation
• Rapid onset & effect, ease of administration / patient cooperation required
Intravenous (IV)
•More reliable route, medication can be titrated to effect, shorter duration of action
•More reliable route, medication can be titrated to effect, shorter duration of action
Transdermal (TD)
•Ease of use, slower onset, titration difficult, effects continue after removal (? duration)
Techniques of administration #
TECHNIQUES OF ADMINISTRATION #
Three techniques to use:
•Titration to clinical effect technique
•Bolus technique
•Continuous infusion technique
1.Titration to clinical effect technique
Advantages:
•Allows careful titration of sedative / analgesic medications
•Reduces total medication requirement via synergistic action
•Provides for a slow, controlled rise in therapeutic plasma level
•May provide for more rapid patient recovery
Disadvantages:
•Requires appropriately trained personnel for administration
•Requires close monitoring
2. Bolus technique:
Advantages:
•Provides a rapid rise in therapeutic plasma level for short procedures.
•Provides a sedate/analgesic using predetermined mg/kg dosage.
Disadvantages:
•Rapid administration of sedative/analgesic medications may result in excess therapeutic plasma level.
•Respiratory obstruction, ventilatory depression, respiratory insufficiency, hypotension, bradycardia, and cardiovascular instability frequently occurs with excess plasma levels of medication
3. Continuous infusion technique:
Advantages:
•Permits constant plasma level through a continuous infusion of medication
•Once a therapeutic plasma level is achieved, continuous infusion technique avoids fluctuations in plasma levels
•May decrease recovery time secondary to reduction in total dose of medication administered
Disadvantages:
• Challenging for non-anesthesia practitioners to maintain an adequate airway in non-intubated patients
•Initial attempts to reach a therapeutic level may result in over sedation
• May be difficult to adjust initial continuous infusion rate based on the patient’s level of consciousness
BENZODIAZEPINES
· Benzodiazepines are used in the majority of procedures
· They can induce relaxation and cooperation and often provide an amnestic response
· Doses are titrated to patient tolerance based on factors such as patient age, weight, medical history, anxiety level, use of
additional medications, length and complexity of the procedure
· In addition to the desired effects, significant respiratory depression can occur. This effect is synergistically increased with
the use of intravenous opiates
· Benzodiazepines are metabolized primarily in the liver and generate active metabolites that are more slowly broken down
and excreted via the kidneys
· The duration of action of the drugs is variable and may extend beyond the predicted elimination half-life of the drug
· In addition to the desired effects, significant respiratory depression can occur. This effect is synergistically increased with
the use of opiates
Nursing Considerations:
· The individual response of the patient to the medication(s) along with the length of the procedure should determine the total
dose administered to the patient.
· It is important to remember that the dose should be reduced for:
1) Elderly or debilitated patients,
2) Patients with renal or hepatic disease
3) Patients receiving narcotics in addition to benzodiazepines (due to their additive effect)
· The administration of the benzodiazepines IV must be performed very cautiously as they can produce respiratory
depression
· The minimum dose that achieves the desired effect should be given
· A small initial dose should be given slowly IV push over 1 – 2 minutes
BENZODIAZEPINES -USE CAUTIOUSLY WITH:
· Renal/hepatic disease
· Sleep apnea
· Cardiovascular disease: Patients may have hypotension and tachycardia
· Patients with short neck
· Patients taking other CNS depressants
· Clients with open angle glaucoma
· Pregnant or nursing mothers
· Obesity
· Elderly patients
· Respiratory disease
SYMPTOMS OF BENZODIAZEPINE OVERDOSAGE:
· Include respiratory depression, apnea, hypotension, dysrhythmia, confusion, and stupor
· Treatment for benzodiazepine overdose is supportive
· Flumazenil has been shown to selectively block the binding of benzodiazepines to its receptor, resulting in reversal of
central nervous system (CNS) depression
· Patients who develop severe respiratory depression after being given an opioid agent and a benzodiazepine should
generally receive Naloxone (Narcan) before being given Flumazenil (Anexate)
· Acute withdrawal, including seizures, may be precipitated after administration of Flumazenil (Anexate) to patients
receiving long-term benzodiazepine therapy
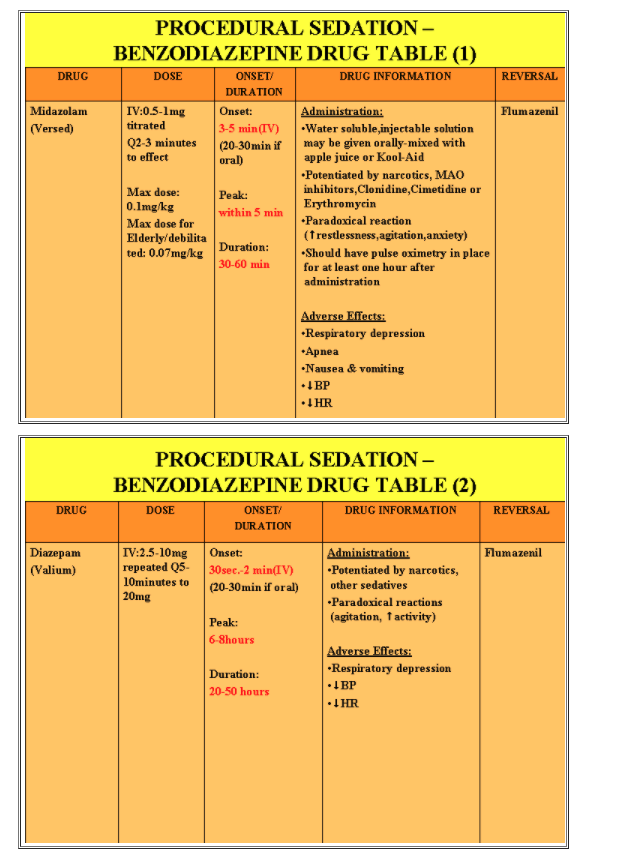
MIDAZOLAM (Versed)
· Is a short acting benzodiazepine CNS depressant. It is indicated for Procedural Sedation prior to short diagnostic or
surgical procedures, either alone or with a narcotic
· Midazolam binds to benzodiazepine receptors on the postsynaptic gamma-aminobutyric acid (GABA) within the central
nervous system, resulting in sedative, anticonvulsant, muscle relaxant, anti-anxiety and amnesic activity
· Midazolam is a potent sedative agent that must be given slowly!!!!
· Contraindicated in patients with a known hypersensitivity or a history of glaucoma because of a possible anticholinergic
effect
· Should not be used in patients with acute alcohol intoxication and with caution with delirious patients or patients on other
CNS depressant medications
· Midazolam has no analgesic, antidepressant, or antipsychotic properties
· Midazolam has been found to cross the placenta and is not recommended for use during pregnancy
· It also enters breast milk and is not recommended for nursing mothers
· May cause hypotension if given too quickly
· Reversed by Flumazenil (Anexate, Romazicon)
· It may cause paradoxical excitation, particularly in the elderly
· It may be administered IV, IM, P0, rectally, or nasally. The most common route of administration is IV
Suggested dose:
0.5-1.0mg IV direct over 2 minutes,may give additional doses in small increments Q 2 minutes to effect to max 0.1mg/kg. (For elderly/debilitated patients: max = 0.07mg/kg)
Side effects:
· Apnea
· Hypotension
· Nausea & vomiting
· Coughing
· Drowsiness
· Confusion
· Anterograde amnesia
Nursing Considerations:
· May cause hypotension, bradycardia or cardiac arrest if given too quickly
· Is 1.5-2 times more potent than Diazepam
· Respiratory depression, hypotension and apnea occur more frequently in patients who have been premedicated with
narcotics or other CNS depressants
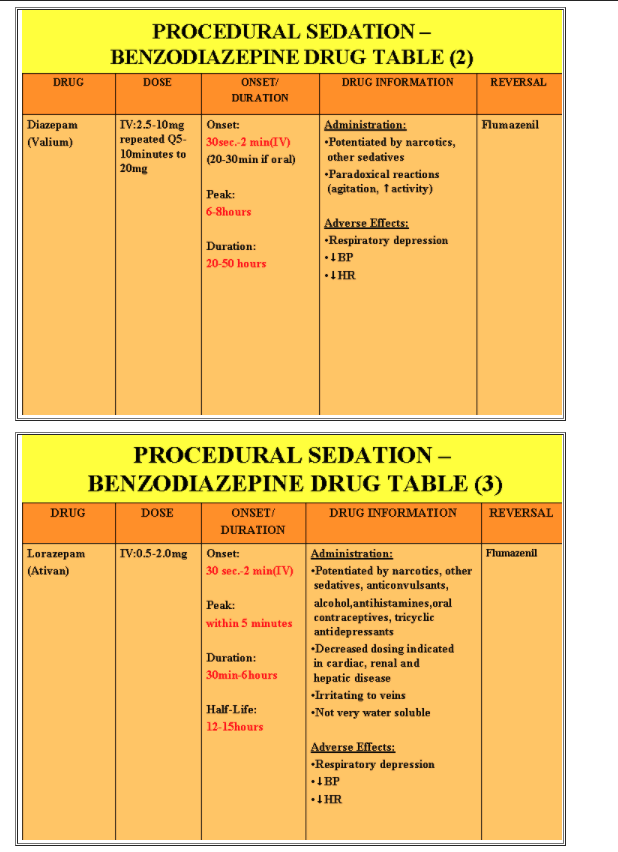
DIAZEPAM (Valium)
· Has similar properties to Midazolam, although it has a longer half-life, a greater chance of phlebitis and less
amnestic capabilities
· It has been replaced for the most part by Midazolam but is still used occasionally for Procedural Sedation and as a
premedication for non-painful procedures
· Used alone or with a narcotic
· This drug is most useful as an anti-seizure medication
· It may be administered IV, IM, PO although IM administration is very painful and not recommended
Suggested dose:
2-10mg IV over 5 -10 min. to a maximum of 20mg
Nursing Considerations:
· Diazepam is extremely irritating to the tissue and should be injected through a large vein
· It cannot be mixed with other medications or diluted due to precipitation
· It should be injected as close to the IV cannula as possible
· Use with caution with the elderly, obese or in patients with hepatic failure
Potential hazards:
· Thrombophlebitis
· Pain at the injection site
· Desquamation at injection site
With rapid administration:
· Severe hypotension
· Bradycardia
· Respiratory depression
· Cardiac arrest
LORAZEPAM (Ativan)
· For short term relief of acute anxiety
· Premedication for relief of anxiety and production of amnesia prior to a procedure/surgery
Nursing Considerations:
· 5 –10 times as potent as Diazepam
· Useful for procedures > 2 hours
Suggested Dose:
0.5-2.0 mg IV Q15 min. prior to procedure, repeat ½ the original dose q10min to max of 4mg
Side effects:
· Pain, burning and redness at the injection site
· Dizziness
· Vertigo (more pronounced in the elderly)
· Anterograde amnesia
· Hypotension or hypertension
· Excessive drowsiness
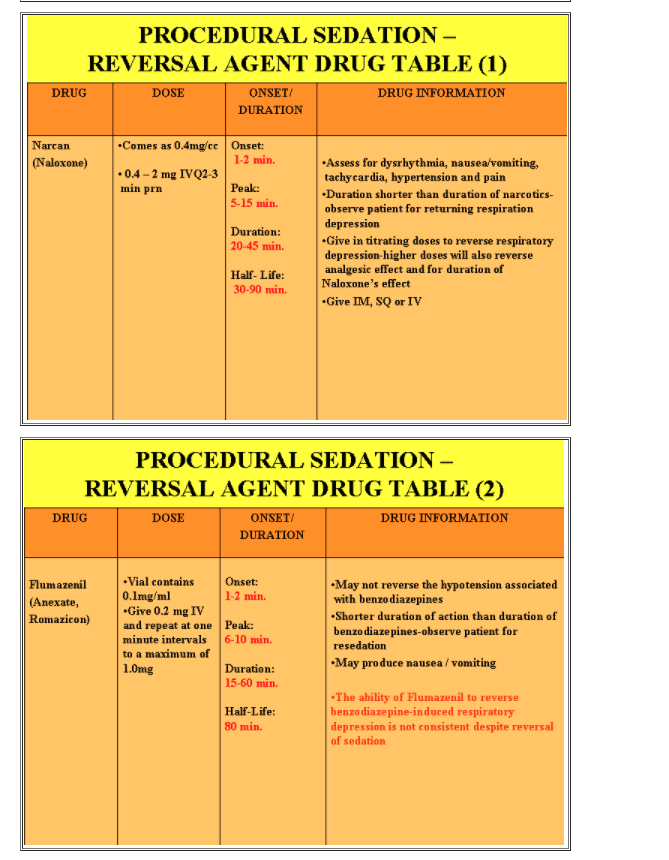
BENZODIAZEPINE REVERSAL AGENTFLUMAZENIL (Anexate, Romazicon)
· Is a benzodiazepine antagonist and should be readily available in all patient care units where benzodiazepines are given
· Will reverse the central nervous system effects of the benzodiazepines
· The duration of antagonism however, is relatively brief and the dose may need to be repeated
· May produce nausea / vomiting
· Reverses sedation without reversing amnesia
· Can cause acute anxiety if given too quickly
· The ability of Flumazenil to reverse benzodiazepine-induced respiratory depression is not consistent despite reversal of
sedation
· Vial contains 0.1mg/ml
· Give 0.2 mg IV and repeat at one-minute intervals to a maximum of 1mg.
· Onset: 1-2 min.
· Peak: 6-10 min.
· Duration: 15-60 min.
· ½ life: 80 min.
Narcotics fall into the categories of:
1) Opioid
2) Synthetic opioid analgesics
- They may be classified as agonists, mixed agonists-antagonists, or partial agonists by their activity at the opioid receptors.
- Opioid drugs bind to specific receptor sites which are unevenly distributed throughout the central nervous system with highest concentrations found in the limbic system, hypothalamus, midbrain, and spinal cord
- Narcotic agents alter both the perception of pain and the emotional response to painful experiences
- The most commonly prescribed narcotic agents used for PSA are: Fentanyl Citrate, Morphine, Hydromorphone and Meperidine
- These drugs primarily affect the Central Nervous System and GI Tract, producing pain relief or analgesia, mood changes, delirium, sedation, respiratory depression, decreased gastric motility, and an inability to concentrate
- Alterations in the endocrine and autonomic nervous system may also be seen
- These agents are metabolized in the liver and excreted in the urine
- The differences in onset and duration of the opiates can be attributed to their affinity for the receptors, their lipid solubility (reflecting their ability to cross the blood brain barrier), half-life, and the presence or absence of active metabolite
- The dosage should be reduced for geriatric and pediatric patients or patients with renal, hepatic, or pulmonary disease
- Must be used cautiously in patients taking other central nervous system depressants, such as other narcotic agents, sedatives, tranquilizers, phenothiazines, and antihistamines.
- Most of the drug interactions with monoamine oxidase (MAO) inhibitors have been described with Meperidine
- Other narcotics should also be avoided in patients on an MAO inhibitor when or in patients currently receiving benzodiazepines or other CNS depressants
- Narcotics will also lower the seizure threshold in patients with a history of a seizure disorder, and the dose should be lowered accordingly
- Since the administration of narcotics can result in respiratory depression and in some circumstances cardiac depression they must be administered cautiously
- The minimum dose that achieves the desired effect should be given
- The individual response of the patient to the medication(s) along with the length of the procedure should determine the total dose administered to the patient
Narcotic use –Nursing Considerations:
- Reduce dosage in the elderly
- Resuscitation equipment must be readily available
- Antidote: Naloxone
- Use with caution in patients with convulsive disorders, cranial injuries, respiratory insufficiency, cardiac arrhythmias and reduced blood volume
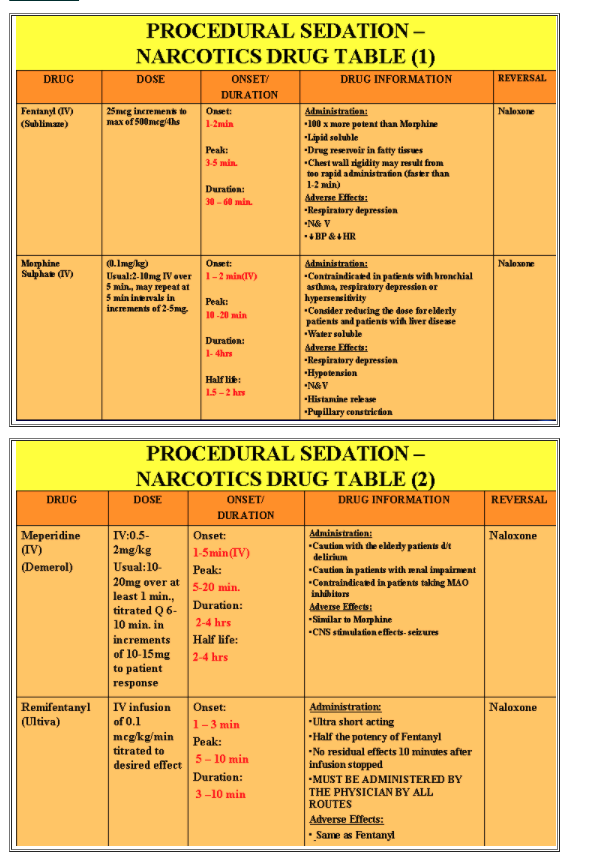
FENTANYL (Sublimaze)
- Is a synthetic opioid
- Produces decreased pain sensation, sedation, euphoria and a decreased awareness
- Used in conjunction with sedatives for pain relief
- More lipophilic than Morphine- crosses the blood-brain barrier faster
- Metabolized through the liver
- Sedation effects reversed with Narcan
- If given in conjunction with a benzodiazepine a smaller dose should be used
- Fentanyl has a very rapid (30sec.-1min.) onset of action and it has is a relatively short (2-4 hours) half-life which makes it an excellent drug for short procedures.
- Suggested Dose:
25-50mcg titrated over at least 1 min, every 5 minutes until analgesia is achieved.May administer up to 500mcg/4hrs
- The average patient usually requires 50-100mcg.
- Fentanyl has an immediate response and provides excellent analgesia
- The half-life is 2-4 hours, but patients should not do any activities that require fine motor or cognition skills (i.e. driving, cooking)
- Rapid IV administration can lead to a rigid chest wall and difficulty breathing. This effect may be reversed with Naloxone (Narcan) or may require a depolarizing muscle relaxant and intubation
Nursing Considerations:
- Fentanyl does not trigger release of histamines as both Morphine and Meperidine can, which allows for increased cardiovascular stability
- Fentanyl is considered to be 100 times more potent than Morphine
- It has a high affinity for fat; therefore prolonged exposure may lead to accumulation of the drug in the fatty tissues, which can increase recovery time.
- The nurse must be aware that the respiratory depressant effect of the drug may last longer than the analgesic effect
- At high doses, Fentanyl can have a “double peak” effect, where there is a risk of re-sedation and respiratory depression 30-60 minutes after the last dose from recirculation of the medication, which has sequestered in the muscles
- A side effect of Fentanyl that is occasionally seen is muscle rigidity. If this happens, the patient’s respiratory muscles can be paralyzed and the patient may have to be manually ventilated, which can be very difficult
Side effects:
- Respiratory depression
- Hypotension
- Nausea & vomiting
- Urinary retention
- Dizziness and mental clouding
MORPHINE (Morphine Sulphate
- Hypotension, a common adverse effect, is felt to be caused through the direct effect of smooth muscle vasodilation and the indirect vasodilatation effects of histamine release
- Patients standing for the first time should be assisted because dizziness is common
- Flushed skin, sweating, pruritus, and urticaria at the site of injection can also occur due to histamine release
- Stimulation of the emetic chemoreceptors in the medulla frequently causes nausea and vomiting
- Benadryl may be ordered to counter the effects of the histamine release
Suggested dose (0.1mg/kg):
Usual: 2-10mg IV over 5 min., may repeat at 5 min intervals in
increments of 2-5mg.
Nursing Considerations:
- Contraindicated in patients with bronchial asthma, respiratory depression, or hypersensitivity
- Poorly soluble in lipids – limited access through blood-brain barrier
- Has a relatively slow onset &long duration=limited use for conscious / procedural sedation
Suggested dose:
2-10mg IV (0.1mg/kg) over at least 5 minutes may repeat at 5 min intervals in increments of 2-5mg.
Side effects:
- Bradycardia or tachycardia
- Hypotension-postural
- Respiratory depression
- Circulatory depression
- Nausea & vomiting
- DEMEROL (Meperidine)
- Convulsions in humans have been attributed to metabolites from the liver’s conversion of Meperidine to Normeperidine (a potent CNS stimulant) after large doses of Meperidine
- Is a synthetic opioid analgesic
- It is 1/10th as potent as Morphine
- It has a rapid onset and short duration of action due to its lipid solubility
Suggested dose:
10-20mg (0.5-2mg/kg) given over at least 1 minute, titrated every 6-10 minutes until analgesia achieved
Nursing Considerations:
- Use with MAO inhibitors can cause CNS excitation or depression that can be severe or even fatal; therefore administration of Meperidine is contraindicated in patients who have taken MAO inhibitors within the past 14 days
- Meperidine also has a vagolytic effect and changes in heart rate may be pronounced, therefore it must be given with extreme caution to patients with history of supraventricular tachycardia.
- Doses of 75 to 100 mg of Meperidine are considered equivalent to 10 mg of Morphine
Side effects:
- Patient should be supine during injection and observed closely
- Use with caution in patients with cranial injuries, respiratory insufficiency, convulsive disorders, cardiac arrhythmias, or hypersensitivity
- Respiratory depression
- Cardiovascular depression
- Euphoria
REMIFENTANYL (Ultiva)
*****MUST BE ADMINISTERED BY THE PHYSICIAN BY ALL ROUTES
- Narcotic analgesic
- Used an analgesic adjunct for procedures requiring conscious analgesia
Suggested Dose:
1mcg/kg bolus, followed by 0.1mcg/kg/minute infusion titrated to desired effect
Nursing Considerations:
- Has an immediate onset of action and a rapid cessation of effect
- Resuscitation equipment must be readily available
- Antidote: Naloxone (Narcan)
- Is not eliminated by the liver or kidney
Side effects:
- Skeletal and thoracic muscle rigidity, especially with higher doses
- Respiratory depression
- Bradycardia or tachycardia
- Hypotension
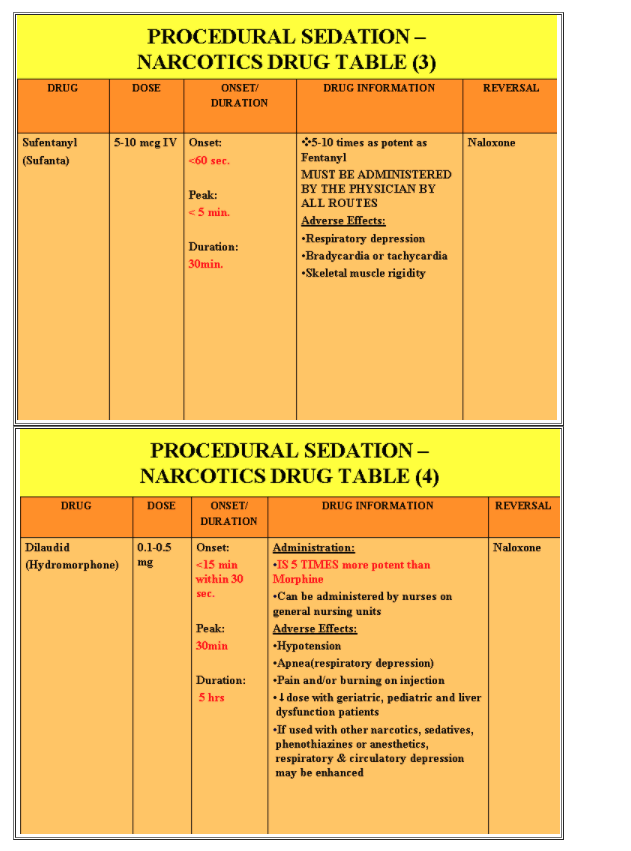
SUFENTANYL (Sufenta)
- ****MUST BE ADMINISTERED BY THE PHYSICIAN BY ALL ROUTES
- 5-10 times as potent as Fentanyl
Suggested dose:
5-10mcg IV
Side effects:
- Respiratory depression
- Bradycardia or tachycardia
- Skeletal muscle rigidity
- Nausea & vomiting
- Urinary retention
- Dizziness and mental clouding
DILAUDID (Hydromorphone)
****IS 5 TIMES MORE POTENT THAN MORPHINE!!!
- Used for symptomatic relief of severe pain.
- May be administered by nurses on general nursing units
- Dilute 2mg(1cc) vial with 9ml NS or SW to make 0.2mg/ml concentration
- Use in caution in patients with respiratory insufficiency, cardiac arrhythmias, convulsive disorders or cranial injuries
*Reduce doses with geriatric, pediatric, debilitated, hepatic dysfunction patients, and those on other CNS depressants. Titrate to desired therapeutic effect
Suggested dose:
IV Direct 0.1-0.5mg given over at least 2-3 min., titrated every 6-10 min. Usual
max. 2mg /hr
NARCOTIC REVERSAL AGENT
NALOXONE (Narcan)
- A pure narcotic antagonist
- Used to reverse narcotic depression induced by opioids (natural and synthetic)
- The dose may need to be repeated if resedation occurs.
- Suggested Dose:
- 0.4- 2.0mg IV Q2-3 min PRN
- It competes for the receptor sites thereby reversing the effect of the narcotic
- It is important to note that all opioid effects are reversed in parallel
- This means that rapid injections of Naloxone not only reverse sedation and respiratory depression, but analgesia as well
- The patient must be closely monitored fro re-sedation (recommended for 120 min after receiving the last dose of IV reversal agent
Nursing Considerations:
- This sudden unmasking of pain may result in significant sympathetic and cardiovascular stimulation, which in turn can cause hypertension, stroke, tachycardia, arrhythmias, pulmonary edema, congestive heart failure, and cardiac arrest.
- Use with caution in patients who have received potentially cardio toxic drugs or who have pre-existing cardiac disease: hypo/hypertension, v-tach or fibrillation
- Since duration of action of narcotic agent may exceed that of Naloxone (Narcan), repeated doses or administration of Naloxone (Narcan) via IV infusion may be required
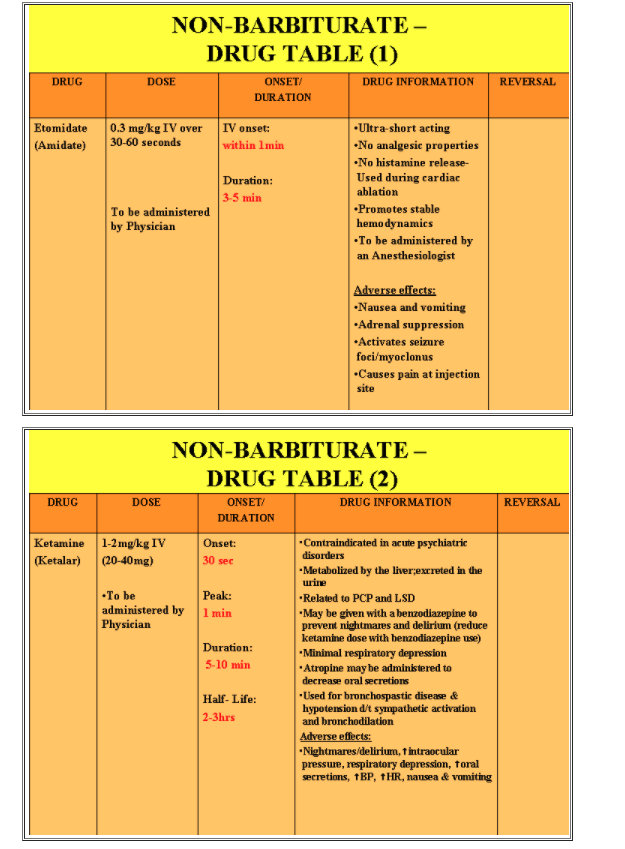
NON-BARBITURATES
ETOMIDATE (Amidate)
- Ultra-short acting non-barbiturate
- MUST BE ADMINISTERED BY A PHYSICIAN
- Can be used during cardiac ablation procedures because it does not cause histamine release
Suggested dose:
0. 3mg/kg IV
KETAMINE (Ketalar)
***MUST BE ADMINISTERED BY A PHYSICIAN
- A non-barbiturate dissociative anesthetic agent with analgesic properties
- Is related to LSD and PCP-can cause vivid dreams and delirium (incidence is less in children and in adults with a concomitant administration of a benzodiazepine)
- Causes bronchodilation-valuable for asthmatic patients
- May eliminate bronchospasm, but maintain protective reflexes in non-intubated patients
- Causes salivation
- Suggested dose:
1-2mg/kg IV (20-40mg)
ANTIEMETICS
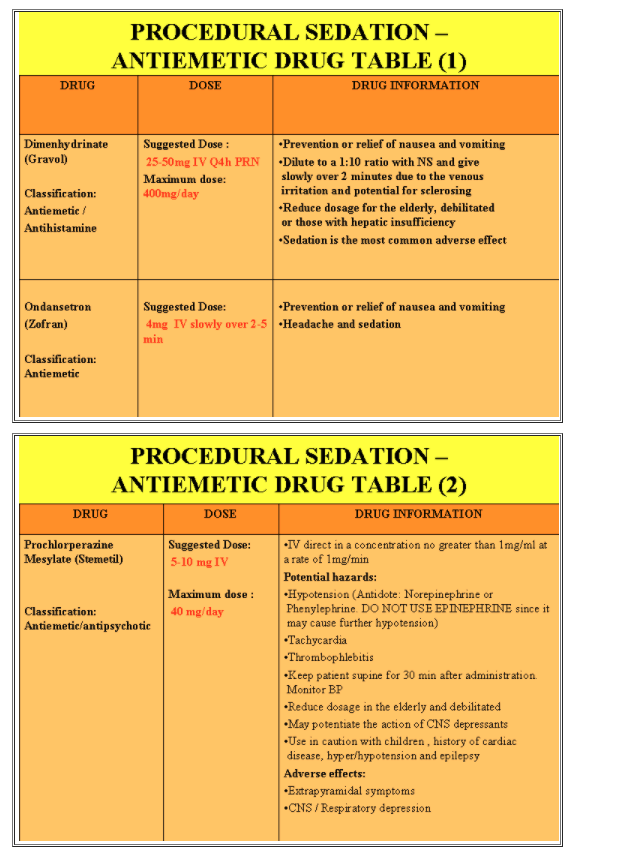
DIMENHYDRINATE (Gravol)
Classification:
Antiemetic, Antihistamine
- Prevention or relief of nausea and vomiting
Suggested dose:
25-50 mg IV Q 4h PRN. Maximum daily dose = 400mg/day
Nursing Considerations:
- Dilute to a 1:10 ratio with NS and give slowly over 2 minutes due to the venous irritation and potential for sclerosing
- Reduce dosage for the elderly, debilitated or those with hepatic insufficiency
- Sedation is the most common adverse effect
- Often given with Dexamethasone 4mg IV to help N&V
ONDANSETRON (Zofran)
Classification:
Antiemetic
- Prevention or relief of nausea and vomiting
Suggested dose:
4 mg IV slowly over 2 –5 min.
Nursing Considerations:
- Anti-emetic effects maximized when combined with Dexamethasone (Decadron) 8mg IV
Adverse effects:
- Headache and sedation
- PROCHLORPERAZINE MESYLATE (Stemetil)Classification:
- Antiemetic, Antipsychotic
- Prevention or relief of nausea and vomiting
Suggested dose:
5-10 mg IV. Maximum dose = 40mg /day
Nursing Considerations:
- IV direct in a concentration no greater than 1mg/ml at a rate of 1mg/min
Potential hazards:
- Hypotension (Antidote: Norepinephrine or Phenylephrine. DO NOT USE EPINEPHRINE since it may cause further hypotension)
- Tachycardia
- Thrombophlebitis
- Keep patient supine for 30 min after administration. Monitor BP
- Reduce dosage in the elderly and debilitated
- May potentiate the action of CNS depressants
- Use in caution with children, history of cardiac disease, hyper/hypotension and epilepsy
Adverse effects:
- Extrapyramidal symptoms
- CNS / Respiratory depression
METOCHLOPRAMIDE HCL (Maxeran, Reglan)
Classification:
- Upper GI tract motility modifier
Suggested dose:
10 mg IV slowly over at least 1-2 min
Nursing Considerations:
- Dopamine antagonist
- Contraindicated in patients with Epilepsy and Parkinsons
- Inconsistent antiemetic effects
Adverse effects:
- Parkinsonism and/or other extrapyramidal effects with high doses and/or in renal impairment
- Contraindicated in patients with Epilepsy and Parkinsons
- Inconsistent antiemetic effects
RANITIDINE (Zantac)Classification:
- Histamine H2 receptor antagonist
Suggested dose:
50 mg IV Q8h. Diluted to 20 ml administered over a least 5 min.
Nursing Considerations:
- Bradycardia and nausea if injected too rapidly
- In severe renal impairment the dose should be decreased by 50%
- Potential for pain, irritation and urticaria with injection
SEDATIVE / HYPNOTIC AGENTS
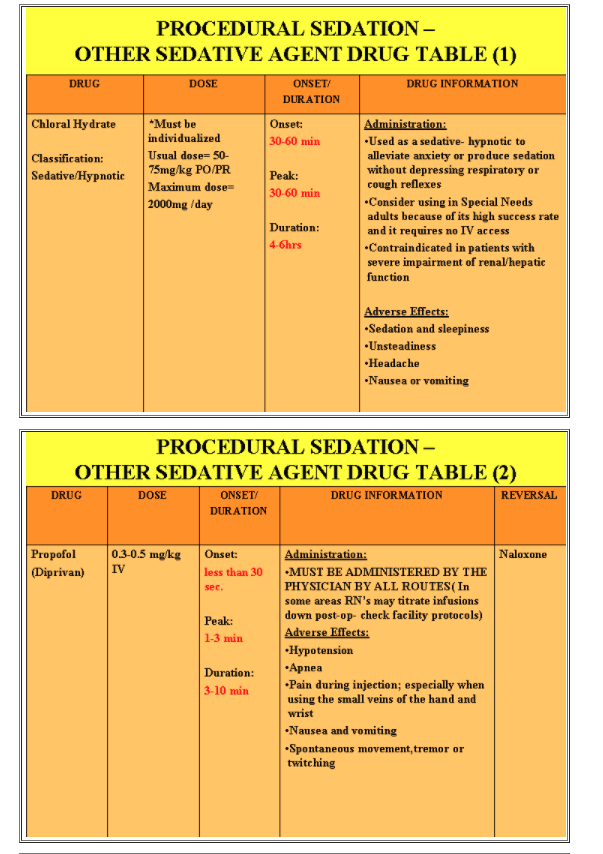
PROPOFOL (Diprivan)
- ***MUST BE ADMINISTERED BY THE PHYSICIAN BY ALL ROUTES (In some areas RN’s may titrate infusions down post-
- op- check facility protocols)
- Used as a sedative / hypnotic agent
- Has no analgesic properties
- Low incidence of nausea and vomiting
- **** Not pharmacologically reversible
- Sense of well-being
- Common induction agent
Suggested dose:
0. 3-0.5 mg/kg IV
Nursing Considerations:
- Patients should be continually monitored for early signs of hypotension or bradycardia
- Effects will be potentiated in patients receiving CNS depressants
- Onset of anesthesia usually occurs within 30 seconds of bolus injection
- Use with caution in patients with hypovolemia, severe cardiac or respiratory disease or history of seizures
- Side effects:
- Hypotension
- Apnea
- Pain during injection; especially when using the small veins of the hand and wrist
- Nausea and vomiting
- Spontaneous movement, tremor or twitching
CHLORAL HYDRATE
Classification:
Sedative / Hypnotic
- Used as a sedative hypnotic to alleviate anxiety or produce sedation without depressing respiratory or cough reflexes
Suggested dose:
- Must be individualized
- Usual dose= 50-75 mg/kg PO/PR
- Maximum dose= 2000 mg /day
Nursing Considerations:
- Consider using in Special Needs adults because of its high success rate and it requires no IV access
- Contraindicated in patients with severe impairment of renal/hepatic function
Adverse Effects:
- Sedation and sleepiness
- Unsteadiness
- Headache
- Nausea or vomiting
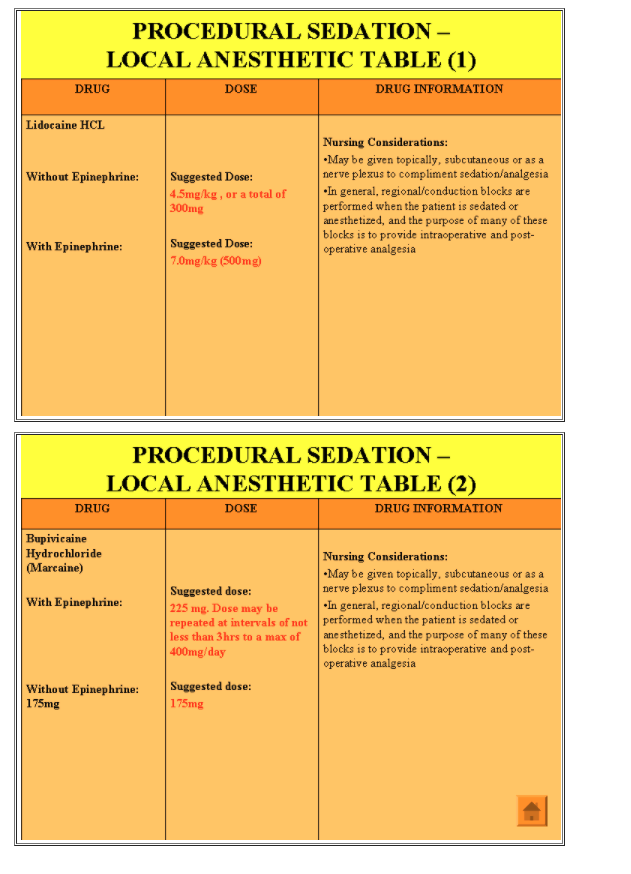
LOCAL ANESTHETICS
- May be given topically, subcutaneous or as a nerve plexus block to compliment sedation/analgesia
- In general, regional/conduction blocks are performed when the patient is sedated or anesthetized, and the purpose of many of these blocks is to provide interoperative and post-operative analgesia.
TOPICAL:
- Topical or surface application to the skin or mucous membrane produces a sensory block
- Is used in adults & pediatric populations
- Available in different preparations:
- 1) Eye drops
- 2) Sprays
- 3) Solutions
- 4) Ointments
- 5) Jellies
Common sites for topical anesthesia include:
- Cornea/conjunctiva
- Tympanic membrane
- Urethra
- Upper airways (mouth, nose, throat, larynx, vocal cords and trachea)
- Backs of hands – pre IV insertion
Nursing considerations related to location are:
Eye
•If the blink reflex is absent; an eye patch may be necessary to prevent a corneal abrasion
Throat
•This may result in loss of protective reflexes (gag, cough)
•Monitor for signs of ineffective airway clearance, and the return of these reflexes
Nasopharynx
•This is a highly vascular area, which allows for rapid absorption of the local anaesthetic (5-10 min), but also the risk of systemic uptake and toxicity
LOCAL INFILTRATION
- Involves injection into the subcutaneous tissue to produce a block of the sensory nerve branches
- Used in adult and pediatric populations
- Used in procedures for biopsies, incision and drainage of abscesses, removal of small cysts and tumors, some dental work and intravascular catheter insertion
- Bupivicaine (Marcaine) is frequently given at surgical incision sites to promote postoperative analgesia
CONDUCTION / NERVE BLOCKS
- Peripheral nerve blockade is achieved by injecting a local anaesthetic into an area close to major nerve groups supplying the surgical site
- Causes sensory and motor nerve blockade
- LOCAL ANESTHETICS-
- SYSTEMIC TOXICITY
- The original site of administration may be on the skin or into the subcutaneous tissue; local anesthetics can migrate into systemic circulation and produce toxicity.
- Higher risk in children than with adults
- Signs of toxicity occur on a continuum from early to late stages of toxicity.
- These signs are:
- Circum-oral and tongue numbness
- Lightheadedness
- Tinnitus
- Visual disturbances
- Muscular twitching, convulsions
- Unconsciousness
- Coma
- Respiratory arrest, then cardiovascular collapse
- CENTRAL NERVOUS SYSTEM:
- Metallic taste in mouth
- Numbness of tongue
- Ringing in ears
- Slurred speech
- Confusion
- Nausea
- Excitation
- Muscle twitching
- Seizures
- Lightheadedness
- Decreased level of consciousness
- Dysrhythmias
- RESPIRATORY AND CARDIOVASCULAR SYSTEMS:
- Difficulty breathing
- Apnea
- Respiratory depression or arrest
- Increased PR interval and QRS complex duration
- Decreased cardiac output
- Hypotension
- Arrhythmias-sinus bradycardia, AV block, asystole
- LOCAL ANESTHETICS & DOSAGES
- LIDOCAINE HYDROCHLORIDE (Lidocaine)
- Suggested dose:
- With Epinephrine: 7.0 mg/kg (500mg)
- Without Epinephrine: 4.5mg/kg or a total of 300mg
- BUPIVICAINE HYDROCHLORIDE (Marcaine)
- Suggested dose:
- With Epinephrine: 225 mg. Dose may be repeated at intervals of not less than 3hrs to a max of 400mg/day
- Without Epinephrine: 175mg
- TYPES OF REACTIONS:1) MILD
- Signs and symptoms:
- Anxiety
- Restlessnes
- Numbness of tongue
- Tinnitus
- Lightheadedness
- Drowsiness
- Disorientation
- Nausea and vomiting
- Increased PR interval and QRS duration
- Decreased BP and cardiac output
- Dysrhythmias
- Treatment:
- Document and report baseline symptoms
- Monitor for the progression or worsening of symptoms
- Definitive treatment may not be necessary
- 2) SEVERE
- Signs and symptoms:
- Muscle twitching
- Tremors of the face and extremities
- Generalized seizures
- Unconsciousness
- Respiratory arrest
- Markedly reduced BP and cardiac output
- Dramatic increase in PR interval and QRS duration
- Arrhythmias (AV block, bradycardia, asystole)
- Treatment:
- Seizure activity-IV barbiturates/ benzodiazepines
- Respiratory problems-oxygen, airway management and/or mechanical ventilation
- Hypotension-IV fluids, vasopressors
- Arrhythmias-IV antiarrhythmics, defibrillation/cardioversion
- ALERT!!!There are variations in drug doses and pharmacokinetics…so check with your pharmacy manual for institutional drug dosages and administration practices
Drug Tables #
REFERENCES
- American Diabetes Association website: http://www.diabetes.org/home.jsp . Diabetes Forecast 2008 Resource Guide
- American Heart Association website: www.americanheart.org . 2008-Cardiac Medications At- a- Glance chart. Reprinted with permission
- American Society of Anesthesiologists. (2001). (Practice guidelines for sedation and analgesia by non-anesthesiologists. An updated report by the American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non-Anesthesiologists., 2001) and analgesia, 1-74
- BC Cancer Agency. (2002) Conscious Sedation Learning Module.
- Canadian Society of gastroenterology Nurses and Associates (2001). Guidelines for the Care of patients receiving conscious sedation.
- Chari, R. et al. (? January 19). Drugs for conscious sedation and neuromuscular paralysis: Guidelines and protocols for use in the emergency department. Emergency Medicine Reports, (2)
- Kost, M., (2004). Moderate Sedation: Core competencies for practice, 2nd edition Permission obtained for 14 pages only including 2 Figures and 5 Tables
- Kost, M., (1998). Manual of conscious sedation, W.B. Saunders CO. Saunders Elsevier, St. Louis, MO
- Lions Gate Hospital (2001). Conscious Sedation & Nursing Implications Educational module
- MacFarlane (2000) BCIT. Peri-Procedural Nursing care of patients receiving conscious sedation
- Saint Mary’s Hospital.(2001) Ambulatory Care Conscious Sedation Self –Learning Module for registered Nurses.1-59.Material used with permission.
- Shields, R (1997). A comprehensive review of sedative and analgesic agents. Critical Care Clinics of North America. 9(3), 281-288.
- University of Utah Center for Pain Medicinehttp://library.med.utah.edu/pain_center/education/outlines/local_anes.html
- Vancouver Community College Continuing Education (2002). Conscious Sedation (HLTH 1182) Nursing Management: Pre-procedural to Post-operative Teaching. 1-59 Material used from Pages 4,18 &19 with permission.
- Vancouver General Hospital –Pharmaceutical Sciences Parenteral Drug Therapy Manual