Description #
This module is aimed at providing information on the electrophysiology of the heart, basic dysrhythmias and their appropriate responses and treatments.
Learning Objectives #
At the end of the session the nurse must be able to :
a) Describe the electrophysiology of the heart
b) Identify basic dysrhythmias
c) Describe the appropriate response to these dysrhythmias
d) Be familiar with common electrolyte imbalances and cardiac medications and their
effects on the cardiac electrophysiology
e) Be familiar with the different types of cardiac pacemakers
ANATOMY & PHYSIOLOGY REVIEW
HEART WALL
Is made up of 3 layers:
1)Epicardium-outermost layer
2)Myocardium-middle and thickest layer, this layer contracts with each heartbeat
3)Endocardium- innermost layer consisting of thin layer of endothelial tissue that lines heart valves and
chambers
Pericardium
· A fluid filled sac that envelops the heart and acts as a tough, protective covering.
· Consists of fibrous pericardium (tough, white, fibrous tissue), and serous pericardium (two layers-parietal &
visceral)
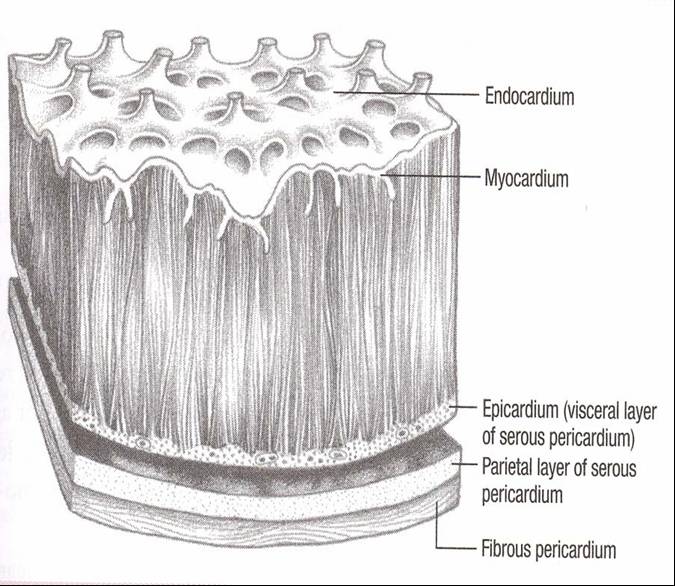
Lippincott Williams & Wilkins(2005) ECG INTERPRETATION: A 2-in-1 reference for Nurses p.3
EXTERIOR OF THE HEART
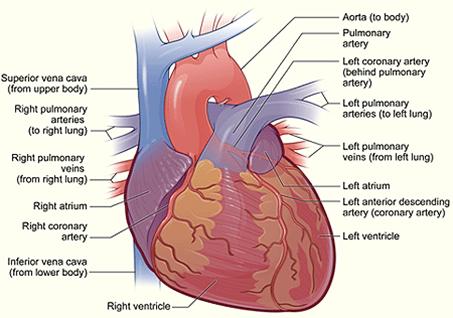
Source: The National Heart, Lung, and Blood Institute
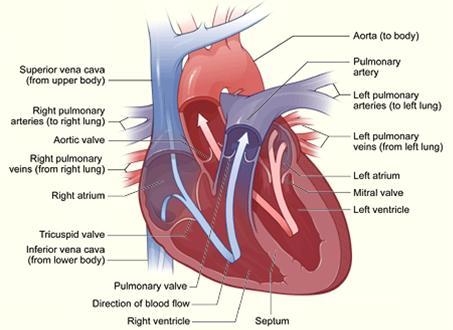
HEART CHAMBERS
- Are four chambers- 2 atria & 2 ventricles
- The right and left atria serve as volume reservoirs for blood being sent into the ventricles
- The right atrium receives deoxygenated blood returning from the body
- The left atrium receives oxygenated blood from the lungs
- The right and left ventricles serve as the pumping chambers of the heart.
- The right ventricle receives deoxygenated blood from the right atrium and pumps it to the lungs
- The left ventricle receives oxygenated blood from the left atrium and pumps it through the aorta
BLOOD FLOW
- Blood returns to heart through the inferior vena cava and superior vena cava → right atrium → right ventricle → pulmonary arteries to lungs → pulmonary veins → left atrium → left ventricle → aorta to rest of the body
- The main coronary arteries lie on the surface of the heart (epicardium)
- The heart receives its blood supply almost entirely through the coronary arteries
- – Right Coronary Artery (RCA)
- – Left Main –Coronary Artery which has 2 major branches known as Left Anterior Descending (LAD) and Left Circumflex Artery (LCA)
- The RCA supplies blood to the right atrium, right ventricle, and inferior wall of the left ventricle
- The LAD supplies blood to the anterior wall of the ventricular septum & the apex
- The Left Circumflex supplies blood to the left atrium, the lateral and posterior wall of the left ventricle
- Blood flow through the coronary arteries occurs during ventricular relaxation or diastole
THE HEART CONTAINS:
Four valves- 2 atrioventricular (AV) valves (Tricuspid and Mitral) and 2 semilunar valves (Pulmonic and Aortic)
Main function is to keep blood flowing through the heart in a forward direction
AV Valves:
-Tricuspid valve separates the right atrium from the right ventricle-Mitral valve separates the left atrium from the left ventricle
-The closure of the AV valves associated with S1
Semilunar Valves:
-The aortic valve lies between the left ventricle and the aorta
-The pulmonic valve lies between the right ventricle and the pulmonary artery
-The closure of the pulmonic valve associated with S2
Heart Valves-Educational material #
Blood Flow-Educational material #
Heart Chambers-Educational material #
Heart Wall-Educational material #
Basic Electrophysiology #
Dubin, 1996, p. 29
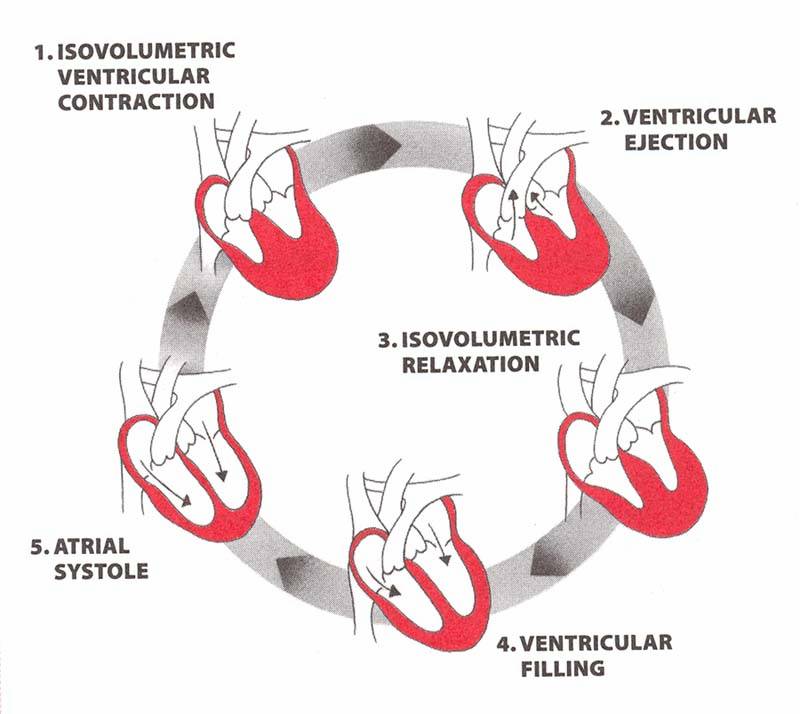
Lippincott Williams & Wilkins(2005) ECG INTERPRETATION: A 2-in-1 reference for Nurses p.10
Consists of ventricular diastole, or relaxation, and ventricular systole, or contraction
Ventricular diastole:
Blood flows from atria into relaxed ventricles
About 70-75% of blood flows passively from atria into ventricles
Atrial contraction (atrial kick) contributes another 25-30% to ventricular filling
Ventricular systole:
Ventricles contract, and blood is ejected into the pulmonic and systemic circulation
Cardiac output:
Measured by multiplying the heart rate times the stroke volume (amount of blood ejected with each ventricular contraction
C.O.=HR x SV
Determined by three factors:
PRELOAD– degree of stretch on muscle fibers when they begin to contract (end
diastolic pressure)
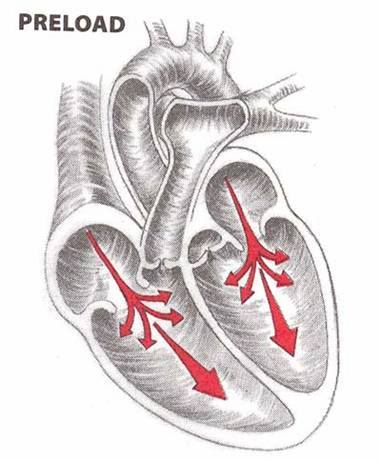
Lippincott Williams & Wilkins(2005) ECG INTERPRETATION: A 2-in-1 reference for Nurses p.11
AFTERLOAD-amount of pressure left ventricle must work against to eject blood during systole
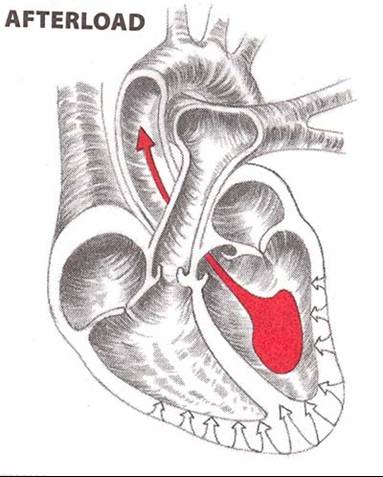
Lippincott Williams & Wilkins(2005) ECG INTERPRETATION: A 2-in-1 reference for Nurses p.11
MYOCARDIAL CONTRACTILITY
- Ventricles ability to contract
- Sympathetic innervation-causes release of norepinephrine, which increases heart rate and accelerates AV node conduction
- Parasympathetic stimulation causes release of acetycholine, which slows heart rate and conduction through AV node
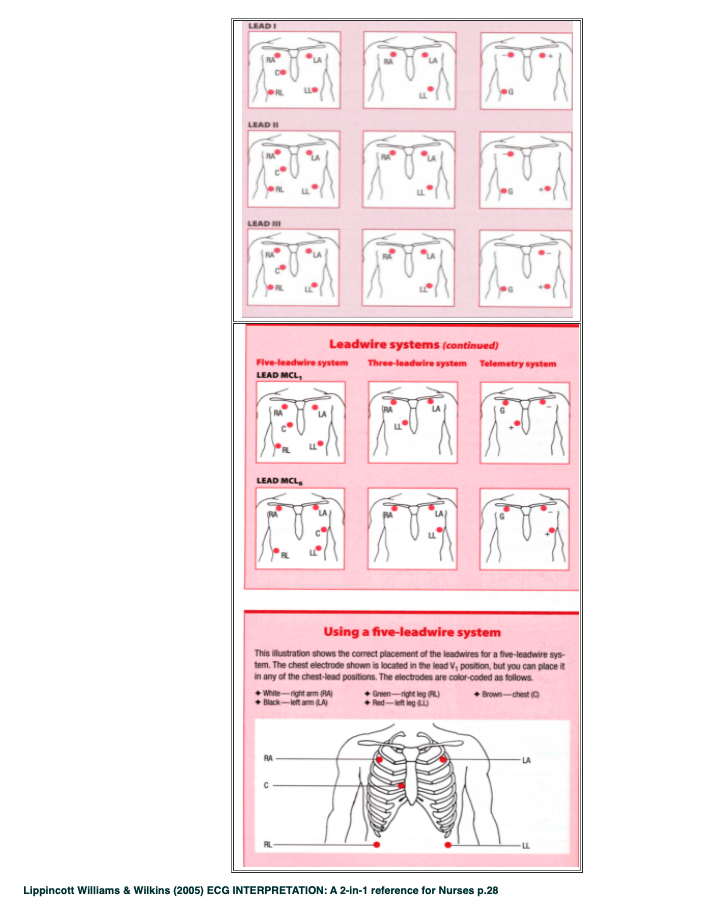
ECG Lead placement #
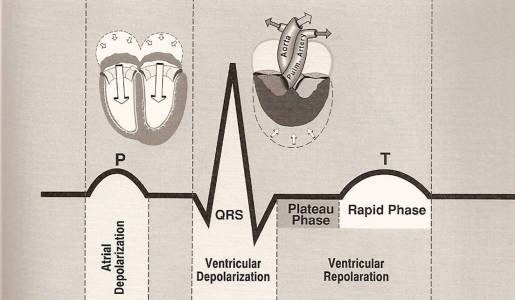
PQRST Complex #
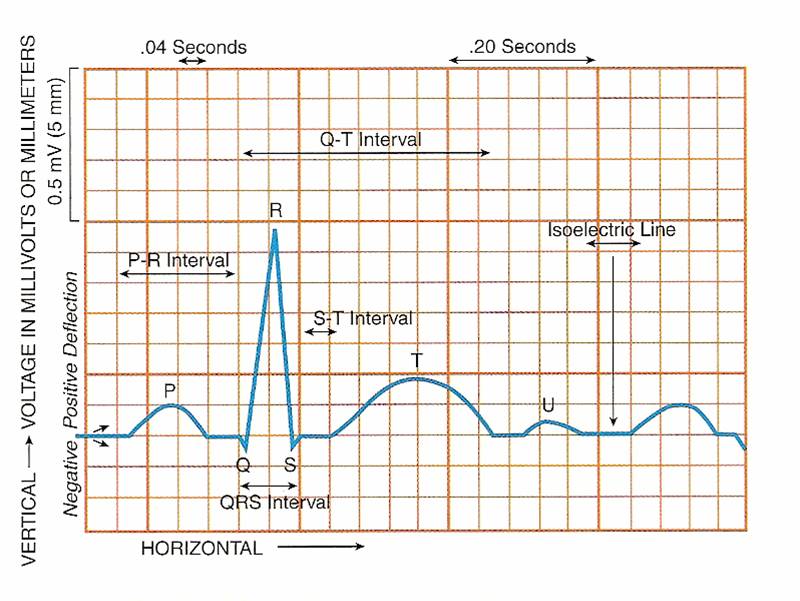
P wave:
- 1st component of a normal ECG
- Represents atrial depolarization
- Usually rounded and upright
- Precedes the QRS complex
- PR interval:Tracks atrial impulse from atrial to AV node (from the onset of atrial depolarization to the onset of ventricular depolarization)
QRS complex:
- Follows the P wave; represents depolarization of ventricles
ST segment:
- Represents end of ventricular depolarization and onset of ventricular repolarization
- Isoelectric
T Wave:
- Represents relative refractory period of polarization or ventricular recovery
- Rounded and smooth
QT intervals:
- Measures time needed for ventricular depolarization and repolarization
- Length varies according to heart rate
U wave:
- Rarely seen
- Upright and rounded
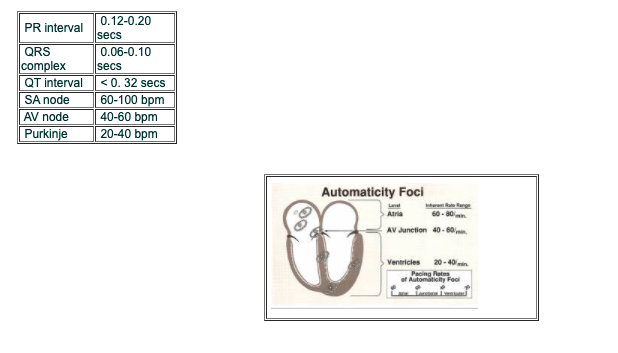
NORMAL VALUES:
PQRST Complex – Educational material #
Conduction Pathway #

Conduction System -Educational material #
Measuring Heart Rate #
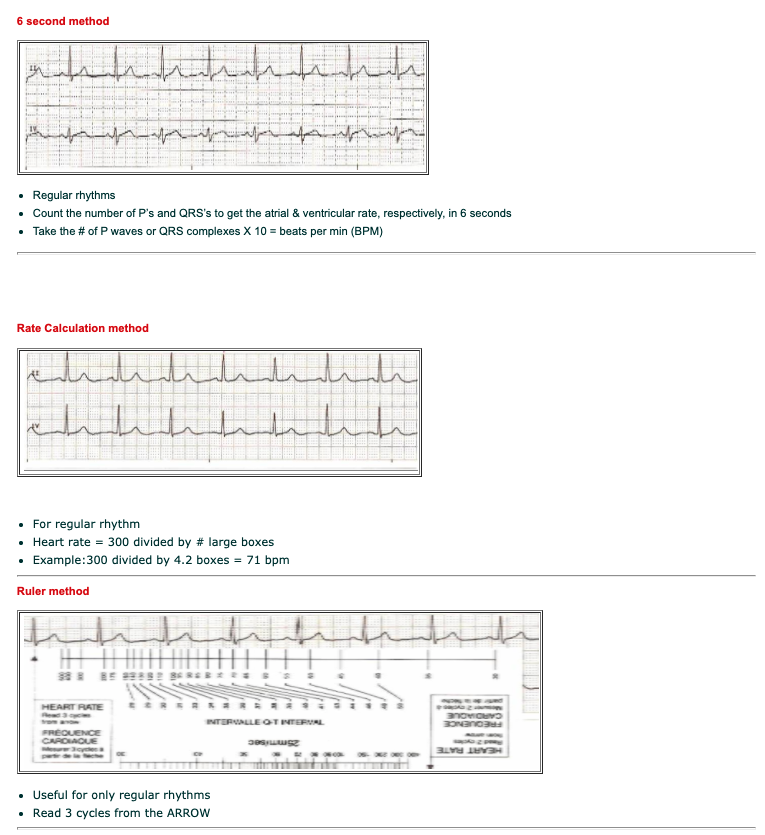
MEASURING HEART RATE
3 methods:
1) 6 second method
2) Rate calculation method
3) Ruler method
Grid Method -Educational material #
#
Six Second Method-Educational material #
#
ECG Paper-Educational material #
#
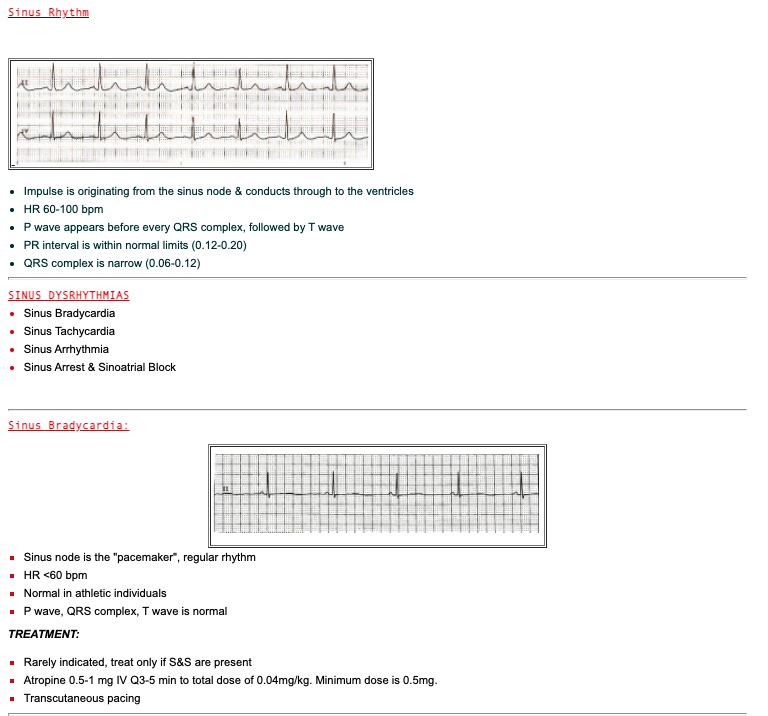
RHYTHM OVERVIEW #
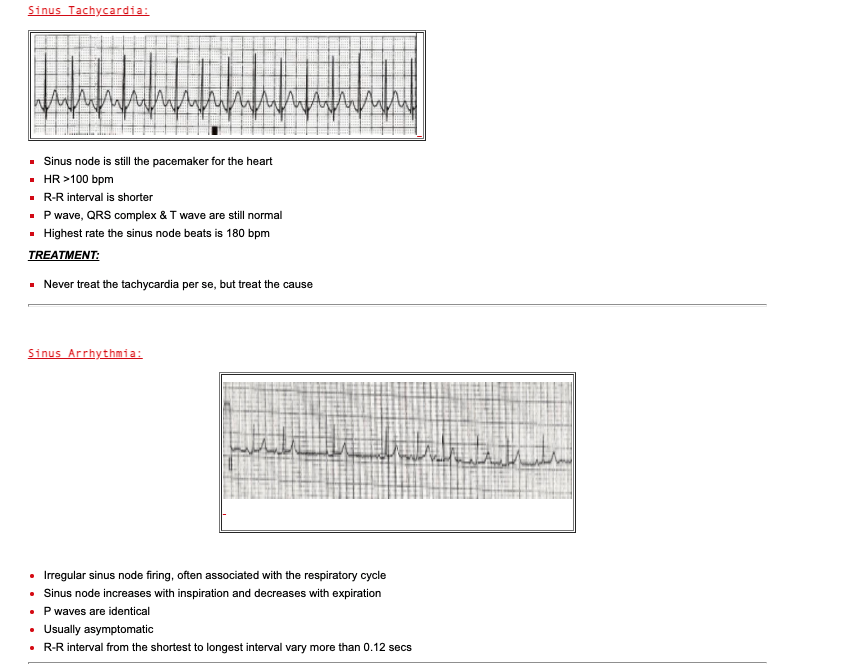
Sinus rhythm (SR)Sinus Tachycardia (ST)
Sinus Bradycardia (SB)
Premature atrial / ventricular contraction (PAC/PVC)
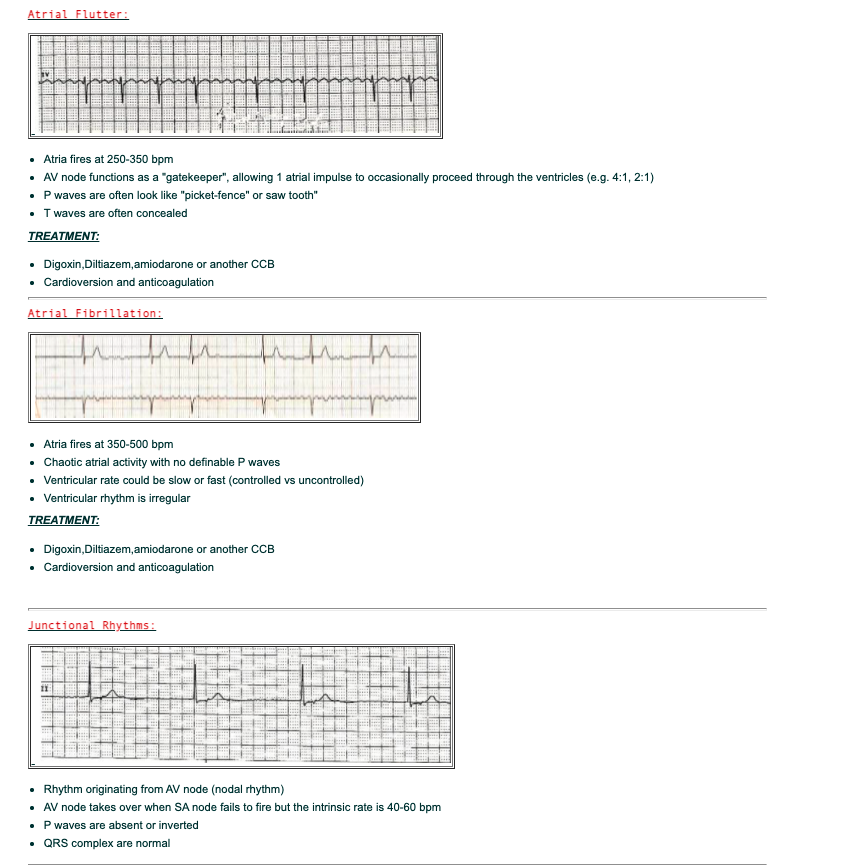
Atrial Flutter/Fibrillation
Junctional Rhythms
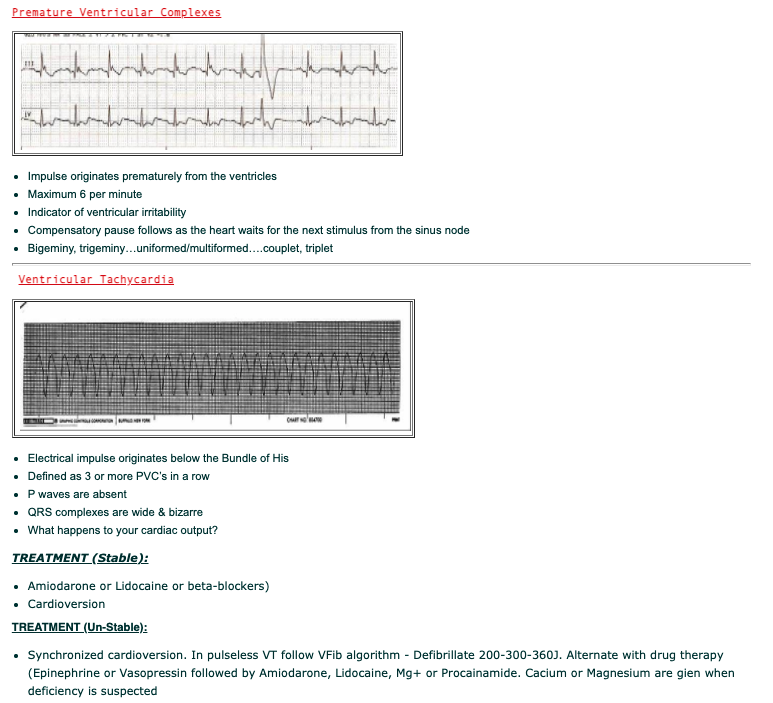
Ventricular Tachycardia (VT)
Ventricular Fibrillation (VFib)
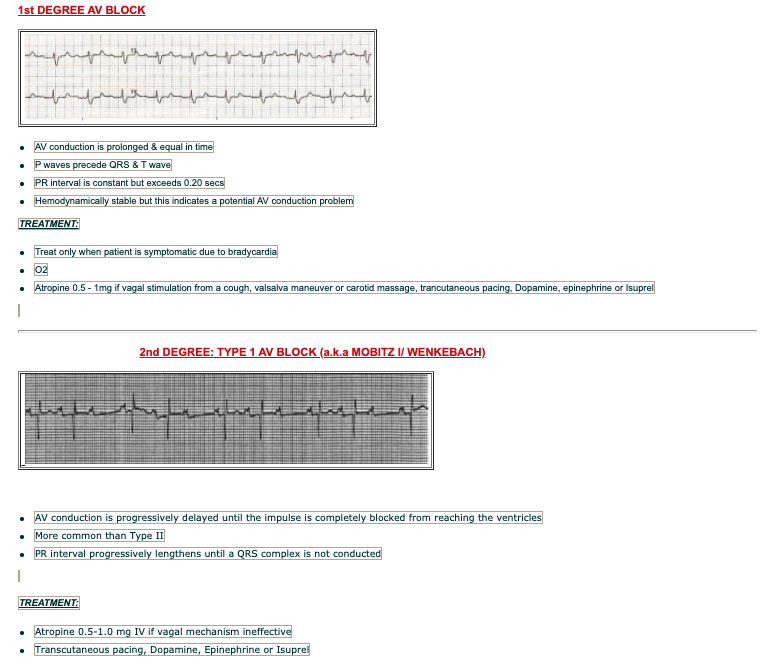
1st degree AV Block
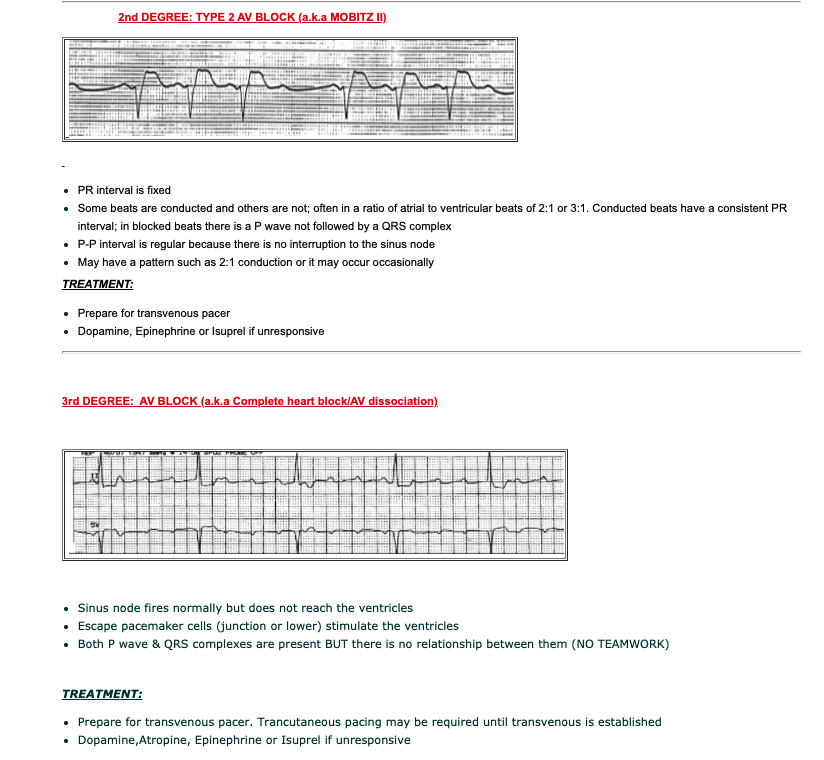
2nd degree AV Block – Type I ( Wenckebach) & Type II (Mobitz II)
3rd degree AV Block
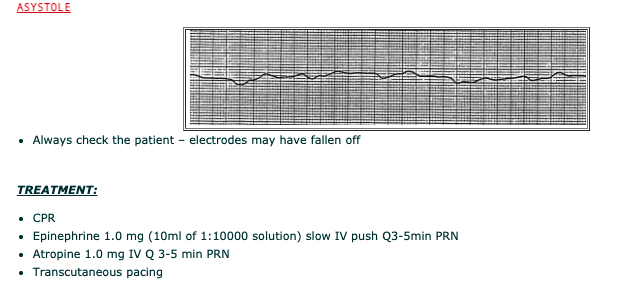
Asystole
STEPS TO ASSESSING ECG RHYTHMS
- Is the rhythm regular or irregular? Fast or slow?
- Determine atrial & ventricular HR
- Are the P waves, QRS complex, & T wave present?
- Determine the PR interval, QRS complex, QT interval?
- Is the ST segment isoelectric, elevated or depressed?
- Is the T wave upright or inverted?
- Interpretation?
QUESTIONS TO CONSIDER:
- What is the hemodynamic significance? Causes?
- What are the nursing actions? Anticipated/expected actions?
Dysrhythmias/Sinus Dysrhythmias #
Atrial Dysrhythmias #
ATRIAL DYSRHYTHMIAS
- PACs
- SVT
- Atrial Flutter
- Atrial Fibrillation

- VENTRICULAR DYSRHYTHMIAS
- PVCs
- VT
- Torsades de Pointes
- V.Fib
ATRIALVENTRICULAR BLOCKS
- 1St degree AV block
- 2nd degree AV block
Type I –(a.ka. Mobitz I / Wenkebach)
Type II (a.k.a.Mobitz II)
- 3rd degree AV block (a.k.a. complete heart block or AV dissociation)
Asystole #
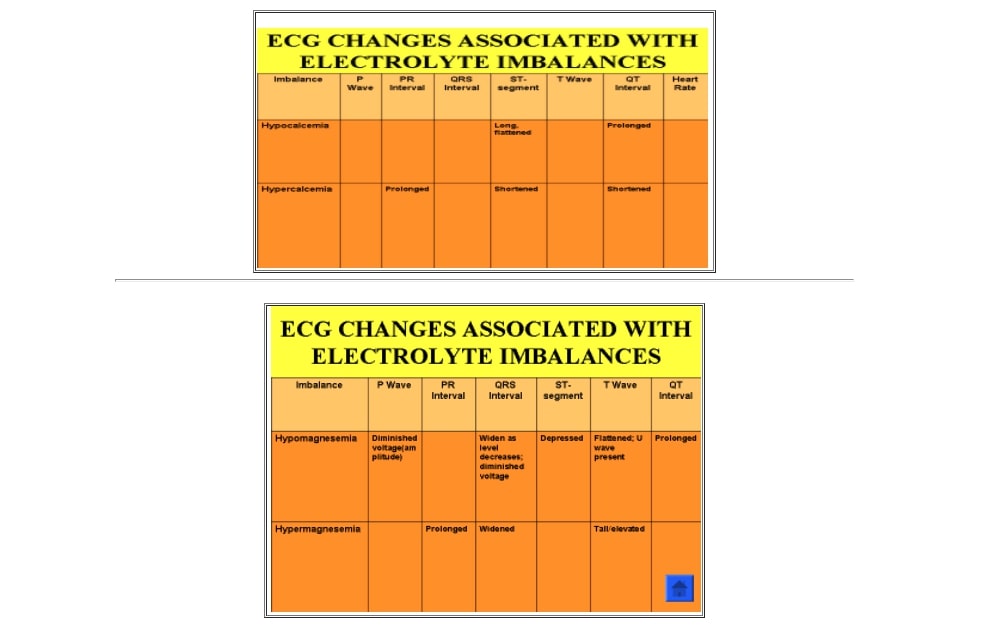
Electrolyte Imbalances #
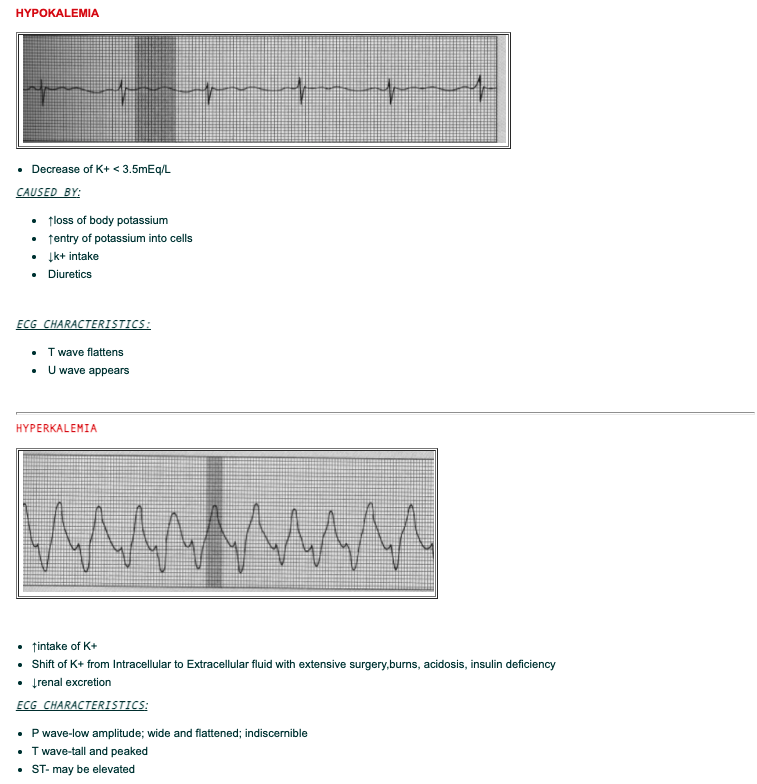
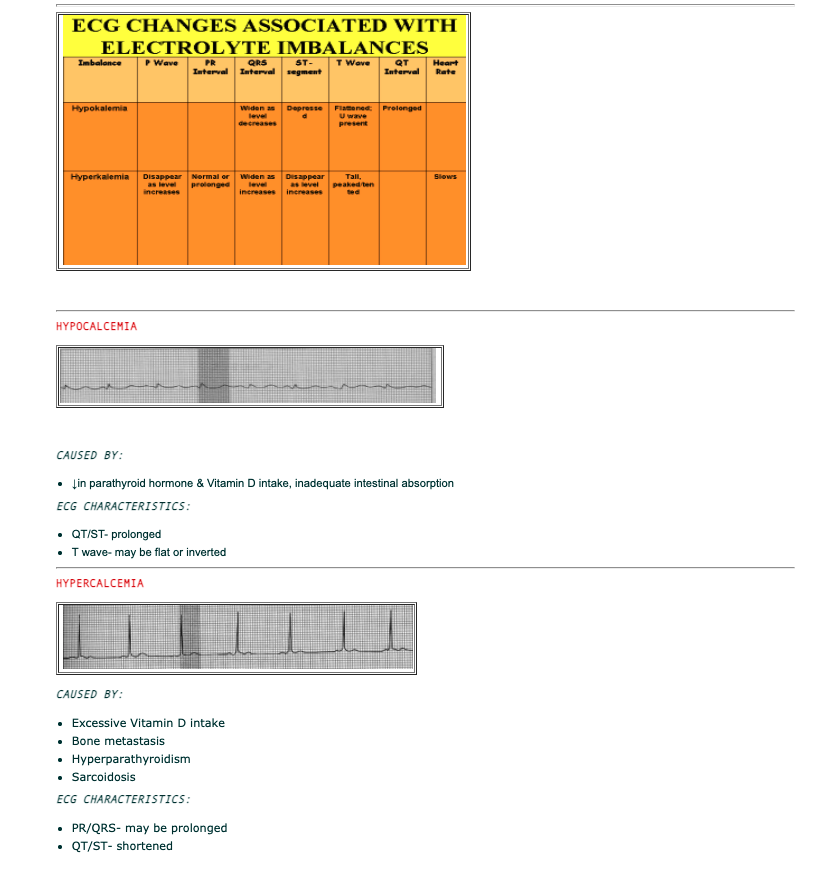
CAUSED BY:
- The normal state of cardiac cell membrane polarization is dependent upon the maintenance of a normal ionic balance across the membranes
- Any changes in the concentration of the following electrolytes (K, Ca, Mg) can cause ECG changes.
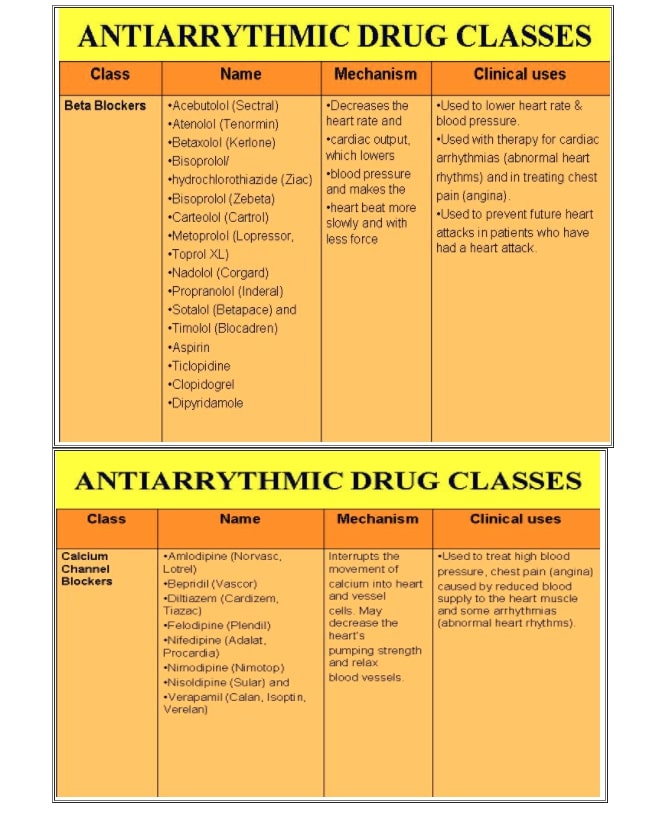
CARDIAC DRUGS
- Classified according to their effect on cell’s electrical activity and their mechanism of action
- Can cause myocardial action changes resulting in characteristic ECG changes
- Divided into 10 major classes
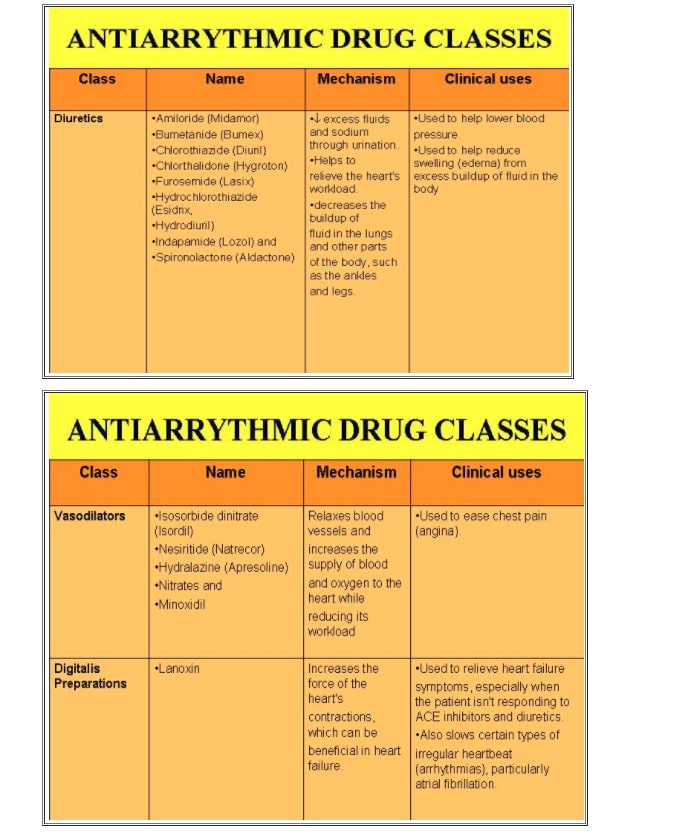
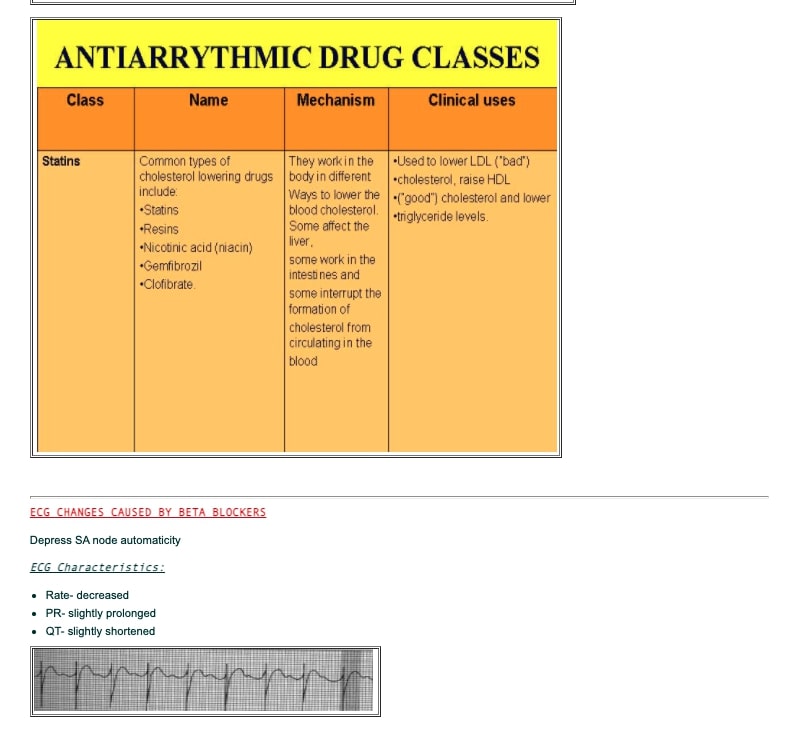
CARDIAC DRUG CLASSIFICATION
There are ten main classes of Cardiac Medications (American Heart Association -AHA):
1)Anticoagulants:
2)Antiplatelet agents
3)Angiotensin-Converting Enzyme (ACE) Inhibitors
4)Angiotensin II Receptor Blockers (or Inhibitors)
5)Beta Blockers
6)Calcium Channel Blockers
7)Diuretics
8)Vasodilators
9)Digitalis Preparations
10)Statins

Procedural Sedation Video of patient scenario for procedures more than 20 minutes in duration.
Procedural Sedation Video of patient scenario for procedures less than 20 minutes in duration.
PACEMAKERS
- Normally have one lead to carry impulses to and from either the right atrium or right ventricle.
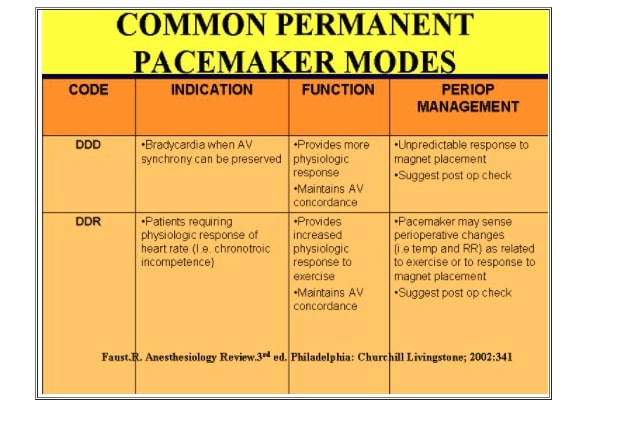
Dual-chamber pacemakers:
- Usually has two leads, one to the right atrium and one to the right ventricle, that can monitor and carry impulses to one or both chambers; these can produce an atrial contraction followed closely by ventricular contraction, thus more naturally resembling the normal activities of the heart
Triple-chamber pacemakers:
- Typically have one lead in the right atrium and one each in the right and left ventricles.
- These pacemakers “resynchronize” the ventricles and may improve the efficiency of the contraction of the heart, improving its blood flow.
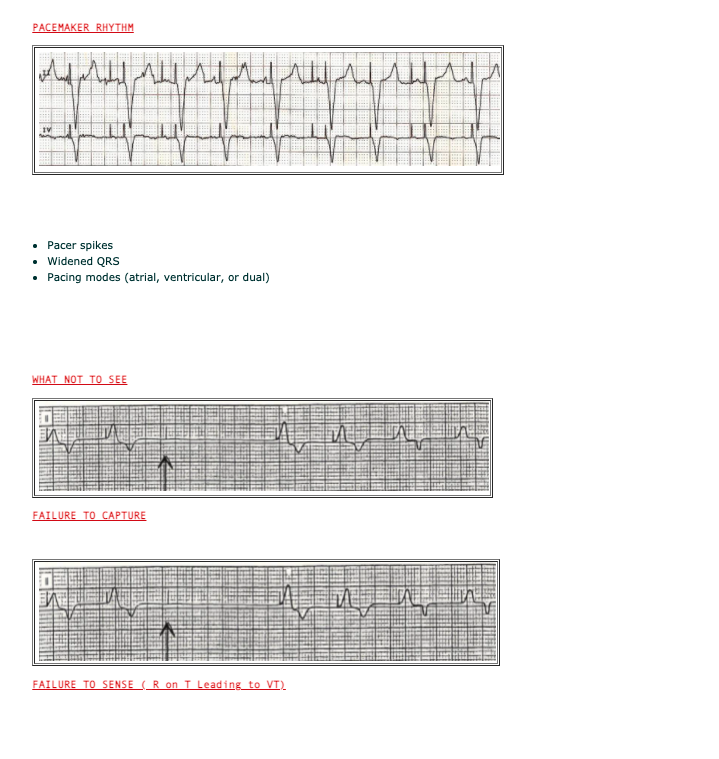
ECG Characteristics:
- Prominent pacemaker spike
- When it stimulates the atria, the spike is followed by a P wave, baseline QRS and T wave
- When the ventricles are stimulated, the spike is followed by a QRS and a T wave
- When the atria and ventricles are both stimulated, the spike is followed by a P wave, then a spike, and then a QRS complex
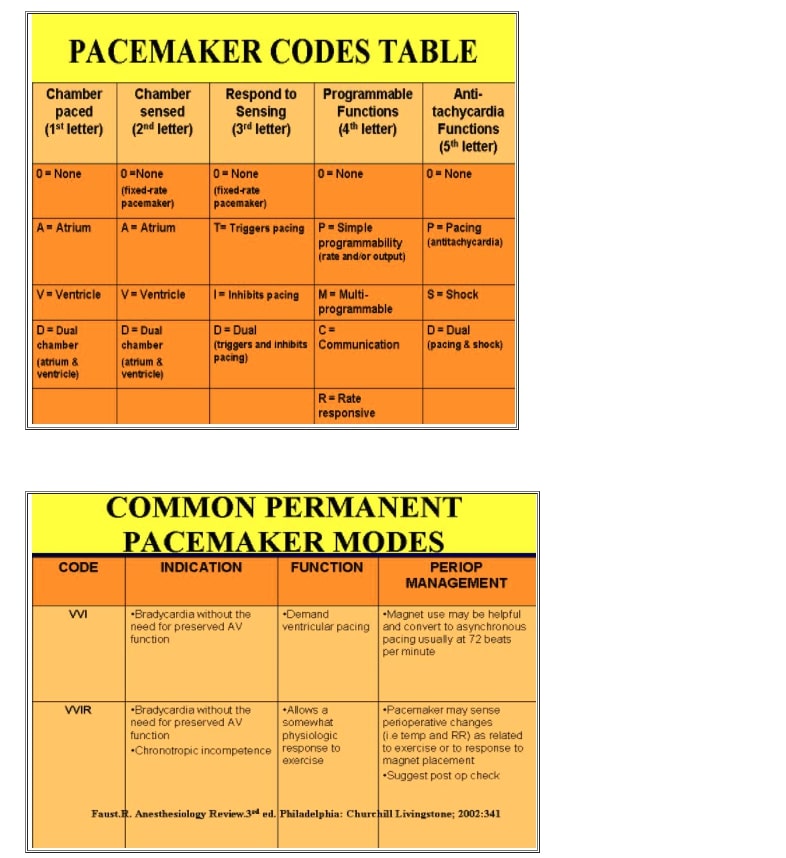
PACEMAKER MODES
- Fixed-Rate (Asynchronous)
- Demand (Synchronous, Noncompetitive)
FIXED RATE PACEMAKERS
- Continuously discharges at a pre-set rate (usually 70-80/min) regardless of the patient’s heart rate
- Simple circuitry reducing the risk of pacemaker failure
- Does not sense pt’s own cardiac rhythm
- Often not used today
DEMAND PACEMAKERS
- Discharges only when the pt’s heart rate drops below the pacemaker’s preset rate
- Can be programmable or nonprogrammable
•Saint Mary’s Hospital.(2001) Ambulatory Care Conscious Sedation Self –Learning Module for registered Nurses.1-59 #
•Vancouver Community College Continuing Education (2002). Conscious Sedation (HLTH 1182) Nursing Management: Pre-procedural to Post-operative Teaching. 1-59
•Vancouver General Hospital –Pharmaceutical Sciences Parenteral Drug Therapy Manual
Video: Six Second Method #
Video: PQRST complex #
Video: ECG Paper #
Video: Grid Method #
Video: 3 Lead Monitor #
Video: 5 Lead Monitor #
$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$
Basic ECG Interpretation additional resources #
#
Basic ECG Interpretation Part 1
Original content developed by: Tina Oye, BSN, RN January 2006
Edited by: Arlene Vanderhoeven, R.N. January 2006
Basic ECG Interpretation Part 2
Original content developed by: Tina Oye, BSN, RN January 2006
Edited by: Arlene Vanderhoeven, R.N. January 2006
Basic ECG Interpretation PART 3
Original content developed by: Tina Oye, BSN, RN January 2006
Edited by: Arlene Vanderhoeven, R.N. January 2006
Basic ECG Interpretation PART 4
Original content developed by: Tina Oye, BSN, RN January 2006
Edited by: Arlene Vanderhoeven, R.N. January 2006